Resuscitation and Emergency Cardiovascular Care Science
With Treatment Recommendations
Part 9: First Aid
2015 International Consensus on First Aid Science With Treatment
Recommendations
Eunice M. Singletary, Co-Chair*; David A. Zideman, Co-Chair*; Emmy D.J. De Buck;
Wei-Tien Chang; Jan L. Jensen; Janel M. Swain; Jeff A. Woodin; Ian E. Blanchard;
Rita A. Herrington; Jeffrey L. Pellegrino; Natalie A. Hood; Luis F. Lojero-Wheatley;
David S. Markenson; Hyuk Jun Yang; on behalf of the First Aid Chapter Collaborators
be refined according to circumstances, need, and regulatory
constraints.
One difference between this 2015 definition and that used
for the 2010 process is that the task force did not restrict first
aid to “assessments and interventions that can be performed…
with minimal or no equipment.” We acknowledge that, in most
cases, equipment might not be available to first aid providers,
particularly for bystanders and lay providers. However, the
First Aid Task Force noted that, in some countries, supplementary first aid supplies now include inexpensive and compact pulse oximeters, glucose meters, and other adjuncts never
before considered to be in the realm of first aid. In the 2015
treatment recommendations, we have striven to remain true to
the “minimal or no equipment” approach, but recognize that
addition of equipment, used by those trained to use and maintain it, may enhance care.
The task force strongly believes that education in first aid
should be universal: everyone can and should learn first aid.
Introduction
Definition of First Aid
Downloaded from http://ahajournals.org by on May 27, 2020
The International Liaison Committee on Resuscitation
(ILCOR) First Aid Task Force first met in June 2013.
Comprising nominated members from around the globe
appointed by each ILCOR member organization, the task force
members first agreed to the goals of first aid and produced a
definition of first aid as it might apply to the international setting. Task force members considered an agreed-upon definition
essential for the subsequent development of research questions, evidence evaluation, and treatment recommendations.
First aid is defined as the helping behaviors and initial
care provided for an acute illness or injury. First aid can be
initiated by anyone in any situation.
A first aid provider is defined as someone trained in first
aid who should
• Recognize, assess, and prioritize the need for first aid
• Provide care by using appropriate competencies
• Recognize limitations, and seek additional care when
How and Why Topics Were Chosen
In the autumn of 2012, ILCOR approved the First Aid Task
Force as a fully participating task force in the 2015 ILCOR
international evidence evaluation and appointed 2 international co-chairs. In the spring of 2013, each member council
of ILCOR nominated individuals for membership in the First
Aid Task Force. In addition to the co-chairs, 11 task force
members were appointed, representing the ILCOR member
organizations of the American Heart Association (AHA), the
European Resuscitation Council (ERC), the Heart and Stroke
Foundation of Canada, the Australian Resuscitation Council,
the InterAmerican Heart Foundation, and the Resuscitation
Council of Asia. Members included physicians specializing
in anesthesia, critical care/resuscitation, emergency medicine,
cardiology, internal medicine, and pediatric emergency medicine, as well as paramedics specializing in prehospital care
guideline development, specialists in first aid course education
needed
The goals of first aid are to preserve life, alleviate suffering, prevent further illness or injury, and promote recovery.
This definition of first aid addresses the need to recognize injury and illness, the requirement to develop a specific
skill base, and the need for first aid providers to simultaneously provide immediate care and activate emergency medical services (EMS) or other medical care as required. First
aid assessments and interventions should be medically sound
and based on evidence-based medicine or, in the absence of
such evidence, on expert medical consensus. The scope of
first aid is not purely scientific, as both training and regulatory requirements will influence it. Because the scope of
first aid varies among countries, states, and provinces, the
treatment recommendations contained herein may need to
The American Heart Association requests that this document be cited as follows: Singletary EM, Zideman DA, De Buck EDJ, Chang WT, Jensen
JL, Swain JM, Woodin JA, Blanchard IE, Herrington RA, Pellegrino JL, Hood NA, Lojero-Wheatley LF, Markenson DS, Yang HJ; on behalf of the
First Aid Chapter Collaborators. Part 9: first aid: 2015 International Consensus on First Aid Science With Treatment Recommendations. Circulation.
2015;132(suppl 1):S269–S311.
*Co-chairs and equal first co-authors.
This article has been co-published in Resuscitation. Published by Elsevier Ireland Ltd. All rights reserved.
(Circulation. 2015;132[suppl 1]:S269–S311. DOI: 10.1161/CIR.0000000000000278.)
© 2015 American Heart Association, Inc., European Resuscitation Council, and International Liaison Committee on Resuscitation.
Circulation is available at http://circ.ahajournals.org
DOI: 10.1161/CIR.0000000000000278
S269
�S270
Circulation
October 20, 2015
Downloaded from http://ahajournals.org by on May 27, 2020
and curriculum development, and a specialist in first aid evidence evaluation methodology and guideline development.
The task force convened in June 2013 to review the topics and questions that were evaluated in 2005 and 2010, past
research questions formulated in the PICO style (population,
intervention, comparator, outcomes) that were never completed, and the new questions that had been submitted since
2010 to the task force, and a priority list created. Topics were
reviewed for areas of controversy, known additional new science, and subject matter not previously evaluated. Task force
members created a priority list for review, and the top 10 priority-ranked PICO questions were assigned. After the successful commencement of the workflow, the task force co-chairs
added a further 12 PICO questions, including 5 new questions,
1 derived question, and 6 that had been previously reviewed.
Selected PICO questions that had been previously reviewed
were, in some cases, reworded to facilitate literature searches,
and outcomes were decided upon by group consensus.
Evidence reviewers were recruited through a call for volunteers distributed by ILCOR to stakeholder organizations around
the world. More than 30 individual reviewers were assigned
to topics, usually by preference or expertise, but avoiding any
direct conflicts of interest. In general, 2 evidence reviewers
were assigned to each PICO, supervised by a member of the
task force designated as the task force question owner. Evidence
reviewers included physicians with diverse specialties including
emergency medicine, EMS, wilderness medicine, critical care,
cardiology, occupational medicine, toxicology, anesthesia, pediatric emergency medicine, public health, and epidemiology, as
well as paramedics, nurse practitioners and first aid education
specialists with experience in guideline and curriculum development, and professional evidence evaluation and methodology
experts.
The Evidence Evaluation Process
For the 2015 international evidence evaluation process, the
AHA developed a new Web-based information and documentation platform, the Systematic Evidence Evaluation and
Review System (SEERS), to support the ILCOR systematic
reviews and to capture the data in reusable formats. This Webbased system facilitated structured reviews in a consistent format that would support the ultimate development of science
summaries and evidence-based treatment recommendations.
Each task force performed a detailed systematic review
based on the recommendations of the Institute of Medicine of
the National Academies,1 using the methodological approach
proposed by the Grading of Recommendations, Assessment,
Development, and Evaluation (GRADE) Working Group.2 After
identifying and prioritizing the PICO questions to be addressed,3
and with the assistance of information specialists, a detailed
search for relevant articles was performed in each of 3 online
databases (PubMed, Embase, and the Cochrane Library).
By using detailed inclusion and exclusion criteria, articles
were screened for further evaluation. The reviewers for each
question created a reconciled risk of bias assessment for each
of the included studies, using state-of-the-art tools: Cochrane
for randomized controlled trials (RCTs),4 Quality Assessment
of Diagnostic Accuracy Studies (QUADAS)-2 for studies of
diagnostic accuracy,5 and GRADE for observational studies
that inform both therapy and prognosis questions.6
GRADE evidence profile tables7 were then created to
facilitate an evaluation of the evidence in support of each of
the critical and important outcomes. The quality of the evidence (or confidence in the estimate of the effect) was categorized as high, moderate, low, or very low,8 based on the
study methodologies and the 5 core GRADE domains of risk
of bias, inconsistency, indirectness, imprecision, and other
considerations (including publication bias).9
The GRADE evidence profile tables were then used to
create a written summary of evidence for each outcome (the
consensus on science statements). Whenever possible, consensus-based treatment recommendations were then created.
These recommendations (designated as strong or weak) were
accompanied by an overall assessment of the evidence and a
statement from the task force about the values and preferences
that underlie the recommendations. Strong recommendations
use the words “we recommend,” and weak recommendations
use the words “we suggest.”
Further details of the methodology that underpinned the
evidence evaluation process are found in “Part 2: Evidence
Evaluation and Management of Conflicts of Interest.”
The learning curve for use of the GRADE evidence
evaluation methodology was steep and resulted in a total of
22 PICO questions, including 6 new questions, being completed by the task force before the ILCOR 2015 International
Consensus Conference on CPR and ECC Science With
Treatment Recommendations in February 2015. The remaining topics not reviewed for 2015 have since been reprioritized,
with the addition of several new questions that were identified
during the ILCOR 2015 work process.
Very little research has been conducted in first aid, and most
of the recommendations are extrapolations from research in the
prehospital or hospital setting. The selected methodology for
evaluation of the literature led to the elimination of lower-quality
data from animal studies, case series, and case reports, except for
topics where no human studies were identified that met the inclusion criteria. These more stringent requirements led to the inclusion of studies with a higher initial quality of evidence, but most
studies were eventually downgraded due to indirectness for the
first aid setting. The gaps in knowledge have been identified by
the evidence reviewers and summarized at the end of each treatment recommendation. It is our hope that these knowledge gaps
will be filled through future research. In the absence of evidencebased medicine to support a treatment recommendation, the task
force has made many recommendations based on expert opinion,
perceived best practice, and the principle of “do no harm.”
PICO Questions Reviewed
First Aid for Medical Emergencies
• Recovery position (FA 517)
• Optimal position for shock (FA 520)
• Oxygen administration for first aid (FA 519)
• Bronchodilator use for asthma with difficulty breathing
(FA 534)
• Stroke recognition* (FA 801)
*Topics not previously reviewed.
�Singletary et al
Aspirin for Chest Pain
• Aspirin for chest pain: administration† (FA 871)
• Aspirin for chest pain: early compared with late (FA 586)
Epinephrine for Anaphylaxis and Treatment of Hypoglycemia,
Exertion-Related Dehydration, and Chemical Eye Injuries
• Second dose of epinephrine for anaphylaxis (FA 500)
• Hypoglycemia treatment* (FA 795)
• Exertion-related dehydration and oral rehydration (FA 584)
• Eye chemical injury: irrigation (FA 540)
First Aid for Trauma Emergencies
• Control of bleeding (FA 530)
• Hemostatic dressings (FA 769)
• Use of a tourniquet (FA 768)
• Straightening of an angulated fracture (FA 503)
• First aid treatment for an open chest wound* (FA 525)
• Cervical spinal motion restriction (FA 772)
• Concussion* (FA 799)
• Cooling of burns (FA 770)
• Wet compared with dry burn dressing (FA 771)
• Dental avulsion (FA 794)
Education
• First aid training* (FA 773)
First Aid for Medical Emergencies
Downloaded from http://ahajournals.org by on May 27, 2020
Important medical topics reviewed for 2015 include use of supplementary oxygen for purposes other than patients with chest
pain, positioning for shock and recovery, use of bronchodilators
for asthmatics with acute shortness of breath, use of a second
dose of epinephrine for anaphylaxis, and the administration of
aspirin for chest pain. The exhaustive ILCOR literature search,
with the help of information specialists and the more rigorous
GRADE methodology, led to a few additional recommendations as well as differences in strength of recommendations.
• No evidence was found to support a change in current
practice for the use of supplementary oxygen by first aid
providers.
• The position recommended for the patient in shock remains
the supine position, although there is some evidence suggesting passive raising of the legs between 30° and 60°
may have a transient (7 minutes or less) benefit (Modified).
• There is a change in recommendations for the position of a
normally breathing, unresponsive person. Because a potential need has been shown for advanced airway management
in the supine position compared with a lateral recumbent
position, we are now recommending that the lateral recumbent position be used as a “recovery” position (Modified).
• Assisting with the administration of inhaled bronchodilators is recommended for asthmatics with acute shortness of breath (Unchanged).
• Although questions remain about the ability of a first aid
provider to recognize anaphylaxis, the use of a second
*Topics not previously reviewed.
†Topics derived from existing questions.
Part 9: First Aid
S271
dose of epinephrine via an autoinjector is beneficial
when a first dose fails to improve symptoms. Adverse
effects were not reported in studies included, although
this may reflect the administration of epinephrine with
an autoinjector, thus limiting opportunity for an inadvertent overdose injection (Modified).
• The use of aspirin for chest pain has been previously
reviewed; however, the task force agreed that this topic
should be looked at again in light of the newly implemented GRADE methodology and the emergence of
newer medications used for acute myocardial infarction
(MI). Thus, the original question asking if aspirin should
be administered for patients with MI was reviewed, followed by a review of the early (ie, prehospital) use of
aspirin for chest pain versus delayed (ie, in-hospital)
administration of aspirin (Modified).
• A new review topic is the use of stroke assessment systems to aid with recognition of stroke, with findings that
will have enormous implications for first aid and public
health. This review found a significant decrease in time
between symptom onset and arrival at a hospital or emergency department with the use of these assessment tools;
use of such tools may reduce the degree of damage from
stroke when treatment is initiated early (New).
• A new review looks at use of oral dietary sugars for mild
symptomatic hypoglycemia in diabetics. The studies for
this review administered various forms of dietary sugars, such as specific candies, dried fruit strips, juice, or
milk, in a dose-equivalent amount compared with glucose tablets, to diabetics with symptomatic hypoglycemia who were conscious and able to swallow and follow
commands. It was concluded that, as a group, dietary
sugar products were not as effective as glucose tablets
for relief of hypoglycemia, but all studied forms showed
benefit and potential usefulness in cases where glucose
tablets are not available (New).
Recovery Position (FA 517)
Among adults who are breathing and unresponsive outside of
a hospital (P), does positioning in a lateral, side-lying, recovery position (I), compared with supine position (C), change
overall mortality, need for airway management, the incidence
of aspiration, the likelihood of cervical spinal injury, complications, incidence of cardiac arrest (O)?
Introduction
In 2010, the treatment recommendation for this topic stated
that there was no evidence that moving an individual into
a recovery position was beneficial. It also stated that if an
individual with a suspected cervical spine injury had to be
turned onto his or her side, the high arm in endangered spine
(HAINES) position seemed to be safer.10 An extensive literature search and use of GRADE methodology resulted in some
studies from the 2010 review being excluded from the 2015
review and other newly identified studies being included. The
revised 2015 recommendations reflect this rigorous evidence
evaluation process.
Although some studies included in this review showed
no benefit to a recovery position over a supine position, there
were studies that demonstrated significant benefit in terms of
�S272
Circulation
October 20, 2015
maintaining an open airway. The task force thought a priority
outcome for any recovery position would be maintenance of
an open airway.
Consensus on Science
Downloaded from http://ahajournals.org by on May 27, 2020
Lateral, Side-Lying Recovery Position Compared With Supine
Position
For the critical outcome of the incidence of aspiration, we
identified very-low-quality evidence (downgraded for imprecision) from 1 observational study with a total of 142 patients11
found in the left lateral decubitus or supine position demonstrating no benefit to being in the left lateral position (relative
risk [RR], 0.93; 95% confidence interval [CI], 0.55–1.58). The
same observational study had a total of 132 patients found in
the right lateral decubitus or supine position and demonstrated
no benefit to being in the right lateral position (RR, 1.15; 95%
CI, 0.67–1.96).
For the critical outcome of need for airway management, only studies with indirect measures of potential need
for airway management were identified, including measures
of total airway volume and stridor scores. Very-low-quality
evidence (downgraded for risk of bias, indirectness, and
imprecision) from 1 observational study with 17 patients12
demonstrated the benefit of the lateral position by increasing
total airway volume (mean difference [MD], 2.7; 95% CI,
0.88–4.52), and very-low-quality evidence (downgraded for
indirectness, and imprecision) from 1 observational study
with 30 patients13 demonstrated the benefit of the lateral
position by decreasing stridor score (MD, −0.9; 95% CI,
−1.21 to −0.59).
HAINES Modified Recovery Position Compared With Lateral
Recovery Position
For the critical outcome of the likelihood of cervical spinal
injury, we identified very-low-quality evidence (downgraded
for indirectness and imprecision) from 1 observational study
with 2 healthy volunteers14 demonstrating less overall lateral
cervical spine flexion with the HAINES position (MD, −17;
95% CI, −21.39 to −12.62), no difference in lateral flexion
of the upper cervical spine with the HAINES position (MD,
−4.5; 95% CI, −11.7 to 2.7), and less lateral flexion of the
lower cervical spine with the HAINES position (MD, −12.5;
95% CI, −21.52 to −3.47). We have also identified very-lowquality evidence (downgraded for indirectness and imprecision) from 1 observational study with 10 cadavers with
surgically created cervical instability15 demonstrating no difference in linear translation between the HAINES recovery
position and the 1992 ERC lateral recovery position in terms
of medial/lateral movement (MD, −1.1; 95% CI, −5.17 to
2.97), compression/distraction (MD, −1.06; 95% CI, −3.7 to
1.58), or anterior/posterior movement (MD, −0.24; 95% CI,
−2.96 to 2.48).
Left Lateral Position Compared With Right Lateral Position
For the critical outcome of the incidence of aspiration, we
identified very-low-quality evidence (downgraded for imprecision) from 1 observational study with a total of 50 patients11
who were found in the left lateral decubitus or right lateral
decubitus position, demonstrating no benefit to the left versus
the right lateral position (RR, 0.82; 95% CI, 0.42–1.6).
1992 ERC Recovery Position Compared With Old Left
Lateral, Semiprone Resuscitation Council (UK) Recovery
Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for imprecision) from 1
observational study with 6 healthy volunteers16 demonstrating no difference in either position in terms of venous occlusion (RR, 5; 95% CI, 0.29–86.44), arterial insufficiency with
venous occlusion (RR, 5; 95% CI, 0.29–86.44), or left arm
discomfort (RR, 7; 95% CI, 0.44–111.92).
1997 Resuscitation Council (UK) Recovery Position
Compared With 1992 ERC Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with 100
healthy volunteers17 demonstrating less pain/discomfort
with the 1992 ERC recovery position (RR, 3.25; 95% CI,
1.81–5.83).
AHA Semiprone Recovery Position Compared With 1992
ERC Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with 40
healthy volunteers placed in 1 or both of the positions18 demonstrating less discomfort with the AHA recovery position
(RR, 0.36; 95% CI, 0.14–0.95).
Morrison, Mirakhur, and Craig Recovery Position Compared
With Rautek Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with 20
healthy volunteers placed in 1 or both of the positions18 demonstrating no difference in discomfort between the positions
(RR, 1.25; 95% CI, 0.47–3.33).
AHA Semiprone Recovery Position Compared With Morrison,
Mirakhur, and Craig Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with 30
healthy volunteers placed in 1 or both of the positions18 demonstrating no difference in discomfort between the positions
(RR, 0.4; 95% CI, 0.14–1.17).
AHA Semiprone Recovery Position Compared With Rautek
Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with 30
healthy volunteers placed in 1 or both of the positions18 demonstrating no difference in discomfort between the positions
(RR, 0.5; 95% CI, 0.16–1.59).
1992 ERC Recovery Position Compared With Morrison,
Mirakhur, and Craig Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with
30 healthy volunteers placed in 1 or both of the positions18
�Singletary et al
demonstrating no difference in discomfort between the positions (RR, 1.1; 95% CI, 0.53–2.23).
1992 ERC Recovery Position Compared With Rautek
Recovery Position
For the critical outcome of complications, we identified verylow-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1 observational study with 30
healthy volunteers placed in 1 or both of the positions18 demonstrating no difference in discomfort between the positions
(RR, 1.38; 95% CI, 0.58–3.24).
We did not identify any evidence to address the critical
outcome of overall mortality or the important outcome of incidence of cardiac arrest.
Treatment Recommendation
We suggest that first aid providers position individuals who
are unresponsive and breathing normally into a lateral, sidelying recovery (lateral recumbent) position as opposed to
leaving them supine (weak recommendation, very-low-quality
evidence).
There is little evidence to suggest the optimal recovery
position.
Downloaded from http://ahajournals.org by on May 27, 2020
Values, Preferences, and Task Force Insights
Due to the low-quality evidence, it was difficult to make a recommendation as to the best recovery position. In terms of the
HAINES position versus the standard left lateral position, the
task force chose to put more value in the outcomes of a study
that included cadavers with surgically created cervical spine
instability over a study involving 2 healthy volunteers. We
discussed the need for guideline developers to clearly address
situations in which a first aid provider should not move a person into a recovery position, such as in the presence of pelvic
or spinal injury.
Finally, discussions were held about the quality of breathing being used to help determine when it is appropriate to
move an individual into the recovery position. The qualifying term “breathing normally” was included in the treatment
recommendation so as to avoid the situation where a first aid
provider recognizes that an individual is breathing and moves
them into a recovery position when in fact chest compressions
should be initiated.
Knowledge Gaps
• Given the poor and outdated evidence available, further
research is needed as to the best recovery position.
• When should a first aid provider not move a person into
the recovery position?
Optimal Position for Shock (FA 520)
Among adults and children who receive first aid for shock (P),
does positioning of the patient (I), compared with not positioning the patient (C), change overall mortality, complications, incidence of cardiac arrest, vital signs, hospital length
of stay (O)?
Introduction
Similar to many topics reviewed for 2015, the reviewers
for this PICO question were challenged by the paucity of
Part 9: First Aid
S273
good-quality scientific studies and the need to extrapolate
data from studies in normotensive volunteers or from studies designed to determine fluid responsiveness in hypotensive
intensive care unit patients. The diversity of positions studied
and the varying time intervals between change of position or
maintenance in a position created difficulty with interpreting
results. Results often differed for the same position between
studies. The supine position remains a basic position that the
First Aid Task Force thinks is the most appropriate position for
an individual with signs or symptoms of shock.
Consensus on Science
After application of inclusion and exclusion criteria, 1 RCT
and 5 observational trials were included in evidence evaluation. For the critical outcome of vital signs, we identified 1
RCT and 5 observational trials.
In Normotensive Subjects (P), Passive Leg Raising to 60° for
5 Minutes (I) Compared With Supine Position (C)
We identified very-low-quality evidence (downgraded for
inconsistency, indirectness, and imprecision) from 1 observational study19 enrolling 43 subjects (12 healthy subjects and 31
subjects with heart disease) showing no significant changes in
systolic blood pressure (SBP), diastolic blood pressure (DBP),
or heart rate (HR).
In Normotensive Subjects With Blood Loss (P), Passive Leg
Raising to 45° for 5 Minutes (I) Compared With Supine
Position for 5 Minutes (C)
We identified low-quality evidence (downgraded for inconsistency, indirectness, and imprecision) from 1 observational
study20 enrolling 27 normotensive subjects with 500 mL blood
loss, showing no benefit from passive leg raising (PLR) with a
nonsignificant change in mean arterial blood pressure (MAP)
but a benefit from PLR, with a significant
• Increase in thoracic bioimpedance cardiac index (MD,
0.8; 95% CI, 0.75–0.85)
in stroke index (SI) (MD, 15.00; 95% CI,
14.46–15.54)
• Decrease in HR (MD, −3; 95% CI, −3.56 to −2.44)
• Increase
Subjects without blood loss showed a significant increase
in cardiac index with PLR (MD, 0.3; 95% CI, 0.12–0.72) but
no significant change in MAP or difference in HR.
In Normotensive Subjects With Blood Loss (P), Standing
for 5 Minutes (I) Compared With Supine Position (C) for 5
Minutes
We identified low-quality evidence (downgraded for inconsistency, indirectness, and imprecision) from 1 observational
study20 enrolling 27 normotensive subjects with 500 mL blood
loss, showing a nonsignificant increase in MAP.
The standing position showed a statistically significant
decrease in cardiac index compared with supine position
(MD, −0.3; 95% CI, −0.38 to −0.22), and an increase in HR
(MD, 22; 95% CI, 20.84–23.16).
In Normotensive Subjects (P), Supine Position for 3 Minutes
Followed by PLR to 60° for 20 Seconds (I) Compared With
Supine Position (C) for 3 Minutes
We identified very-low-quality evidence (downgraded
for inconsistency, indirectness, and imprecision) from 1
�S274
Circulation
October 20, 2015
observational study21 enrolling 10 normotensive subjects
showing a benefit from the supine position plus PLR, with
a significant increase in both cardiac output (CO) (MD, 0.6;
95% CI, 0.48–0.72) and stroke volume (SV) (MD, 7; 95% CI,
2.93–11.07).
In Normotensive Subjects (P), Supine Position for 3 Minutes
Followed by PLR to 60° for 7 Minutes (I) Compared With
Supine Position for 3 Minutes (C)
We identified very-low-quality evidence (downgraded for
inconsistency, indirectness, and imprecision) from 1 observational study21 enrolling 10 normotensive subjects showing
no significant difference in MAP, CO, or HR. Thus, improvements in CO and SV seen with PLR at 20 seconds disappeared
by 7 minutes.
In Normotensive Subjects (P), PLR to 60° for 1 Minute (I)
Compared With Supine Position (C)
We identified very-low-quality evidence (downgraded for
inconsistency, indirectness, and imprecision) from 1 observational study22 enrolling 125 normotensive subjects. No cardiovascular benefit was shown for PLR to 60° for 1 minute.
In Hypotensive Patients (P), PLR to 45° (I) for 2 Minutes
Compared With Semirecumbent (Head at 45°) for 2 Minutes (C)
We identified low-quality evidence (downgraded for inconsistency, indirectness, and imprecision) from 1 RCT23 enrolling
35 hypotensive subjects. No difference was found in HR, but a
statistically significant benefit with PLR was demonstrated with
Downloaded from http://ahajournals.org by on May 27, 2020
• An increase in MAP (median difference 7 higher, CI not
estimable)
• An increase in SBP (median difference 12 higher, CI not
estimable)
• An increase in central venous pressure (CVP) (median
difference 2 higher, CI not estimable)
In Hypotensive Patients (P), Supine Position (C) for 2
Minutes Compared With Semirecumbent (Head at 45°) for 2
Minutes (I)
We identified low-quality evidence (downgraded for inconsistency, indirectness, and imprecision) from 1 RCT23 enrolling 35 hypotensive subjects. Placing patients in the supine
position for 2 minutes compared with a semirecumbent 45°
position failed to show any benefit for MAP, SBP, or HR. A
significant increase in CVP was reported with transfer from
semirecumbent to supine position (median difference 1 higher,
CI not estimable).
In Hypotensive Patients (P), PLR to 45° for 2 Minutes (I)
Compared With Supine for 2 Minutes (C)
We identified very-low-quality evidence (downgraded for
inconsistency, indirectness, and imprecision) from 1 RCT23
enrolling 35 hypotensive subjects. No difference was noted
for HR, but a statistically significant benefit with PLR was
shown with
• An increase in MAP (median difference 5 higher, CI not
estimable)
• An increase in systolic arterial pressure (SAP) (median
difference 8 higher, CI not estimable)
• An increase in CVP (median difference 1 higher, CI not
estimable)
In Hypotensive Patients (P), Supine Position for 4 Minutes
(C) Compared With PLR to 45° for 4 Minutes (I)
We identified very-low-quality evidence (downgraded for
inconsistency, indirectness, and imprecision) from 1 observational study24 enrolling 15 hypotensive subjects. No statistically significant difference in MAP or HR was shown between
the supine position and PLR to 45° for 4 minutes. A statistically significant decrease in SAP was found for change in
position from PLR to supine (MD, −4; 95% CI, −16.88 to
8.88) and for diastolic arterial pressure (DAP) (MD, −3; 95%
CI, −14.81 to 8.81).
In Hypotensive Patients (P), PLR to 45° for 4 Minutes (I)
Compared With Supine for 4 Minutes (C)
We identified very-low-quality evidence (downgraded for
inconsistency, indirectness, and imprecision) from 1 observational study24 enrolling 15 hypotensive subjects. There was
no statistically significant difference in MAP or HR between
PLR to 45° for 4 minutes and the supine position for 4 minutes. Statistically significant benefit with PLR was found for
SAP (MD, 7; 95% CI, −10.89 to 24.89) and DAP (MD, 3.0;
95% CI, −8.47 to 14.47).
We did not identify any evidence to address the critical
outcomes of complications, incidence of cardiac arrest, overall mortality, or length of hospital stay.
Treatment Recommendation
We suggest first aid providers place individuals with shock in
the supine position as opposed to the upright position (weak
recommendation, low-quality evidence).
Values, Preferences, and Task Force Insights
In regard to other positions studied, a review of the evidence suggests clinical equipoise in the first aid setting. For
individuals with shock who are in the supine position and
with no evidence of trauma, the use of PLR may provide a
transient (less than 7 minutes) but statistically significant
improvement in HR, MAP, cardiac index, or stroke volume.
The clinical significance of this transient improvement is
uncertain; however, no study reported adverse effects due
to PLR.
Because improvement with PLR is brief and its clinical
significance uncertain, this position is not recommended,
although it may be appropriate in some first aid settings as
a temporizing measure while awaiting more advanced emergency medical care. Studies included used PLR ranging
between 30° and 60° elevation. An optimal degree of elevation was not identified.
• Categories of hypotensive shock in studies included with
this review were septic shock, cardiogenic shock, and
hypovolemic shock.
• In making these recommendations, we place increased
value on the potential but uncertain clinical benefit of
improved vital signs and cardiac function by positioning
an individual with shock in the supine position or supine
with PLR position over the risk of movement to effect a
change in position.
�Singletary et al
• The Trendelenburg
position was excluded from evaluation in this review due to the inability or impracticality of first aid providers to place a person into the
Trendelenburg position in an out-of-hospital setting.
Knowledge Gaps
Well-designed studies are needed to assess
• Clinical
effects of position change in hypotensive
patients
• Effect of position change in patients without fluid
responsiveness
• Adverse effects of position change
Oxygen Administration for First Aid (FA 519)
Among adults and children who exhibit symptoms or signs
of shortness of breath, difficulty breathing, or hypoxemia
outside of a hospital (P), does administration of supplementary oxygen (I), compared with no administration of oxygen
(C), change survival with favorable neurologic/functional
outcome at discharge, 30 days, 60 days, 180 days, and/or
1 year; survival only at discharge, 30 days, 60 days, 180
days, and/or 1 year; shortness of breath; time to resolution
of symptoms; or therapeutic endpoints (eg, oxygenation and
ventilation) (O)?
Downloaded from http://ahajournals.org by on May 27, 2020
Introduction
Administration of supplementary oxygen is traditionally
considered essential for individuals presenting with shortness of breath, difficulty breathing, or hypoxemia. In certain circumstances, oxygen supplementation might have
potential adverse effects that complicate the disease course
or even worsen clinical outcomes. In this PICO question, we
sought to determine the impact of oxygen supplementation,
as compared with no oxygen supplementation, on outcomes
of patients who have shortness of breath, difficulty breathing,
or hypoxemia.
This review differs from the 2010 review in the targeted
population. In 2015, we focus on adults and children who
exhibit signs and symptoms of shortness of breath, difficulty
breathing, or hypoxemia in the out-of-hospital setting. In
addition, we attempt to identify specific medical conditions
that may benefit from supplementary oxygen administration
by first aid providers. We excluded chest pain from the conditions evaluated for potential use of oxygen. Oxygen administration for individuals with chest pain due to acute coronary
syndrome is separately reviewed by the ACS task force and
described in “Part 5: Acute Coronary Syndromes.”
Consensus on Science
For the critical outcomes of survival and therapeutic endpoints as measured by a composite of death, need for
assisted ventilation, and respiratory failure, we identified very-low-quality evidence (downgraded for risk of bias,
indirectness, and imprecision) from 1 retrospective observation study25 enrolling 232 patients with acute exacerbation
of chronic obstructive pulmonary disease showing no benefit
from supplementary oxygen administration (odds ratio [OR],
1.4; 95% CI, 0.6–2.9).
Part 9: First Aid
S275
For the important outcome of shortness of breath, we
identified very-low-quality evidence (downgraded for inconsistency and serious indirectness) from 1 RCT26 enrolling 14
terminal cancer patients with dyspnea and hypoxemia showing benefit with supplementary oxygen administration (MD in
visual analog scale score, −20.5; 95% CI, −27.6 to −13.5), and
low-quality evidence (downgraded for inconsistency and indirectness) from 1 meta-analysis27 and 4 RCTs26,28–30 enrolling
134 advanced cancer patients with dyspnea without hypoxemia who did not show benefit from supplementary oxygen
administration (standardized MD, −0.09; 95% CI, −0.22 to
0.04, P=0.16).
For the important outcome of oxygen saturation, we
identified moderate-quality evidence (downgraded for indirectness) from 3 RCTs, 1 enrolling 14 terminal cancer patients
with dyspnea and hypoxemia26 (MD in oxygen saturation,
8.6%; 95% CI, 7.0–10.3), 1 enrolling 6 patients with dyspnea
and hypoxemia29 (MD in oxygen saturation, 10.0%; 95% CI,
6.3–13.7), and 1 enrolling 51 advanced cancer patients with
dyspnea28 (mean increase in oxygen saturation, air 0.94% versus oxygen 5.43%; P<0.001), all showing benefit with supplementary oxygen.
For the important outcome of complete relief of decompression injury after first recompression, we identified
very-low-quality evidence (downgraded for risk of bias and
indirectness) from 1 retrospective observation study31 enrolling 2231 patients with decompression injury from a registry
database showing benefit from first aid supplementary oxygen
administration (OR, 1.5; 95% CI, 1.2–1.8).
We did not identify any evidence to address the outcomes
of survival, survival with favorable neurologic outcomes, or
time to resolution of symptoms.
Treatment Recommendation
No recommendation; the confidence in effect estimate is so
low that the task force thinks a recommendation to change
current practice is too speculative.
Values, Preferences, and Task Force Insights
In this review, the administration of supplementary oxygen
was found to be of some benefit in the following specific
circumstances:
• Advanced cancer patients who exhibit symptoms or signs
of shortness of breath (dyspnea) and signs of hypoxia
• Individuals with decompression injury
The use of supplementary oxygen should be limited to
individuals with specific training in oxygen administration.
Public commenting requested an oxygen saturation target
for this review. We did not evaluate flow rates, but patients
with hypoxemia in the included studies were provided supplementary oxygen that helped them reach normoxemia.
Knowledge Gaps
• Is
oxygen beneficial to all patients with shortness of
breath or dyspnea with diverse etiologies?
• Does administration of oxygen improve survival
in patients presenting with shortness of breath or
hypoxemia?
�S276
Circulation
October 20, 2015
Bronchodilator Use for Asthma with Difficulty
Breathing (FA 534)
Among adults and children in the prehospital setting who have
asthma and are experiencing difficulty in breathing (P), does
bronchodilator administration (I), compared with no bronchodilator administration (C), change time to resolution of symptoms, time to resumption of usual activity, complications,
harm to patient, therapeutic endpoints (eg, oxygenation and
ventilation), need for advanced medical care (O)?
Introduction
The 2005 review of asthma and bronchodilator therapy noted
that the incidences of severe asthma and deaths from asthma
are increasing and found bronchodilator therapy for wheezing to be safe and effective.32 Although evidence in 2005 was
extrapolated from prehospital and hospital studies, the potential benefit of decreased mortality led to the recommendation
that first aid rescuers assist with administration of bronchodilator therapy for asthmatics with acute shortness of breath.
The use of bronchodilators in the first aid setting can
take many forms, ranging from assisting someone with their
bronchodilator to administering a bronchodilator as part of an
organized response team with medical oversight. This review
did not compare methods of bronchodilator therapy but sought
evidence for or against patient outcomes with all inhaled
bronchodilator therapies that might be used for acute asthma
exacerbations.
Downloaded from http://ahajournals.org by on May 27, 2020
Consensus on Science
After application of inclusion and exclusion criteria, the
search strategy yielded 8 double-blind RCTs,33–40 2 observational studies,41,42 and 1 meta-analysis.43 It is important to note
that all of these trials involved administration of the bronchodilators in a healthcare setting (prehospital EMS setting,
emergency department, or in-hospital setting); because none
involved administration by first aid providers in a typical first
aid setting, all have been downgraded for indirectness.
Regarding the critical outcome of time to resolution of
symptoms, 2 RCTs were found. Very-low-quality evidence
(downgraded for risk of bias, imprecision, and indirectness) from 1 RCT33 with 28 participants aged 3 months to
2 years showed benefit in reduction of respiratory rate (MD,
5.1; 95% CI, 0.45–9.75), wheezing score (MD, 0.8; 95%
CI, 0.36–1.24), accessory muscle score (MD, 0.85; 95%
CI, 0.45–1.23), and total clinical score (MD, 2.5; 95% CI,
1.06–3.94) when treatment (albuterol/salbutamol nebulization) was compared with placebo. Low-quality evidence
(downgraded for imprecision and indirectness) from another
RCT34 with 17 participants aged 18 to 41 years showed benefit in reduction of time to subjective improvement in dyspnea in participants treated with fast-acting β2-adrenergic
agonists (formoterol or salbutamol dry-powdered inhaler)
compared with placebo dry-powdered inhaler or the slowacting β2-agonist (salmeterol dry-powdered inhaler). This
study also demonstrated a reduction in time to return to baseline symptoms in the fast-acting β2-adrenergic agonist group
compared with the placebo or slow-acting β2-agonist groups
(MD indeterminable).
Regarding the critical outcome of time to resumption of
usual activity, there were no human trials found.
Regarding the important outcome of complications, verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 RCT33 with 28 participants aged
3 months to 2 years failed to demonstrate a significant difference in mean HR between participants treated with nebulized
albuterol/salbutamol and those treated with placebo (MD,
7; 95% CI, −9.6 to 23.6). Very-low-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from
a second RCT35 comprising 11 participants aged between 9
and 16 years failed to demonstrate a difference in mean HR
or mean blood pressure when albuterol/salbutamol metereddose aerosol was compared with placebo. A total of 4 patients
on the albuterol/salbutamol days reported tremors, compared
with 6 on the placebo days. All tremors were “fine” in quality. Very-low-quality evidence (downgraded for risk of bias,
imprecision, and indirectness) from a third RCT36 comprising
100 patients with an average age of 33 years failed to demonstrate a significant difference in potassium, SBP or DBP,
tremor, headache, nervousness, weakness, palpitations, or dry
mouth between the albuterol/salbutamol metered-dose aerosol
given once group (T0), compared with every 30 minutes for
4 doses group (T30), compared with every 60 minutes for 2
doses group (T60). There was a statistically significant difference in mean HR change between the T30 compared with T0
groups, where the T30 group’s HR (beats per minute [BPM])
increased and the T0 group’s decreased (MD, 9.2; 95% CI,
3.51–14.93). Very-low-quality evidence (downgraded for risk
of bias, imprecision, and indirectness) from an observational
study41 comprising 52 participants with an average age of 33.6
years failed to demonstrate a significant difference in respiratory rate and HR between the treatment group (nebulized
isoetharine) and the control group. One participant in the treatment group reported headache and 2 participants in the control
group reported headache or nausea (MD undeterminable).
Regarding the important outcome of harm to patient, there
were no human trials found.
Regarding the important outcome of therapeutic endpoints (eg, oxygenation and ventilation), 1 RCT35 with verylow-quality evidence (downgraded for bias, imprecision, and
indirectness) showed benefit in an improvement in percentage
maximal achievable forced expiratory volume over 1 second
(FEV1) and forced vital capacity (FVC) at 60 minutes when
comparing inhaled albuterol/salbutamol metered-dose aerosol
or isoproterenol metered-dose aerosol to placebo and at 360
minutes (MD undeterminable). A second RCT37 with verylow-quality evidence (downgraded for bias, imprecision, and
indirectness) enrolled 134 participants with an average age
of 8.3 years, which demonstrated a statistically significant
improvement in FEV1 after initial treatment dose (day 0) for
levalbuterol/salbutamol and albuterol/salbutamol compared
with placebo (33.1%, 29.6% versus 17.8%; P<0.05). Verylow-quality evidence (downgraded for serious indirectness
and imprecision) from a third RCT36 involving 100 patients
demonstrated a statistically significant improvement in FEV1
when albuterol/salbutamol metered-dose aerosol was given
every 30 minutes for 4 doses (T0, 30, 60, 90) or every 60
minutes for 2 doses (T0, 60) compared with when albuterol/
salbutamol metered-dose aerosol was given once at T0 (MD
undeterminable). Very-low-quality evidence (downgraded for
�Singletary et al
Downloaded from http://ahajournals.org by on May 27, 2020
serious indirectness and imprecision) was identified in another
RCT38 enrolling 17 patients ranging in age from 18 to 41
years, who demonstrated a more rapid return to 85% of baseline FEV1 when treated with formoterol dry-powdered inhaler
or albuterol/salbutamol dry-powdered inhaler compared with
placebo (7.2 and 6.5 minutes versus 34.7 minutes, respectively). This study also showed benefit by demonstrating an
increase in FEV1 at 60 minutes with formoterol, albuterol/
salbutamol, and salmeterol all by dry-powdered inhaler compared with placebo (46.2%, 42.2%, and 41.2% versus 31.5%,
respectively) (MD undeterminable).
Further very-low-quality evidence (downgraded for risk of
bias, very serious indirectness, and imprecision) was identified from an RCT39 enrolling 26 patients between 7 and 16
years of age, which showed a benefit in median recovery
time to 95% of baseline FEV1 of 5.0 minutes for formoterol
dry-powdered inhaler versus 44 minutes with placebo (MD
undeterminable). Very-low-quality evidence (downgraded for
very serious risk of bias, imprecision, and very serious indirectness) from an RCT40 enrolling 17 patients with an average
age of 10.3 years demonstrated that formoterol dry-powdered inhaler and albuterol/salbutamol dry-powdered inhaler
resulted in a mean recovery time to within 90% of baseline
FEV1 that was shorter than that of placebo (8.3 minutes and
13.2 minutes versus 36.1 minutes, respectively) (MD undeterminable). Very-low-quality evidence (downgraded for risk
of bias, very serious imprecision, and indirectness) from an
RCT33 showed an increase in arterial oxygen saturation in
nebulized albuterol/salbutamol treated patients compared
with those who were treated with placebo (MD of 1.6, 0.28,
and 2.92, respectively). Very-low-quality evidence (downgraded for risk of bias and indirectness) from 1 observational
study41 demonstrated an improvement in percent recovery of
peak expiratory flow rate (PEFR) when patients were treated
with nebulized isoetharine compared with placebo (MD, 55.3;
95% CI, 25.4–85.2). Very-low-quality evidence (downgraded
for risk of bias and indirectness) from a second observational
study42 enrolling 208 participants with an average age of 43.7
years showed a reduction in first posttreatment PEFRs of less
than 120 L/min in the cohort given prehospital nebulized albuterol compared with a historic control (RR, 0.75; 95% CI,
0.58–0.98). In addition, the patient condition on arrival at the
emergency department was not as severe in the prehospital
nebulized albuterol group versus control (RR, 0.79; 95% CI,
0.64–0.98).
Regarding the low priority outcome of need for advanced
medical care, very-low-quality evidence (downgraded for
risk of bias, very serious indirectness, and imprecision) from 1
RCT36 showed a benefit with a significant association between
early, frequent use of albuterol/salbutamol metered-dose aerosol and fewer subsequent albuterol/salbutamol metered-dose
aerosol treatments. Participants who received 30-minute or
60-minute albuterol/salbutamol metered-dose aerosol compared with a single dose placebo at study start required less
subsequent bronchodilation after study end at 120 minutes
(20.6%, 23.5%, and 42.4%, respectively; P<0.05).
Very-low-quality evidence (downgraded for very serious
risk of bias, imprecision, and indirectness) from an observational study42 showed no benefit, by failing to demonstrate
Part 9: First Aid
S277
a difference in length of emergency department stay when
patients were administered prehospital nebulized albuterol/
salbutamol compared with those who were not. Very-lowquality evidence (downgraded for risk of bias, imprecision,
and indirectness) from a meta-analysis43 failed to demonstrate
a difference in clinical outcome or patient disposition in those
patients treated with nebulized ipratropium bromide and nebulized albuterol/salbutamol compared with those treated with
nebulized albuterol/salbutamol alone.
Treatment Recommendation
When an individual with asthma is experiencing difficulty
breathing, we suggest that trained first aid providers assist the
individual with administration of a bronchodilator (weak recommendation, very-low-quality evidence).
Values, Preferences, and Task Force Insights
In making this recommendation, we place higher value in an
intervention that may reduce mortality in a life-threatening situation over the risk of potential adverse effects. This review found
evidence that use of a bronchodilator in asthmatics with acute
difficulty breathing is effective for reducing wheezing, dyspnea,
and respiratory rate, while improving measures of effectiveness
such as FEV1 or PEFR, and with few reported side effects.
As with the 2005 review and as noted above, no studies
of bronchodilator administration in the first aid setting met
the inclusion criteria; therefore, studies were used from the
EMS and hospital settings. While these studies support the use
of bronchodilators for asthmatics with difficulty in breathing,
caution is required in extrapolating our findings to a first aid
recommendation.
The task force recognizes that first aid providers may be
limited in their abilities to administer or assist with bronchodilator therapy due to clinical governance and local regulations. In addition, this recommendation must be appropriately
operationalized by first aid organizations with due consideration to the setting and scope of practice in which the first aid
is being applied.
Knowledge Gaps
• What is the optimal bronchodilator for administration?
• What is the optimal dose of bronchodilator?
• How should this bronchodilator be administered?
• Is there evidence that prehospital use of bronchodilators
for asthmatics with acute shortness of breath reduces
mortality?
Stroke Recognition (FA 801)
Among adults with suspected acute stroke (P), does the use of
a rapid stroke scoring system or scale (I), compared with standard first aid assessment (C), change time to treatment (eg,
door to drug), recognition of acute injury or illness, discharge
with favorable neurologic status, survival with favorable neurologic outcome, or increased public/layperson recognition of
stroke signs (O)?
Introduction
The use of stroke assessment systems has become widespread
by EMS and other healthcare providers to identify individuals
�S278
Circulation
October 20, 2015
2.
3.
Figure 1. Summary receiver operating characteristic plot of
stroke screening systems.
4.
Downloaded from http://ahajournals.org by on May 27, 2020
with possible stroke, but in many countries, it is often not an
educational component of first aid courses. In some regions,
simple stroke assessment systems have been the focus of
recent public campaigns, with the objective of raising public awareness of the signs of stroke and minimizing delays in
recognition, diagnosis, and definitive treatment. This review
evaluated the outcomes related to use of stroke assessment
systems and showed reduced time to recognition of stroke
with most stroke assessment systems, more accurate recognition of stroke, and increased public/layperson recognition of
signs of stroke.
The task force discussed the need to identify the relative
sensitivities and specificities of each included stroke assessment system to discern which may be most useful in the first
aid setting. The ideal stroke assessment system for use by first
aid providers would have high sensitivity, thereby “casting a
wide net” to identify possible stroke victims. Additional benefit may be gained if a stroke assessment system with both
high sensitivity and specificity is used by those with advanced
training (such as EMS providers). Thus, this review identified
stroke assessment systems that may be preferred, based on
sensitivity and specificity, to aid those developing guidelines
for stroke recognition in various first aid and out-of-hospital
settings (Figures 1 and 2).
Consensus on Science
For the critical outcome of time to treatment, we identified
6 studies with 6 different stroke assessment systems studied:
1. For the Face (facial drooping), Arm (arm weakness),
Speech (speech difficulty), Time (time to call 9-1-1/
EMS) (FAST) scale (measured as number of patients
with time from symptom onset to hospital arrival within
3 hours), we identified moderate-quality evidence from
1 observational study44 enrolling 356 patients showing
benefit where 48.2% patients who had the scale applied
5.
6.
arrived within 3 hours compared with 14.6% who did not
have the scale applied (RR, 3.3; 95% CI, 2.29–4.75).
For the Kurashiki Prehospital Stroke Scale (KPSS;
measured as number of patients with time from symptom onset to hospital arrival within 3 hours), we identified very-low-quality evidence (downgraded for risk of
bias) from 1 observational study45 enrolling 430 patients
showing benefit where 62.9% patients who had the scale
applied arrived within 3 hours compared with 52.3%
who did not have the scale applied (RR, 1.2; 95% CI,
1.01–1.43). In the same study, the mean time was 2.1
hours for those who had a stroke screening scale applied
compared with 2.7 hours for those who did not have
a stroke screening scale applied (MD, −0.6; 95% CI,
−2.45 to 1.25).
For the Ontario Prehospital Stroke Scale (OPSS; measured as number of patients with time from symptom
onset to hospital arrival within 3 hours), we identified
very-low-quality evidence (downgraded for risk of bias)
from 1 observational study46 enrolling 861 patients showing no significant benefit where 52.3% patients who had
the scale applied arrived within 3 hours compared with
47.2% who did not have the scale applied (RR, 1.1; 95%
CI, 0.96–1.28).
For the Los Angeles Prehospital Stroke Screen (LAPSS;
measured in minutes from symptom onset to emergency
department arrival time), we identified low-quality
evidence from 1 observational study47 enrolling 1027
patients showing a mean time of 356 minutes for those
who had a stroke screening scale applied compared with
359 minutes for those who did not have a stroke screening scale applied (SMD, 0.11; 95% CI, 0.02–0.24).
For the Cincinnati Prehospital Stroke Scale (CPSS;
measured with EMS on-scene time), we identified lowquality evidence (downgraded for risk of bias) from 1
observational study48 enrolling 308 patients showing no
benefit, as the mean on-scene time was 17 minutes for
those who had a stroke screening scale applied compared
with 19 minutes for those who did not have a stroke
screening scale applied (MD, −2.00; 95% CI, −3.34 to
0.66).
For the Face, Arm, Speech, Time, Emergency Response
(FASTER) protocol (measured with symptom onset to
emergency department arrival [door] time), we identified very-low-quality evidence (downgraded for risk of
bias) from 1 observational study49 enrolling 115 patients
showing no significant benefit where the mean time was
59 minutes for those who had a stroke screening scale
applied compared with 76 minutes for those who did not
have a stroke screening scale applied (P=0.180).
For the important outcome of recognition of stroke
(interventional studies, outcome defined as definitive stroke
diagnosis or administration of thrombolytic/fibrinolytic; the
publications varied in the term used), we identified 4 observational studies of 4 different stroke scales:
1. For FAST (measured as number of patients with confirmed stroke or transient ischemic attack), we identified
moderate-quality evidence from 1 observational study44
enrolling 356 patients showing benefit where 48.2%
patients who had the scale applied were diagnosed
�Singletary et al
Part 9: First Aid
S279
Downloaded from http://ahajournals.org by on May 27, 2020
Figure 2. Forest plot of stroke assessment systems.
compared with 14.6% who did not have the scale applied
(RR, 3.3; 95% CI, 2.29–4.75).
2. For KPSS (measured as number of patients who received
fibrinolytic), we identified very-low-quality evidence
(downgraded for risk of bias) from 1 observational
study45 enrolling 430 patients showing no benefit where
13.7% patients who had the scale applied were diagnosed compared with 14.4% who did not have the scale
applied (RR, 0.95; 95% CI, 0.59–1.53).
3. For the FASTER scale (measured as number of
patients who received thrombolytic), we identified very-low-quality evidence (downgraded for risk
of bias) from 1 observational study49 enrolling 34
patients showing benefit where 19.1% patients who
had the scale applied received fibrinolytic compared
with 7.5% who did not have the scale applied (RR,
0.87; 95% CI, 0.78–0.98).
4. For CPSS (measured with patients who received fibrinolytic), we identified moderate-quality evidence from
1 observational study50 enrolling 308 patients showing
benefit where 45.7% patients who had the scale applied
received fibrinolytic compared with 2.1% who did not
have the scale applied (RR, 22.2%; 95% CI, 7.14–69.1).
For the important outcome of recognition of stroke (diagnostic studies, outcome defined as correct stroke diagnosis),
we identified low-quality evidence (all downgraded for risk
of bias) from 22 observational studies44,46–48,51–68 enrolling a
total of 30 635 patients, studying 8 different stroke screening
assessment systems, showing diagnostic performance across
all stroke screening systems of sensitivity ranging from 0.41
to 0.97 and specificity ranging from 0.13 to 1.00. These studies were divided into subgroups based on whether the stroke
scales included glucose measurement or not. For studies that
included stroke scales with glucose measurement (LAPSS,
OPSS, Melbourne Ambulance Stroke Screen [MASS], Medic
Prehospital Assessment for Code Stroke [Med PACS], and
Recognition of Stroke in the Emergency Room [ROSIER]),
the pooled sensitivity is 0.80 (95% CI, 0.79–0.81) and pooled
specificity is 0.93 (95% CI, 0.92–0.93), compared with
stroke scales without glucose measurement (FAST, CPSS,
and Medical Priority Dispatch System [MPDS]), which have
pooled sensitivity of 0.81 (95% CI, 0.81–0.82) and pooled
specificity of 0.47 (95% CI, 0.45–0.48).
For the important outcome of increased public/layperson recognition of signs of stroke, very-low-quality evidence
�S280
Circulation
October 20, 2015
(downgraded for risk of bias) from 1 human study69 enrolling
72 participants (members of the public) showed benefit where
76.4% of participants (55/72) were able to identify signs of
stroke before training on a stroke screening assessment system
compared with 94.4% (68/72) immediately after training (OR,
5.25; 95% CI, 1.67–16.52), and 96.9% of participants (63/65)
were able to identify the signs of stroke 3 months after training
(OR, 2.07; 95% CI, 0.36–11.69).
Downloaded from http://ahajournals.org by on May 27, 2020
Treatment Recommendation
We recommend that first aid providers use stroke assessment systems (such as FAST or CPSS) for individuals with
suspected acute stroke (strong recommendation, low-quality
evidence).
We suggest the use of FAST or CPSS stroke assessment
systems (weak recommendation, low-quality evidence).
We suggest the use of stroke assessment systems that
include blood glucose measurement, when available, such
as LAPSS, OPSS, ROSIER, or KPSS, to increase specificity of stroke recognition (weak recommendation, low-quality
evidence).
In the absence of a glucometer, we suggest the use of
FAST or CPSS stroke assessment systems compared with
MASS, LAMS, or MPDS (weak recommendation, low-quality evidence).
The literature search was rerun in January 2015 to capture the most updated evidence possible. Two additional studies were added51,59 and incorporated into the consensus on
science and GRADE tables, both supporting this treatment
recommendation.
Values, Preferences, and Task Force Insights
In making this recommendation, we place increased value on
the benefits of early stroke recognition, which could lead to
early treatment to minimize potentially devastating neurologic
injury.
Training first aid providers in stroke assessment systems
outweighs the risks, largely limited to false-positive identification by first aid providers. The cost of the intervention is
estimated to be low.
In this review of the literature, the stroke assessment systems include various components, such as looking for specific
signs and obtaining blood glucose levels. Our review found
that stroke assessment systems that included blood glucose
measurement had similar sensitivity and increased specificity to accurately identify stroke compared with those systems
that did not include glucose measurement. We recognize that
first aid providers may or may not have access to a properly
calibrated glucose measurement device. Although use of these
devices is not a standard component of first aid, glucose measurement devices are commonly available among the public.
Ideal stroke assessment systems for first aid use are accurate, have few steps, are easily understood and remembered,
and take minimal time to complete. Those developing local
guidelines for first aid providers can use the results of this
review to determine if the benefit of increased specificity with
systems that include glucose measurement would be desirable
in their settings, compared with using simpler stroke assessment systems that do not include glucose measurement, which
have similar sensitivity but lower specificity.
Knowledge Gaps
More research is required to determine how much training is
needed and what type of training should be used to enable
first aid providers to correctly apply stroke assessment systems and to compare the accuracy of use of stroke assessment
systems by first aid providers to the accuracy of use of stroke
assessment systems by healthcare providers. Research is also
required to determine accuracy of assessment and its effect
on survival and neurologic status at discharge. In addition,
future research could include investigating direct transport
to specified stroke centers when a stroke assessment system
measurement is positive (bypassing community/small emergency departments).
Aspirin for Chest Pain
Chest pain is one of the common symptoms of acute MI.
Antiplatelet agents such as aspirin play a large role in management. In 2010, the first aid treatment recommendation stated
that the administration of aspirin to individuals with chest discomfort was recommended.
In 2015, 2 PICOs were generated, 1 simply looking at the
administration of aspirin and the other looking at the timing of
this administration. The first PICO sought to determine if the
administration of aspirin in the setting of MI was beneficial.
Subsequently, the second PICO was used to determine if there
was a difference in outcomes when aspirin is given early, in
the first hours after symptom onset by a first aid provider, or
later, in the setting of chest pain symptoms due to suspected
acute MI. This same PICO was also used to see if there would
be benefit to early administration of aspirin to adults with
chest pain of unclear etiology.
Aspirin for Chest Pain: Administration (FA 871)
Among adults experiencing chest pain due to suspected MI (P),
does administration of aspirin (I), compared with no administration of aspirin (C), change cardiovascular mortality, complications, adverse effects, incidence of cardiac arrest, cardiac
functional outcome, infarct size, hospital length of stay (O)?
Introduction
This 2015 PICO question asks if administration versus no
administration of aspirin changed outcomes in the setting of
suspected acute MI. There are no major changes from what
has been stated in previous treatment recommendations.
Consensus on Science
For the critical outcome of cardiovascular mortality (at 5
weeks), we identified high-quality evidence from 1 RCT70
enrolling 17 187 patients with acute MI showing benefit to
aspirin (162.5 mg, enteric-coated) administration (RR, 0.79;
95% CI, 0.73–0.87).
For the critical outcome of cardiovascular mortality (at
3 months), we identified very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from
1 RCT71 enrolling 100 patients with acute MI showing no
benefit to aspirin (100 mg, capsule) administration (RR, 0.83;
95% CI, 0.4–1.75).
For the critical outcome of cardiovascular mortality (at
28 days), we identified low-quality evidence (downgraded for
�Singletary et al
Downloaded from http://ahajournals.org by on May 27, 2020
risk of bias and indirectness) from 1 RCT72 enrolling 1705
patients with acute MI showing no benefit to aspirin (300 mg,
capsule) administration (RR, 0.98; 95% CI, 0.81–1.19).
For the critical outcome of cardiovascular mortality
(in-hospital), we identified very-low-quality evidence (downgraded for risk of bias and indirectness) from 1 observational
study73 with a total of 22 572 patients with acute MI showing
benefit to aspirin (500 mg, oral or intravenous loading dose;
100 mg, oral; maintenance recommended) administration
(RR, 0.33; 95% CI, 0.31–0.35).
For the critical outcome of adverse effects (bleeding),
we identified high-quality evidence from 1 RCT70 enrolling
16 981 patients with acute MI showing adverse effects (minor
bleeding) with aspirin (162.5 mg, enteric-coated) administration (RR, 1.25; 95% CI, 1.04–1.51).
For the critical outcome of adverse effects (allergic reaction), we identified very-low-quality evidence (downgraded
for risk of bias and imprecision) from 1 observational study74
with 219 patients with suspected acute MI showing no adverse
effects (allergic reaction) with aspirin (dose not available)
administration (unable to calculate RR as there was no control
group).
For the critical outcome of complications, we identified high-quality evidence from 1 RCT70 enrolling 16 981
patients with acute MI showing benefit to aspirin (162.5 mg,
enteric-coated) administration (RR, 0.62; 95% CI, 0.52–
0.73). We also found very-low-quality evidence (downgraded for risk of bias, imprecision, and indirectness) from 1
RCT71 enrolling 100 patients with acute MI showing benefit
to aspirin (100 mg, capsule) administration (RR, 0.11; 95%
CI, 0.05–0.98).
We identified very-low-quality evidence (downgraded for
risk of bias and indirectness) from 1 observational study73
with a total of 22 572 patients with acute MI showing no benefit to aspirin (500 mg oral or intravenous loading, 100 mg
oral maintenance recommended) administration (RR, 1.05;
95% CI, 0.78–1.42).
For the critical outcome of incidence of cardiac arrest,
we identified high-quality evidence from 1 RCT70 enrolling 16 981 patients with acute MI showing benefit to aspirin
(162.5 mg, enteric-coated) administration (RR, 0.87; 95% CI,
0.79–0.96).
For the important outcome of infarction size, we identified very-low-quality evidence (downgraded for bias, imprecision, and indirectness) from 1 RCT71 enrolling 89 patients
with acute MI showing no benefit to aspirin (100 mg, capsule)
administration (MD, −161; 95% CI, −445.57 to 230.57).
We did not identify any evidence to address the important outcomes of cardiac functional outcome or length of
hospital stay.
Treatment Recommendation
We recommend the administration of aspirin to adults with
chest pain due to suspected MI (strong recommendation, highquality evidence).
Values, Preferences, and Task Force Insights
In making this recommendation, we place a higher value on
decreasing mortality and decreased complications of MI over
the risks of adverse effects, such as bleeding.
Part 9: First Aid
S281
Public comments for this question requested a suggestion
for the optimal aspirin dose and form. Our PICO question
was not designed to look at changes in outcomes based on
various doses of aspirin, as all the articles selected for review
compared administration to no administration, as opposed to
1 dose compared with another. Due to the heterogeneity in
study design in the articles that were included in this review,
the dose and form (eg, chewable or nonchewable, entericcoated or nonenteric coated) of aspirin varied, and no recommendation could be made regarding the optimal dose or form
of aspirin administered. Where available, the dose of aspirin
used for each study has been identified in the consensus on
science statement.
Knowledge Gaps
• Is aspirin safe if given to patients with chest pain who are
not having an MI?
• Is aspirin safe when given by a first aid provider?
• Is there high-quality evidence to indicate that the administration of aspirin after MI is time critical?
Aspirin for Chest Pain: Early Compared With Late
(FA 586)
Among adults who are experiencing chest pain outside of a
hospital (P), does early administration of aspirin (I), compared
with later administration of aspirin (C), change cardiovascular
mortality, complications, incidence of cardiac arrest, cardiac
functional outcome, infarct size, hospital length of stay, chest
pain resolution (O)?
Introduction
This 2015 PICO question asked if early administration versus later administration of aspirin changes outcomes, which
is different wording from the focus of the 2010 review. The
recommendation in 2015 differs from that in 2010 as a result
of the intent of the PICO question, as well as the studies identified after using the rigorous literature search techniques and
reviewed through the GRADE process.
Consensus on Science
In this review, early administration of aspirin is defined as
prehospital or administration in the first hours from onset of
symptoms of MI (ie, median 1.6 hours in 1 study).75
For the critical outcome of cardiovascular mortality
(at 7 days), we identified very-low-quality evidence (downgraded for risk of bias and indirectness) from 2 observational
studies75,76 with a total of 2122 patients with acute MI showing benefit to early aspirin administration (RR, 0.37; 95% CI,
0.23–0.62).
For the critical outcome of cardiovascular mortality (at
30 days), we identified very-low-quality evidence (downgraded for risk of bias and indirectness) from 2 observational
studies75,76 with a total of 2122 patients with acute MI showing benefit to early aspirin administration (RR, 0.45; 95% CI,
0.3–0.68).
For the critical outcome of cardiovascular mortality (at
5 weeks), we identified low-quality evidence (downgraded for
indirectness) from 1 RCT70 enrolling 8587 patients with acute
MI showing no benefit to aspirin (162.5 mg, enteric-coated)
�S282
Circulation
October 20, 2015
Downloaded from http://ahajournals.org by on May 27, 2020
administration within 2 hours of symptom onset (RR, 0.92;
95% CI, 0.76–1.11).
For the critical outcome of cardiovascular mortality
(at 1 year), we identified very-low-quality evidence (downgraded for indirectness) from 1 observational study75 with
1200 patients with acute MI showing benefit to early aspirin
(160 mg, oral) administration (RR, 0.47; 95% CI, 0.29–0.77).
For the critical outcome of complications, we identified
very-low-quality evidence (downgraded for indirectness)
from 1 observational study76 with a total of 922 patients with
acute MI showing no increase in complication rate with early
aspirin (greater than 200 mg, chewable) administration (RR,
0.61; 95% CI, 0.46–0.81). We also identified very-low-quality
evidence (downgraded for risk of bias and indirectness) from
1 observational study75 with a total of 1200 patients with acute
MI demonstrating an increase in complications (such as reischemia) in the group that received early aspirin (160 mg,
oral) administration (RR, 1.22; 95% CI, 1.09–1.37).
For the critical outcome of incidence of cardiac arrest,
we identified very-low-quality evidence (downgraded for
indirectness) from 1 observational study76 with a total of 922
patients with acute MI showing no benefit to early aspirin
(greater than 200 mg, chewable) administration (RR, 0.82;
95% CI, 0.56–1.2) and very-low-quality evidence (downgraded for risk of bias and indirectness) from 1 observational
study75 with a total of 1200 patients with acute MI demonstrating an increased incidence of cardiac arrest in the group
that received early aspirin (160 mg, oral) administration (RR,
1.53; 95% CI, 1.13–2.09).
We did not identify any evidence to address the important
outcomes of cardiac functional outcome, infarct size, or hospital length of stay or the low importance outcome of chest
pain resolution.
Treatment Recommendation
We suggest the early administration of aspirin by first aid providers to adults with chest pain due to suspected MI (weak
recommendation, very-low-quality evidence).
There is no evidence for the early administration of aspirin by first aid providers to adults with chest pain of unclear
etiology.
Values, Preferences, and Task Force Insights
In making this recommendation, we place a higher value on
the benefits of aspirin, such as decreased mortality from MI,
which outweigh possible risks of complications.
The task force discussed concerns about first aid providers
being able to differentiate chest pain of cardiac origin from
other causes of chest discomfort. With any treatment recommendations naming a particular clinical pathology, such as in
this case with MI or chest pain of cardiac origin, it is very
important that guidelines or educational materials clearly indicate what signs and symptoms the first aid provider should
look for to recognize that clinical presentation.
Knowledge Gaps
• Is aspirin safe if given to patients with chest pain of other
etiologies, particularly gastrointestinal?
• Is it safe for a first aid provider to administer 1 dose of
aspirin?
• Is
there any high-quality evidence demonstrating that
there is a critical time window for the administration of
aspirin after the onset of acute MI in terms of reducing
morbidity and mortality?
• Is the prehospital administration of aspirin required if
the patients are fast tracked to percutaneous coronary
intervention (PCI)?
Epinephrine for Anaphylaxis and Treatment
of Hypoglycemia, Exertion-Related
Dehydration, and Chemical Eye Injuries
This section includes the topics of a second dose of epinephrine for anaphylaxis and first aid treatment of hypoglycemia in
diabetics, exertion-related dehydration, and chemical injuries
of the eye.
Second Dose of Epinephrine for
Anaphylaxis (FA 500)
Among adults and children experiencing severe anaphylaxis
requiring the use of epinephrine (P), does administration of a
second dose of epinephrine (I), compared with administration
of only 1 dose (C), change resolution of symptoms, adverse
effects, complications (O)?
Introduction
In 2010, evidence evaluation regarding effectiveness of
administration of a second dose of epinephrine for anaphylaxis concluded that there was insufficient evidence
to make a recommendation regarding the routine first aid
administration of a second dose of epinephrine. Use of a
more rigorous literature search strategy and of the GRADE
methodology for the 2015 review provided additional scientific evidence that has resulted in a change in the treatment
recommendation.
The question’s specific focus was on the benefit of a second dose of epinephrine for severe anaphylaxis when signs
and symptoms fail to respond to an initial dose. For the purpose of this review, if a study provided data for epinephrine
administered after a first dose, unless the study specified that a
second dose was given as part of a protocol, it was presumed
that doses administered after a first dose were administered
due to failure to respond.
Consensus on Science
For the critical outcome of resolution of symptoms, we identified very-low-quality evidence (downgraded for risk of bias
and confounding) from 9 observational studies77–85 showing
benefit for giving a second dose (or multiple doses) of epinephrine to patients not responding to a first dose (RR, 1.16;
95% CI, 1.13–1.20).
In addition, for the critical outcome of resolution of
symptoms, we identified very-low-quality evidence (downgraded for risk of bias) from 1 observational study86 showing
no significant difference between the percentage of resolved
reactions in an ambulance service routinely using 2 doses of
epinephrine versus an ambulance service using a single dose
(RR, 0.97; 95% CI, 0.9–1.04).
We did not identify any evidence to address the critical
outcomes of adverse effects or complications.
�Singletary et al
Treatment Recommendation
We suggest a second dose of epinephrine be administered by
autoinjector to individuals with severe anaphylaxis whose
symptoms are not relieved by an initial dose (weak recommendation, very-low-quality evidence).
Downloaded from http://ahajournals.org by on May 27, 2020
Values, Preferences, and Task Force Insights
In making this recommendation, we place a higher value on
the resolution of life-threatening symptoms, such as airway
compromise, breathing difficulty, and circulatory collapse,
over the potential risk of adverse effects from an unnecessary
second injection.
When caring for a person with anaphylaxis, first aid providers should always call EMS (eg, 9-1-1 or 1-1-2) rescue
services.
Public comments and discussion on this topic centered on
issues of dosing, interval time for a second dose, and the possibility of adverse effects should epinephrine be inadvertently
administered to a person not experiencing anaphylaxis. This
evidence review did not evaluate the time interval between doses
of epinephrine or the optimal dose. However, literature included
in the review suggests that a second dose of epinephrine may be
administered 10 to 15 minutes after the initial dose.80
While the included studies did not identify any adverse
effects, selection bias might have prevented those effects
from being identified. Adverse effects have previously been
reported in the literature when epinephrine is administered in
the incorrect dose or via inappropriate routes, such as the intravenous route. Use of autoinjectors by first aid providers may
minimize the opportunity for incorrect dosing of epinephrine.
Knowledge Gaps
In 2010, first aid worksheet 303B attempted to define if or can
“the First Aid Provider Appropriately Recognize the Signs and
Symptoms of Anaphylaxis.” The task force did not address
this PICO question in 2015, and thus the question “How can
a first aid provider determine that a victim needs additional
epinephrine?” remains.
• What
should the time interval be between doses of
epinephrine?
• Would a higher concentration (0.5 mg) recommended
for standard therapy versus the injectable syringe dose
(0.3 mg) be more effective and decrease the need for
additional doses in the EMS setting?
• Should an initial injection be administered in the
early stages of anaphylaxis, before the onset of severe
symptoms?
Hypoglycemia Treatment (FA 795)
Among adults and children with symptomatic hypoglycemia
(P), does administration of dietary forms of sugar (I), compared
with standard dose (15–20 g) of glucose tablets (C), change time
to resolution of symptoms, risk of complications (eg, aspiration),
blood glucose, hypoglycemia, hospital length of stay (O)?
Introduction
This is a new topic for the 2015 consensus on science.
Because glucose tablets may not be readily available in all
first aid settings, this task force performed a review to evaluate
Part 9: First Aid
S283
the effectiveness of dietary (ie, food source) sugars compared
with glucose tablets for the management of symptomatic
hypoglycemia.
The literature search for this review identified 5 studies
that compared glucose tablets to various commercial sugarcontaining dietary products. The named commercial products
cited in the consensus on science and in the treatment recommendation were specifically included in evaluated studies and
are not particularly endorsed by the First Aid Task Force. To
our knowledge, none of the product manufacturers contributed
to or were involved with the identified studies. Two tables listing the specific sugar content for each studied product are provided to assist with guideline development (Tables 1 and 2).
Consensus on Science
Dietary Sugars (I) Compared With Glucose Tablets (C)
For the critical outcome of time to resolution of symptoms,
none of the 4 studies identified87–90 showed that any form of
dietary sugar or glucose tablets improved the blood glucose
before 10 minutes.
For the important outcome of hypoglycemia (clinical
relief in 15 minutes or less), we identified low-quality evidence (downgraded for risk of bias and imprecision) from 3
randomized controlled studies88–90 with pooled data from 502
diabetic patients treated with dietary sugars (sucrose, fructose,
orange juice, jelly beans, Mentos, and milk) and 223 treated
with glucose tablets (15–20 g) that showed a benefit with glucose tablets, with slower resolution of symptoms 15 minutes
after diabetic patients were treated with dietary sugars compared with glucose tablets (RR, 0.89; 95% CI, 0.83–0.96).
For the important outcome of blood glucose (diabetic
patients with at least a 20-mg/dL increase of blood glucose
by 20 minutes), we found very-low-quality evidence (downgraded for risk of bias and imprecision) from 1 observational
study87 with 13 diabetic patients treated with dietary sugars
and 9 treated with glucose tablets that showed a benefit with
glucose tablets, with fewer diabetic patients demonstrating
a 20-mg/dL increase in blood glucose level 20 minutes after
treatment when treated with dietary sugars compared with
glucose tablets (RR, 0.3; 95% CI, 0.1–0.85). For the critical outcome of time to resolution of symptoms, the important outcome of risk of complications (eg, aspiration), and the
low-priority outcome of hospital length of stay, there were no
human trials found.
Sucrose (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief
in 15 minutes or less), we found low-quality evidence (downgraded for risk of bias and imprecision) from 2 RCTs88,90 with
pooled data from 177 diabetic patients treated with sucrose
(165 with sucrose candy [Skittles] and 12 with sucrose tablets) and 171 treated with glucose tablets that showed no difference in their effects on blood glucose. Sucrose (either as
sucrose candy [Skittles] or sucrose tablets) and glucose tablets
were equivalent in providing clinical relief of hypoglycemia
15 minutes after ingestion (RR, 0.99; 95% CI, 0.91–1.07).
For the important outcome of blood glucose (mean change
in blood glucose [mmol/L] after 15 minutes), we found lowquality evidence (downgraded for risk of bias and imprecision)
�S284
Circulation
October 20, 2015
Table 1. Major Dietary Sugars With About 20 g Carbohydrate From Sugar and
Number of People With Improvement in Hypoglycemia Within 15 Minutes
Carbohydrates
per Serving
Type of Food or Fluid
Glucose tablets
Measure Representing
20 g Carbohydrates*
Clinical Relief 15 Minutes
or Less After Ingestion
Varies
Varies
194/223 (87.0%)
0.9 g/candy
20–25 candies
150/177 (84.7%)
Fructose (fruit leather,
eg, Stretch Island)‡
10 g/strip
2 strips
111/165 (67.3%)
Orange juice (unsweetened,
from concentrate)§
1 g/10 mL
200 mL
35/50 (70.0%)
33/45 (73.3%)
Sucrose (Skittles)†
Jelly beans§
1.1 g/jelly bean
15–20 jelly beans
Mentos║
2.8 g/mint
5–10 mints
Whole milk¶
21.75 g/mL
435 mL
44/48 (91.7%)
Not reported
*These measurements may differ from those in the evaluated studies, because the amount was not
standardized across studies.
†Manufacturer label.
‡One study88 used fruit leather under the trade name Fruit to Go (Kelowna, British Columbia, Canada). We
were unable to find the nutritional information for this fruit leather, so we substituted another brand, Stretch
Island Cherry Flavor (Stretch Island Fruit Co, La Jolla, CA); http://www.stretchislandfruit.com/en_US/
Products.html, accessed February 2, 2015.
§http://onlinelibrary.wiley.com/doi/10.1002/pdi.953/pdf.
║Manufacturer label.
¶Brodows, 1984.87
Downloaded from http://ahajournals.org by on May 27, 2020
from 1 randomized controlled study90 with 6 diabetic patients
treated with sucrose (dissolved in water) and 6 treated with
glucose tablets that showed a benefit to glucose administration, with the MD (mmol/L) in blood glucose 15 minutes after
ingestion lower with sucrose (dissolved in water) than glucose
tablets (MD, −0.9; 95% CI, −1.78 to −0.02). A second arm of
this same study with 6 diabetic patients treated with sucrose
(chewed) and 6 treated with glucose tablets showed no benefit, with the MD (mmol/L) in blood glucose 15 minutes after
ingestion similar between sucrose (chewed) and glucose tablets (MD, 0.3; 95% CI, −0.8 to 1.41). For the critical outcome
of time to resolution of symptoms, the important outcome of
risk of complications (eg, aspiration), and the lower-priority
outcome of hospital length of stay, there were no human trials
found.
Fructose (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief
in 15 minutes or less), we found low-quality evidence (downgraded for risk of bias and imprecision) from 1 RCT88 with 165
diabetic patients treated with fructose (Fruit to Go) and 165
treated with glucose tablets that showed benefit with glucose,
with a lower incidence of resolution of symptoms 15 minutes
after treatment for diabetic patients treated with fructose compared with glucose tablets (RR, 0.77; 95% CI, 0.68–0.86). For
the critical outcome of time to resolution of symptoms, the
important outcomes of risk of complications (eg, aspiration)
and blood glucose, and the low-priority outcome of hospital
length of stay, there were no human trials found.
Orange Juice (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief
in 15 minutes or less), we found very-low-quality evidence
(downgraded for risk of bias, inconsistency, and imprecision)
from 2 RCTs89,90 with the pooled data of 50 diabetic patients
treated with orange juice and 58 treated with glucose tablets that showed no difference in the resolution of symptoms
15 minutes after treatment for diabetic patients treated with
orange juice compared with glucose tablets (RR, 0.84; 95%
CI, 0.69–1.02). For the important outcome of blood glucose,
Table 2. Type of Dietary Sugar Representing 15 g of Carbohydrates and Number of People
With Improvement in Hypoglycemia Within 15 Minutes
Type of Dietary Sugar
Glucose tablets
Glucose solution*†
Glucose gel*‡
Cornstarch hydrolysate*§
Carbohydrates per
Serving
Measure Representing
15 g Carbohydrates*
Clinical Relief 15 Minutes or
Less After Ingestion
Varies
Varies
194/223 (87.0%)
1 g/10 mL
150 mL
5/6 (83.3%)
15 g of glucose in 40 g of
40% dextrose gel
15 g
2/6 (33.3%)
15 g cornstarch
15 g
4/5 (80%)
*Glucose solution, glucose gel, and hydrolysate were evaluated in 1 study.90
†15 g of glucose dissolved in 150 mL of water.
‡Hypostop, Novo Industries.
§15 g of cornstarch hydrolysate containing 2% to 3% glucose, 6% to 8% maltose, 89% to 92% oligosaccharides and
polysaccharides, and 0.15% protein (Glucides 19, Roquette Freres, Lestrem, France) diluted in 150 mL of water.
�Singletary et al
we identified very-low-quality evidence (downgraded for
risk of bias and imprecision) from 1 RCT90 with 6 diabetic
patients treated with orange juice and 6 treated with glucose
tablets that showed no benefit with glucose tablets, with the
MD (mmol/L) in blood glucose 15 minutes after ingestion
lower with orange juice than with glucose tablets (MD, −0.7;
95% CI, −1.55 to −0.15). Very-low-quality evidence (downgraded for risk of bias and imprecision) from 1 observational
study87 with 8 diabetic patients treated with orange juice and 9
treated with glucose tablets showed no difference in a diabetic
patient’s likelihood of having a 20-mg/dL increase in blood
glucose level 20 minutes after treatment with orange juice
compared with glucose tablets (RR, 0.48; 95% CI, 0.18–1.26).
For the critical outcome of time to resolution of symptoms,
the important outcome of risk of complications (eg, aspiration), and the low-priority outcome of hospital length of stay,
no human trials were found.
Downloaded from http://ahajournals.org by on May 27, 2020
Jelly Beans (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief
less in 15 minutes or less), we found very-low-quality evidence (downgraded for risk of bias and imprecision) from 1
RCT89 with 45 diabetic patients treated with jelly beans and 52
treated with glucose tablets that showed no difference in the
resolution of symptoms 15 minutes after treatment, whether
diabetic patients were treated with jelly beans or glucose tablets (RR, 0.85; 95% CI, 0.69–1.04). For the critical outcome
of time to resolution of symptoms, the important outcomes of
risk of complications (eg, aspiration) and blood glucose, and
the low-priority outcome of hospital length of stay, no human
trials were found.
Mentos (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief
in 15 minutes or less), we found very-low-quality evidence
(downgraded for risk of bias and imprecision) from 1 RCT89
with 48 diabetic patients treated with Mentos and 52 treated
with glucose tablets that showed no difference in the resolution of symptoms 15 minutes after treatment, whether diabetic
patients were treated with Mentos or glucose tablets (RR,
1.06; 95% CI, 0.92–1.21). For the critical outcome of time
to resolution of symptoms, the important outcomes of risk of
complications (eg, aspiration) and blood glucose, and the lowpriority outcome of hospital length of stay, no human trials
were found.
Milk (I) Compared With Glucose Tablets (C)
For the important outcome of blood glucose (diabetic patients
with at least a 20-mg/dL increase of blood glucose by 20 minutes), we found very-low-quality evidence (downgraded for
risk of bias and imprecision) from 1 observational study87 that
included 5 diabetic patients treated with whole milk and 9
treated with glucose tablets, showing no difference in likelihood of a 20-mg/dL increase in blood glucose level 20 minutes after treatment, whether diabetic patients were treated
with milk or glucose tablets (RR, 0.11; 95% CI, 0.01–1.62).
For the critical outcome of time to resolution of symptoms,
the important outcomes of risk of complications (eg, aspiration) and hypoglycemia, and the low-priority outcome of hospital length of stay, no human trials were found.
Part 9: First Aid
S285
Glucose Gel (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief in
15 minutes or less), we identified very-low-quality evidence
(downgraded for risk of bias and imprecision) from 1 RCT90
that included 6 diabetic patients treated with glucose gel and 6
treated with glucose tablets, finding no difference in the resolution of symptoms 15 minutes after treatment (RR, 0.5; 95%
CI, 0.14–1.77).
For the critical outcome of time to resolution of symptoms, the important outcomes of risk of complications (eg,
aspiration) and blood glucose, and the low-priority outcome
of hospital length of stay, no human trials were found.
Glucose Solution (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief in
15 minutes or less), we identified very-low-quality evidence
(downgraded for risk of bias and imprecision) from 1 RCT90
that included 6 diabetic patients treated with glucose solution
and 6 treated with glucose tablets, finding no difference in the
resolution of symptoms 15 minutes after treatment (RR, 1.25;
95% CI, 0.64–2.44).
For the critical outcome of time to resolution of symptoms, the important outcomes of risk of complications (eg,
aspiration) and blood glucose, and the low-priority outcome
of hospital length of stay, no human trials were found.
Cornstarch Hydrolysate (I) Compared With Glucose Tablets (C)
For the important outcome of hypoglycemia (clinical relief
in 15 minutes or less), we found very-low-quality evidence
(downgraded for risk of bias and imprecision) from 1 RCT90
that included 5 diabetic patients treated with cornstarch
hydrolysate 15 g and 6 treated with glucose tablets, finding
no difference in the resolution of symptoms 15 minutes after
treatment (RR, 1.20; 95% CI, 0.59–2.45).
For the critical outcome of time to resolution of symptoms, the important outcomes of risk of complications (eg,
aspiration) and blood glucose, and the low-priority outcome
of hospital length of stay, no human trials were found.
The following dietary sugars were evaluated in the
included studies:
• Skittles: ~90 g carbohydrate per 100 g, sugar (sucrose)
corn syrup, partially hydrogenated soybean oil, fruit
juice from concentrate (grape, strawberry, lemon, lime,
orange), citric acid, dextrin, natural and artificial flavors,
gelatin, food starch–modified coloring, ascorbic acid
• Fruit to Go: apple pure concentrate; apple, cherry, and
elderberry juice concentrates; wild berry concentrate
(concentrated cherry, raspberry, blueberry, cranberry and
boysenberry juices, natural flavor); citrus pectin; natural
flavor; lemon juice concentrate
• Mentos: 2.8 g carbohydrate in each mint (71% glucose
and 29% oligosaccharides), 91.6 g carbohydrate per 100
g, 69.3 g sugar per 100 g, sugar, glucose syrup (corn),
reconstituted fruit juices (strawberry, orange, lemon;
2.5%), hydrogenated vegetable oil (coconut), acid (citric
acid), rice starch, thickeners (gum arabic, gellan gum,
flavorings, glazing agent [carnauba wax]), emulsifier
(sucrose esters of fatty acids), colors
• Glucose gel: 15 g of glucose in 40 g of 40% dextrose gel
(Hypostop, Novo Industries)
�October 20, 2015
• Glucose solution: 15 g of glucose dissolved in 150 mL
of water
• Cornstarch hydrolysate: 15 g of cornstarch hydrolysate containing 2% to 3% glucose, 6% to 8% maltose,
89% to 92% oligosaccharides and polysaccharides, and
0.15% protein (Glucides 19, Roquette Freres, Lestrem,
France) diluted in 150 mL of water.
Treatment Recommendation
We recommend that first aid providers administer glucose tablets for treatment of symptomatic hypoglycemia in conscious
individuals (strong recommendation, low-quality evidence).
We suggest that if glucose tablets are not available, various
forms of dietary sugars such as Skittles, Mentos, sugar cubes,
jelly beans, or orange juice can be used to treat symptomatic
hypoglycemia in conscious individuals (weak recommendation, very-low-quality evidence).
There is insufficient evidence to make a recommendation
on the use of whole milk, cornstarch hydrolysate, and glucose
solution, or glucose gels as compared with glucose tablets for
the treatment of symptomatic hypoglycemia.
Downloaded from http://ahajournals.org by on May 27, 2020
Values, Preferences, and Task Force Insights
In making this recommendation, we acknowledge the likelihood that glucose tablets will not always be available and that
other dietary sugars are often more accessible.
In the 4 studies, most individuals had symptom improvement 10 to 15 minutes after treatment.
A rerun of the original literature search was performed
in January 2015. No new studies were identified that subsequently altered the treatment recommendation.
This review generated a number of excellent questions
within the ILCOR task forces and via public commenting.
Several of the comments asked if alternative forms of candy or
dietary sugars could be substituted for those listed in the tables.
Although alternative dietary sugars and candy may be effective in treating hypoglycemia, the forms of sugars listed in this
review are the specific dietary sugars that have been evaluated,
with the specific amount used (ie, number of candies or amount
of orange juice) equating to glucose 15 to 20 g. Those who
commented also asked if there is any harm from giving more
than the tested amount of dietary sugars. While this review did
not look at adverse effects of administering more sugar than
needed, it is well known that providing more sugar than needed
to diabetics with symptomatic hypoglycemia can lead to “overshooting” of blood glucose goals, which, when repeated over
time, may be as harmful as recurrent episodes of hypoglycemia.
Concern was expressed over administration of oral sugars
to diabetics with symptomatic hypoglycemia, particularly if
they have altered mental status. The recommendations made
by this task force apply to individuals with symptomatic hypoglycemia who are conscious, able to follow commands, and
able to swallow. If these criteria are not present, oral treatment
should be withheld because there is risk of aspiration, and
EMS (eg, 9-1-1 or 1-1-2) rescue services should be contacted.
The evidence reviewers for this topic were asked if some
guidance could be provided in terms of the time required for
resolution of symptoms of hypoglycemia after treatment using
dietary sugar supplements as tested, to help determine when
a repeat treatment may be necessary. For all tested dietary
A
3
2.5
Change in glucose (mmol/L)
Circulation
2
Glucose tablets
1.5
Just Juice (orange)
1
Jelly beans
Mentos dragees
0.5
0
t=0
t=2
t=5
t=10
t=15
Time (minutes)
B
Glucose (mmol/L)
S286
6
5
4
Glucose tablets
3
Just Juice (orange)
2
Jelly beans
1
Mentos dragees
0
t=0
t=2
t=5
t=10
t=15
Time (minutes)
Figure 3. Change in blood glucose from baseline for 4 treatment
groups. A, Mean change in blood glucose from baseline by time
for 4 treatment groups (P=0.034 at 10 minutes and P=0.005
at 15 minutes, respectively, between groups). B, Mean blood
glucose by time for 4 treatment groups (P=0.099 at 10 minutes
and P=0.026 at 15 minutes, respectively, between groups). From
McTavish L, Wiltshire E. Effective treatment of hypoglycemia in
children with type 1 diabetes: a randomized controlled clinical
trial. Pediatr Diabetes. 2011;12:381–387.89
sugars, blood glucose levels did not improve substantially
until 10 to 15 minutes after treatment (Figure 3).
Glucose gels and paste are not directly equivalent to oral
glucose tablets in terms of dosing and absorption, and, therefore, we did not include them in the control arm of this review.
Instead, these agents were included as interventions compared
with glucose tablets, with the finding of a single study with a
very small number of subjects, showing them to be suboptimal
as compared with oral glucose tablets. The task force strongly
believes that further studies are needed with glucose gels and
paste to determine if they are absorbed through the buccal
mucosa or sublingually (versus swallowed), and to determine
any dose equivalence to glucose tablets. We are aware of studies evaluating dextrose spray, gel, or paste for neonates or
children, but without a glucose tablet comparison; thus, these
studies were excluded from this review.
Knowledge Gaps
More evidence and well-designed studies are needed regarding
• Complications associated with various oral hypoglycemia treatment options
length of stay for various oral hypoglycemia
treatment options
• Other dietary forms of sugars that patients or providers may have readily available (eg, high-fructose syrup
drinks or soda pop soft drinks)
• Glucose gels, pastes, and spray
• Dietary sugar snacks containing gelatin (jelly beans, jelly
lollies, or candies), honey, and sweetened condensed milk
• Hospital
�Singletary et al
Exertion-Related Dehydration and Oral
Rehydration (FA 584)
Among adults and children with exertion-related dehydration
(P), does drinking oral carbohydrate-electrolyte (CE) liquids
(I), compared with drinking water (C), change volume/hydration status, vital signs, development of hyperthermia, development of hyponatremia, need for advanced medical care, blood
glucose, patient satisfaction (O)?
Downloaded from http://ahajournals.org by on May 27, 2020
Introduction
A review of this topic was performed in 2010 and concluded
that CE beverages are recommended for rehydration of individuals who become dehydrated through sweating in hot
climates and/or exercise. For the 2015 review, the task force
used an extensive literature search combined with GRADE
methodology, resulting in a much larger number of included
studies. In addition, we included several alternative beverages
with varying CE content compared with water. The authors
of some included studies noted that a relatively lower urine
volume is considered an indicator for increased intravascular volume during the immediate postexercise rehydration
period.86,89,91 The physiologic basis of this relates to a fall in
plasma osmolality and sodium concentration with plain water
ingestion after exercise, which stimulates urine production
and reduces the stimulus to drink, both of which delay the
rehydration process. Addition of sodium chloride to plain
water has been shown to increase fluid intake while reducing urine output. Thus, for this review, a lower urine output
in the first several hours after ingestion of studied fluids is
considered a beneficial effect for rehydration. The rehydration index is an indication of how much of the fluid ingested
was actually used in body weight restoration,92,93 with a lower
number reflecting a higher amount of ingested fluid used in
body weight restoration.
Consensus on Science
After the application of inclusion and exclusion criteria to the
1751 initial citations, a total of 12 studies were included. A
summary of the evidence from these 12 studies is provided
(Table 3).
12% CE Solution (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified very-low-quality evidence (downgraded for risk of
bias and imprecision) from 1 RCT91 with 30 subjects showing a benefit with the use of CE solution, with increased fluid
retention (%) at 2 hours after exercise (MD, 16.1; 95% CI,
7.45–24.75).
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, and
development of hyponatremia, or the important outcomes of
blood glucose, need for advanced medical care, and patient
satisfaction.
5% to 8% CE Solution (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified low-quality evidence (downgraded for risk of
bias and imprecision) from 8 studies including 204 subjects
showing an overall benefit to 5% to 8% CE solution compared with water in 10 of 15 outcomes, and 5 of 15 showing
no difference:
• Very-low-quality
Part 9: First Aid
S287
evidence (downgraded for imprecision) from 1 observational study94 with 38 subjects
showing at 2 hours after hydration no difference for body
weight loss (kg) with CE solution compared with water,
a benefit with CE solution with increased rehydration
(%) (MD, 8; 95% CI, 6.09–9.91), and a benefit with CE
solution for increased blood volume response (%) (MD,
2.8; 95% CI, 2.26–3.34).
• Moderate-quality evidence (downgraded for imprecision) from 1 RCT95 with 18 subjects showing no benefit
for CE solution compared with water for rehydration (%)
at 4 hours after hydration (MD, −1.6; 95% CI, −11.12
to 7.92).
• Very-low-quality evidence (downgraded for risk of bias
and imprecision) from 2 RCTs91,96 with 54 subjects
showing no difference in fluid retention (%) at 2 hours
after hydration for CE solution compared with water;
low-quality evidence (downgraded for risk of bias and
imprecision) from 2 RCTs96,97 with 44 subjects showing
a benefit of CE solution for increased fluid retention (%)
at 3 hours (MD, 15.6; 95% CI, 12.44–18.8); very-lowquality evidence (downgraded for imprecision) from 1
observational study98 with 26 subjects showing a benefit with CE solution for increased fluid retention (%)
at 3 hours (MD, 21.7; 95% CI, 9.89–33.51); very-lowquality evidence (downgraded for imprecision) from 1
observational study99 with 26 subjects showing a benefit
with CE solution for increased fluid retention (%) at 4
hours (MD, 22; 95% CI, 9.6–34.4); low-quality evidence
(downgraded for risk of bias and imprecision) from 1
RCT100 with 22 subjects showing no difference in fluid
retention (%) at 4 hours.
• Low-quality evidence (downgraded for risk of bias
and imprecision) from 1 RCT97 with 20 subjects
showing a benefit with CE solution compared with
water with decreased mean urine volume by weight
(g) between 1 and 2 hours after hydration (MD, −175;
95% CI, −206.37 to −143.63) and a benefit of CE
solution with decreased mean urine volume between
2 and 3 hours after hydration (MD, −41; 95% CI,
−64.27 to −17.73); very-low-quality evidence (downgraded for imprecision) from 1 observational study94
with 38 subjects showing at 2 hours after hydration
a benefit with CE solution with decreased mean
urine volume (mL) (MD, −160; 95% CI, −198.15 to
−121.85); very-low-quality evidence (downgraded
for imprecision) from 1 observational study98 with
26 subjects showing a benefit with CE solution
with decreased mean urine volume (mL) at 3 hours
after hydration (MD, −465.3; 95% CI, −700.73 to
−229.87); low-quality evidence (downgraded for risk
of bias and imprecision) from 1 RCT100 with 22 subjects showing no difference for mean urine volume
(mL) at 4 hours after hydration; and very-low-quality
evidence (downgraded for imprecision) from 1 observational study99 with 26 subjects showing a benefit
with CE solution with decreased mean urine volume
(mL) at 4 hours after hydration (MD, −277; 95% CI,
−458.26 to −95.74).
• Very-low-quality evidence (downgraded for imprecision) from 1 observational study98 with 26 subjects
�S288
Circulation
Table 3.
Effectiveness/Beneficial Effects of Various Rehydration Solutions
Fluid
October 20, 2015
PICO Outcome
Studies (RCT/Obs)
Subjects
Benefit CE
12% CE
Volume/hydration status
1 (1/0)
30
1
5%–8% CE
Volume/hydration status
8 (5/3)
204
10
No Difference
Benefit Water
Total Outcomes
1
5
15
5%–8% CE
Vital signs
3 (2/1)
86
5
5
5%–8% CE
Hyperthermia
1 (1/0)
36
1
1
5%–8% CE
Hyponatremia
1 (1/0)
18
3
5%–8% CE
Advanced medical care
1 (1/0)
18
3
5%–8% CE
Patient satisfaction
2 (1/1)
50
3%–4% CE
Volume/hydration status
3 (3/0)
66
3
3%–4% CE
3
3
8
3
Patient satisfaction
2 (2/0)
36
1
3
Coconut water
Volume/hydration status
3 (3/0)
60
3
1
Coconut water
Patient satisfaction
2 (2/0)
44
2
2
Volume/hydration status
1 (1/0)
20
3
Patient satisfaction
1 (1/0)
20
1
Volume/hydration status
1 (1/0)
12
1
3% Na + Coconut water
3% Na + Coconut water
Coconut water (conc)
Coconut water (conc)
Vital signs
1 (1/0)
24
Coconut water (conc)
Patient satisfaction
1 (1/0)
24
Green tea- 4.2% CE
4
4
1
5
3
1
1
2
1
1
2
Blood glucose
1 (0/1)
48
Volume/hydration status
1 (0/1)
26
2
Lemon tea-CE
Vital signs
1 (0/1)
26
1
Lemon tea-CE
Patient satisfaction
1 (0/1)
26
2
Lemon tea-CE
8
1
2
1
4
2
1
4
6
Chinese tea - caffeine
Volume/hydration status
1 (1/0)
20
2% Milk
Volume/hydration status
1 (1/0)
22
2
4
2
2% Milk + Na/K
Volume/hydration status
1 (1/0)
22
2
2
Downloaded from http://ahajournals.org by on May 27, 2020
CE indicates carbohydrate-electrolyte; conc, from concentrate; K, potassium; Na, sodium; Obs, observational; PICO, population, intervention, comparator, outcome;
and RCT, randomized controlled trials.
showing no difference in plasma volume change (%) at 3
hours after hydration with CE solution; 1 observational
study of very-low-quality evidence99 (downgraded for
imprecision) with 26 subjects showing a benefit with CE
solution with increased plasma volume change (%) at 4
hours (MD, 11; 95% CI, 9.42–12.58).
For the critical outcome of vital signs, we identified the
following:
• Very-low-quality
evidence (downgraded for imprecision) from 1 observational study99 with 26 subjects
showing no significant difference for HR (BPM) at 1
hour after hydration and at 3 hours after hydration with
CE solution.
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT101 with 36 subjects showing no
difference in HR (BPM) 20 minutes after hydration or
respiratory rate (BPM) 20 minutes after hydration with
CE solution.
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT96 with 24 subjects showing no
benefit with CE solution for HR (BPM) at 3 hours after
hydration (MD, 7; 95% CI, −0.02 to 14.02).
For the critical outcome of development of hyperthermia, we identified low-quality evidence (downgraded for
risk of bias and imprecision) from 1 RCT101 with 36 subjects
showing no difference in core temperature (°C) after hydration with CE solution compared with water.
For the critical outcome of development of hyponatremia (a potential complication of endurance exercise), we
identified moderate-quality evidence (downgraded for imprecision) from 1 RCT95 with 18 subjects showing an increased
serum sodium (mmol/L) at 2 hours after hydration (MD, 3;
95% CI, 2.08–3.92), at 3 hours (MD, 3; 95% CI, 2.08–3.92),
and at 4 hours after hydration (MD, 4; 95% CI, 3.08–4.92)
with CE solution compared with water.
We did not identify any evidence to address the important
outcome of need for advanced medical care.
For the important outcome of patient satisfaction, we
identified the following:
• Very-low-quality
evidence (downgraded for imprecision) from 1 observational study95 with 26 subjects
showing no difference in abdominal discomfort ratings (1–10) with CE solution compared with water at
2, 3, and 4 hours after hydration, and no difference in
stomach fullness ratings (1–10) at 2, 3, or 4 hours after
hydration.
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT96 with 24 participants showing
no difference in stomach upset ratings (1–5) at 2 or 3
hours after hydration with CE solution compared with
water.
�Singletary et al
We did not identify any evidence to address the important
outcome of blood glucose.
3% to 4% CE Solution (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified the following:
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 2 RCTs92,93 with 36 subjects showing
no difference in the rehydration index for CE solution
compared with water.
• Very-low-quality evidence (downgraded for risk of bias
and imprecision) from 3 RCTs91–93 with 66 subjects
showing a benefit with CE solution with increased fluid
retention (%) at 2 hours after hydration (MD, 8.97; 95%
CI, 7.54–10.4).
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT93 with 20 subjects showing a
benefit of CE solution with decreased cumulative urine
output (mL) at 2 hours into the hydration period (MD,
−174.5; 95% CI, −220.89 to −128.11).
For the important outcome of patient satisfaction, we
identified the following:
• Low-quality evidence (downgraded for risk of bias and
Downloaded from http://ahajournals.org by on May 27, 2020
imprecision) from 1 RCT93 with 20 subjects showing no
difference for nausea scores (1–5) at 90 minutes after
hydration with CE solution, and low-quality evidence
(downgraded for risk of bias and imprecision) from 2
RCTs92,93 with 36 subjects showing no difference for
nausea scores (1–5) at 2 hours for CE solution compared
with water.
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT93 with 20 subjects showing no
difference for stomach upset scores (1–5) at 90 minutes
after hydration with CE solution compared with water,
and low-quality evidence (downgraded for risk of bias
and imprecision) from 2 RCTs92,93 with 36 subjects
showing a benefit with CE solution with a decrease in
stomach upset scores (1–5) at 2 hours after hydration
(MD, −0.3; 95% CI, −0.45 to 0.16).
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, and
development of hyponatremia, or the important outcomes of
blood glucose and need for advanced medical care.
Coconut Water (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified the following:
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 2 RCTs92,93 with 36 subjects showing no difference in rehydration index for coconut water
compared with water.
• Very-low-quality evidence (downgraded for risk of bias
and imprecision) from 3 RCTs92,93,96 with 60 subjects
showing a benefit with coconut water with increased
fluid retention (%) at 2 hours after hydration (MD, 5.81;
95% CI, 4.35–7.27), and very-low-quality evidence
(downgraded for risk of bias and imprecision) from 1
RCT96 with 24 subjects showing no difference in fluid
Part 9: First Aid
S289
retention (%) at 3 hours after hydration with coconut
water compared with water.
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT93 with 20 subjects showing a
benefit with coconut water with decreased cumulative
urine output (mL) at 2 hours into the hydration period
(MD, −76.9; 95% CI, −120.34 to −33.46) compared with
water.
For the important outcome of patient satisfaction, we
identified the following:
• Low-quality evidence (downgraded for risk of bias and
imprecision) from 1 RCT93 with 20 subjects showing no
difference for nausea scores (1–5) with coconut water
compared with water at 90 minutes after hydration and
at 2 hours.
• Low-quality evidence (downgraded for risk of bias
and imprecision) from 1 randomized trial93 with 20
subjects showing a benefit with coconut water with
a decrease in stomach upset scores (1–5) at 90 minutes after hydration (MD, −0.4; 95% CI, −0.54 to
−0.26), very-low-quality evidence (downgraded for
risk of bias and imprecision) from 2 RCTs93,96 with
44 subjects showing benefit with coconut water with
a decrease in stomach upset scores (1–5) at 2 hours
after hydration (MD, −0.41; 95% CI, −0.55 to −0.28),
and very-low-quality evidence (downgraded for risk
of bias and imprecision) from 1 RCT96 with 24 subjects showing no benefit with coconut water with an
increase in stomach upset scores (1–5) at 3 hours after
hydration with the coconut water compared with water
(MD, 1.84; 95% CI, 1.08–2.6).
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, or
development of hyponatremia, or the important outcomes of
blood glucose or need for advanced medical care.
3% Sodium Plus Coconut Water (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified low-quality evidence (downgraded for risk of bias
and imprecision) from 1 RCT93 with 20 subjects showing a
benefit with 3% sodium plus coconut water compared with
water, with a decreased rehydration index (MD, −0.7; 95%
CI, −0.81 to −0.59), a benefit with 3% sodium plus coconut
water with increased retained fluid (%) at 2 hours after hydration (MD, 10.5; 95% CI, 9.09–11.91), and a benefit with 3%
sodium plus coconut water with decreased urine volume (mL)
at 2 hours after hydration (MD, −150.3; 95% CI, −187.39 to
−113.21).
For the important outcome of patient satisfaction, we
identified low-quality evidence (downgraded for risk of bias
and imprecision) from 1 randomized trial93 with 20 subjects
showing a benefit with 3% sodium plus coconut water compared with water, with less nausea (1–5) at 90 minutes after
hydration (MD, −0.2; 95% CI, −0.38 to −0.02).
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, and
development of hyponatremia, or the important outcomes of
blood glucose or need for advanced medical care.
�S290
Circulation
October 20, 2015
Coconut Water From Concentrate (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified very-low-quality evidence (downgraded for risk of
bias and imprecision) from 1 RCT96 with 24 subjects showing
no difference in mean fluid retention at 120 minutes after exercise (MD, 10.7; 95% CI, −6.39 to 27.79) for coconut water
from concentrate compared with water, but higher mean fluid
retention with coconut water at 180 minutes after exercise
(MD, 17; 95% CI, 0.86–33.14).
For the critical outcome of vital signs, we identified verylow-quality evidence (downgraded for risk of bias and imprecision) from 1 RCT96 with 24 subjects showing no difference
in mean HR (BPM) at 180 minutes after exercise with coconut
water from concentrate compared with water.
For the important outcome of patient satisfaction, we
identified very-low-quality evidence (downgraded for risk of
bias and imprecision) from 1 RCT96 with 24 subjects showing
no difference in mean stomach upset score (1–5) for coconut
water from concentrate compared with water at 120 minutes
(MD, 1.84; 95% CI, 0.91–2.77) and at 180 minutes (MD,
1.47; 95% CI, 0.6–2.34).
We did not identify any evidence to address the critical
outcomes of development of hyperthermia or development of
hyponatremia, or the important outcomes of blood glucose or
need for advanced medical care.
Downloaded from http://ahajournals.org by on May 27, 2020
Green Tea–Based 4.2% CE Solution (I) Compared With
Water (C)
For the important outcome of blood glucose, we identified very-low-quality evidence (downgraded for risk of bias
and imprecision) from 1 observational study102 with 48 subjects showing that a green tea–based 4.2% CE solution was
associated with increased mean glucose (mg/dL) at 2 hours
after hydration compared with water (MD, 6.9; 95% CI,
1.59–12.21).
We did not identify any evidence to address the critical
outcomes of volume/hydration status, vital signs, development of hyperthermia, and development of hyponatremia, or
the important outcomes of need for advanced medical care
and patient satisfaction.
Lemon Tea–Based 12% CE (t-CE) Solution (I) Compared
With Water (C)
For the critical outcome of volume/hydration status, we
identified of very-low-quality evidence (downgraded for risk
of bias and imprecision) from 1 observational study99 with 26
subjects showing no difference in mean retained fluid (%) at
4 hours after hydration (MD, 6; 95% CI, −5.15 to 17.15) with
t-CE solution compared with water and no difference in mean
urine volume (mL) at 4 hours after hydration.
For the critical outcome of vital signs, we identified verylow-quality evidence (downgraded for risk of bias and imprecision) from 1 observational study99 with 26 subjects showing
no difference in mean HR (BPM) at 60 minutes after hydration with t-CE solution compared with water.
For the important outcome of patient satisfaction, we
identified very-low-quality evidence (downgraded for risk
of bias and imprecision) from 1 observational study99 with
26 subjects showing no difference in mean abdominal discomfort scores (1–10) at 120 minutes after hydration with
t-CE, no benefit with t-CE with an increase in abdominal
discomfort scores at 180 minutes (MD, 1.3; 95% CI, 0.69–
1.91), and no benefit with t-CE compared with water with an
increase in abdominal discomfort at 240 minutes; also, there
was no difference for mean stomach fullness scores (1–10)
with t-CE solution at 120 minutes after hydration, and no
significant difference for mean stomach fullness scores with
t-CE solution at 180 minutes or at 240 minutes as compared
with water.
We did not identify any evidence to address the critical
outcome of development of hyperthermia and development of
hyponatremia, or the important outcome of blood glucose and
need for advanced medical care.
Chinese Tea Plus Caffeine (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified low-quality evidence (downgraded for risk of
bias and imprecision) from 1 RCT97 with 20 subjects showing no difference with Chinese tea plus caffeine compared
with water in mean total body water loss (%), no difference
in mean fluid retention (%) at 3 hours after hydration, and
no significant difference in mean urine volume by weight (g)
between 60 and 120 minutes or between 120 and 180 minutes
after hydration.
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, or
development of hyponatremia, or the important outcomes
of blood glucose, need for advanced medical care, or patient
satisfaction.
Milk (2% Fat) (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified low-quality evidence (downgraded for risk of bias
and imprecision) from 1 RCT100 with 22 subjects showing a
benefit with milk (2% fat) compared with water at 4 hours
after hydration for fluid retention (%) (MD, 33; 95% CI,
24.64–41.36) and for urine volume (mL) (MD, −594; 95% CI,
−742.34 to −445.66).
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, or
development of hyponatremia, or the important outcomes
of blood glucose, need for advanced medical care, or patient
satisfaction.
Milk (2% Fat) Plus High Sodium (Na+) and Potassium (K+)
Concentration (I) Compared With Water (C)
For the critical outcome of volume/hydration status, we
identified low-quality evidence (downgraded for risk of bias
and imprecision) from 1 RCT100 with 22 subjects showing a
benefit with milk (2% fat) with high Na+/K+ concentration
compared with water at 4 hours after hydration for fluid retention (%) (MD, 36; 95% CI, 29.64–42.36) and benefit with
urine volume (mL) (MD, −655; 95% CI, −773.26 to −536.74).
We recognize that this beverage is not a standard commercial
product.
We did not identify any evidence to address the critical
outcomes of vital signs, development of hyperthermia, or
development of hyponatremia, or the important outcomes
of blood glucose, need for advanced medical care, or patient
satisfaction.
�Singletary et al
Treatment Recommendation
We suggest that first aid providers use 3% to 8% CE drinks for
treating exertion-related dehydration. If 3% to 8% CE drinks
are not available or not tolerated, alternative beverages for
rehydration include water, 12% CE solution, coconut water,
2% milk, tea, tea-CE, or caffeinated tea beverages (weak recommendation, very-low-quality evidence).
Values, Preferences, and Task Force Insights
In making this recommendation, we recognize that first aid
providers are commonly recruited to assist at first aid stations
located at sporting and challenge events and that exerciseinduced dehydration is a common problem. It may not be possible to determine the exact quantity or percent of fluid loss in
the first aid setting.
Public comment was made about the potential mortality
associated with ingestion of water only during ultramarathons.
The reviewers for this PICO question specifically looked at
sodium levels reported after rehydration in the included studies and agreed that oral rehydration with CE liquids may
assist in preventing hyponatremia, although this review did
not specifically address exercise-associated hyponatremia. In
addition, all included trials conducted exercise in a controlled
environment and time period. Extreme events such as ultramarathons were not included in the evidence evaluation.
Knowledge Gaps
How can a first aid provider determine the amount of liquid
required for rehydration?
Downloaded from http://ahajournals.org by on May 27, 2020
Eye Chemical Injury: Irrigation (FA 540)
Among adults and children who have a chemical or other
unknown substance enter the conjunctival sac (P), does irrigation with isotonic saline, balanced salt solution, or other
commercial eye irrigation solutions (I), compared with irrigation with water (C), change tissue healing, functional recovery, pain, complications, time to resumption of usual activity,
restoration to the preexposure condition, time to resolution of
symptoms (O)?
Introduction
The 2010 review of eye injuries focused on irrigation of eyes
after exposure to an unknown toxic substance, with a recommendation to use copious amounts of water unless a specific antidote is available. For 2015, the First Aid Task Force
looked at which solutions might be compared with water for
the management of ocular injuries from chemicals or other
substances. This use of water as a comparator made the literature search extremely difficult, and no human comparative trials were identified. Thus, animal studies were later introduced
into the search strategy, and 1 comparative animal study met
all our inclusion criteria.
Consensus on Science
Saline (I) Compared With Water (C)
For the critical outcome of pH level, studied as maximum pH
of the anterior chamber after alkali application to the cornea,
we identified very-low-quality evidence (downgraded for indirectness and imprecision) from 1 in vivo observational animal
study103 using the eyes of 16 rabbits divided into 4 groups of
Part 9: First Aid
S291
4 rabbits (8 eyes) in which twice normal sodium hydroxide
(2N NaOH) was applied to the corneas, demonstrating benefit
(ie, in reduction of the high, alkaline pH) with irrigation using
water, including
• A statistically significant higher maximum pH when irrigating with 0.5 L of 0.9% normal saline versus 0.5 L of
tap water (MD, 0.62; 95% CI, 0.25–0.99)
• A statistically significant higher maximum pH when irrigating with 1.5 L of 0.9% normal saline versus 0.5 L tap
water (MD, 0.57; 95% CI, 0.035–1.105)
• A statistically significant higher maximum pH when irrigating with 0.5 L of 0.9% normal saline versus 1.5 L of
tap water (MD, 0.5; 95% CI, 0.119–0.881)
No significant difference in maximum pH was found after
irrigation using 1.5 L of 0.9% normal saline versus 1.5 L of
tap water (MD, 0.45; 95% CI, −0.09 to 0.994).
We did not identify any evidence to address the outcomes
of intraocular penetration, risk of secondary glaucoma, corneal thickness (swelling), or intraocular pressure.
Treatment Recommendation
We suggest that first aid providers use continuous, large volumes of clean water for irrigation of chemical eye injuries
(weak recommendation, very-low-quality evidence).
We did not identify any studies evaluating the use of irrigation for other substances entering the eye comparing irrigation solutions with water.
Values, Preferences, and Task Force Insights
In making this recommendation, we value the preservation of
vision.
We recommend that the local poison center be called to
assist with identification of any chemical involved in an ocular injury. Because of the dangers associated with chemical
eye injuries, a healthcare professional should evaluate these
injuries immediately.
Public comments expressed concern that our recommendation could be made based on a single animal study. This is
a valid concern. However, although the included animal study
is of a very-low-quality evidence, it is important because it
demonstrates the extreme caustic nature of an alkali injury
to the cornea and the need to irrigate with large volumes of
water. The included study showed persistently high pH levels
of the alkali-injured corneas at 3 hours after irrigation with
1.5 L of either saline or water. Thus, based on this single
study, we again recommend continuous irrigation of corneal
injuries caused by alkaline substances with clean or tap water
and to continue until a healthcare professional evaluates the
injury and determines that the pH of the eye has returned to
normal.
Knowledge Gaps
Well-designed studies are needed to evaluate
• Irrigation with commercial eye-rinsing solutions versus
tap water (controlled trial)
• Comparison between different types of commercial eyerinsing solutions and tap water, including irrigation times
• Civilian first aid setting
• Control for confounders, type of toxin, or other substance
�S292
Circulation
October 20, 2015
First Aid Trauma Emergencies
Important trauma topics reviewed for 2015 included the first
aid management of hemorrhage, angulated fractures, open
chest wounds, burns (cooling of burns and burn dressings),
and dental avulsion. Two additional important trauma topics
were cervical spinal motion restriction and the recognition of
concussion by first aid providers.
The correct management of hemorrhage and the enhancement of hemostasis in the first aid setting are essential to
maintaining the circulating blood volume in acute trauma.
Three PICO reviews focused on critical interventions for
severe bleeding:
• There
was inadequate evidence to support the use of
proximal pressure points or limb elevation to control
bleeding. The use of localized cold therapy is suggested
for closed bleeding in extremities to aid hemostasis, but
there was no evidence to support this therapy for open
bleeding (Revised).
• The use of hemostatic dressings in first aid is supported
when standard first aid hemorrhage control (eg, direct
wound pressure) fails to control severe bleeding or cannot be applied (Revised).
• Similarly, the evidence supports the use of tourniquets in
the civilian setting when standard first aid hemorrhage
control (eg, direct wound pressure) fails to control severe
external limb bleeding (Revised).
Downloaded from http://ahajournals.org by on May 27, 2020
The task force recognized that the use of hemostatic dressings and tourniquets will have cost and training implications.
However, the task force thought that these costs would be
moderate and justified considering the benefit of maintaining
circulating blood volume in the management of trauma.
• There was no evidence to support the straightening of an
angulated fracture in the first aid situation, and the task
force did not make a recommendation. The task force
recognized the need to protect the victim from further
injury by splinting the fracture in position to reduce
pain or to enable safe extrication and transportation
(Revised).
• The application of an occlusive dressing or device by
first aid providers to an open chest wound may lead to an
unrecognized tension pneumothorax. The task force suggested that these wounds be left open with local control
of bleeding rather than risk occlusion (New).
• There is a growing body of scientific evidence showing
complications related to use of cervical collars. When
combined with concern for potential secondary injury
due to neck movement during attempts to apply a collar, this has led to a suggestion (weak recommendation)
against the use of cervical collars by first aid providers. The task force acknowledges that first aid providers may not be able to distinguish between high- and
low-risk criteria for spinal injuries, and recognizes the
possible need for alternative methods of cervical spine
motion restriction or stabilization, but these were not
formally reviewed. The task force believes that formal
spinal motion restriction in high-risk individuals is best
accomplished by trained emergency medical rescuers or
healthcare professionals (Revised).
• The
recognition of concussion after head trauma is a
common challenge of first aid. No simple concussion
scoring system was found that would assist the first aid
provider in making this important diagnosis; however,
there are more advanced scoring systems for use by
healthcare professionals (New).
• The correct first aid management of burns is critical to
their eventual outcome. Cooling burns is a widespread first
aid practice, but it is only supported by low-quality scientific evidence. No evidence was found as to the preferred
method of cooling, the temperature of the coolant, or the
duration of cooling. It was recommended that active cooling begin as soon as possible by using cool or nonfreezing
water or cooling adjuncts such as gel pads (Revised).
• A comparison of wet dressings with dry dressings for
thermal burns yielded no recommendation. There were
no studies comparing plastic wrap, considered a dry
dressing, with a wet dressing (Revised).
• It is widely recommended that an avulsed tooth be
replanted immediately in the conscious victim. However,
first aid providers may not have the skills or the willingness to undertake this procedure. This review suggests a
series of commercially available storage solutions and
simple household mediums, when available, for the
short-term storage of an avulsed tooth until reimplantation can be accomplished (New).
Control of Bleeding (FA 530)
Among adults and children with bleeding (P), does application of localized cold therapy, elevation of extremity, and/
or application of pressure over proximal pressure points (I),
compared with direct pressure alone (C), change overall mortality, hemostasis, major bleeding, complications, hospital
length of stay (O)?
Introduction
For 2015, this review compared direct pressure with either
localized cold therapy (such as a cold pack), elevation of an
extremity, or proximal pressure points. The absence of literature on all interventions except localized cold therapy, and
the interpretive caution required when generalizing results
from hospital to first aid settings, limited the treatment
recommendations.
Consensus on Science
For the critical outcome of mortality, we identified no
evidence.
For the critical outcome of hemostasis, we identified
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 RCT104 showing a benefit
in the reduction of femoral hematoma formation in post-PCI
patients receiving cold pack (vasoconstriction) compared with
sandbags (compression). This study enrolled 50 patients and
reported a statistically significant reduction in femoral hematoma formation, but no quantitative data were provided to
calculate the MD and CI. The publication included an illustration suggesting that cold compression reduced the size of the
hematoma by approximately 20 cm2 over 180 minutes in the
cold compression group and by less than approximately 10
cm2 in the compression-only group.
�Singletary et al
For the critical outcome of major bleeding, we identified
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 RCT,105 which enrolled 80
patients who underwent total knee arthroplasty and reported
an MD in calculated total body blood loss in the cold compression group of 610 mL (95% CI, 415.6–804.4) and an MD
in extravasation of 357 mL (95% CI, 184.6–529.3).
For the important outcome of complications, we identified
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 RCT105 showing a nonsignificant reduction in complications of the occurrence of deep
vein thrombosis in the cold compression group (1/60 knees)
compared with the non–cold compression group (2/40 knees).
For the important outcome of hospital length of stay, we
identified no evidence.
Treatment Recommendation
We suggest that localized cold therapy with or without pressure may be beneficial in hemostasis for closed bleeding
in extremities (weak recommendation, very-low-quality
evidence).
There is inadequate evidence to make a treatment recommendation concerning the use of proximal pressure points,
localized cold therapy for external bleeding, or the elevation
of an extremity for control of bleeding.
Downloaded from http://ahajournals.org by on May 27, 2020
Values, Preferences, and Task Force Insights
In making this weak recommendation, we do so cautiously
because we are generalizing results from the healthcare setting to the first aid setting.
Public comments on this topic expressed concern about
the application of localized cold therapy to pediatric patients
and the risk of hypothermia. The task force thought that local
application of cold therapy to an area of closed bleeding, such
as a bruise or hematoma, is intended to be directed at a relatively small, limited-size injury and would not result in hypothermia (eg, an instant cold pack applied to a bruise).
Knowledge Gaps
There is a paucity of literature comparing different bleedingcontrol strategies commonly used by first aiders. Studies
assessing the relative effectiveness of cold therapy, elevation
of an extremity, and proximal pressure in addition to manual
compression in the first aid setting are needed, as are studies
assessing the effectiveness of combining these strategies with
other interventions such as hemostatic agents and tourniquets.
In addition, further research exploring how much pressure
is required to control bleeding by using a proximal pressure
point is required to determine if this is feasible by a first aid
provider.
Hemostatic Dressings (FA 769)
In patients with severe external bleeding (P), does the application of topical hemostatic dressings plus standard first aid
(I), compared with standard first aid alone (C), change overall
mortality, vital signs, hemostasis, complications, blood loss,
major bleeding, incidence of cardiac arrest (O)?
Introduction
Hemostatic dressings are commonly used to control bleeding
in the surgical and military settings. Early-generation powder
Part 9: First Aid
S293
or granular hemostatic agents were poured directly into the
wound and were associated with exothermic reactions that
could exacerbate tissue injury. These products have improved
in recent years, and hemostatic agent–impregnated dressings
are now believed to be associated with fewer adverse effects.
Their use in the civilian setting is becoming more common.
The objective of this review was to evaluate the current
evidence for the use of hemostatic dressings and to identify
if their use by first aid providers can be safely recommended.
Consensus on Science
For the critical outcome of overall mortality, we identified
very-low-quality evidence (downgraded for risk of bias and
indirectness) from 1 human case series106 enrolling 26 patients,
demonstrating that 7.7% of patients with hemostatic dressings
(2/26) died (no comparison group). We also identified verylow-quality evidence (downgraded for indirectness) from
7 animal RCT studies107–113 showing benefit, where 29.1%
(25/86) of subjects who were treated with hemostatic dressings died, compared with 65.8% (54/82) who were not treated
with hemostatic dressings (RR, 0.44; 95% CI, 0.31–0.64).
For the critical outcome of hemostasis, very-low-quality
evidence (downgraded for risk of bias, indirectness, and imprecision) from 4 human case series106,114–116 enrolling 130 participants demonstrated that hemostasis occurred in 90.8% of
participants (118/130) (no comparison group). We also identified very-low-quality evidence (downgraded for risk of bias,
indirectness, and imprecision) from 3 animal studies112,113,117
showing benefit where hemostasis occurred in 74.2% (23/31)
who were treated with hemostatic dressings, compared with
50% (13/26) who were not treated with hemostatic dressings
(RR, 1.48; 95% CI, 0.96–2.30).
For the critical outcome of complications, very-lowquality evidence (downgraded for indirectness and imprecision) from 4 human case series studies106,114–116 enrolling 96
participants demonstrated that complications from hemostatic
dressings occurred in 3% of participants (3/96) (no comparison group).
For the important outcome of time to bleeding cessation,
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 human case series114 demonstrated that 73% of participants (25/34) achieved hemostasis
in under 3 minutes after a hemostatic dressing was applied (no
comparison group).
Treatment Recommendation
We suggest hemostatic dressings be used by first aid providers
when standard first aid hemorrhage control (including direct
pressure with or without a dressing) cannot control severe
external bleeding (weak recommendation, very-low-quality
evidence).
Values, Preferences, and Task Force Insights
In making this recommendation, we place increased value on
the benefits of hemostasis, which outweigh the risks (including infection and/or burns). The cost of the intervention is
moderate.
This PICO question specifically addressed hemostatic
dressings and does not apply to other agents (such as granules)
that may be applied alone or followed by a gauze dressing.
�S294
Circulation
October 20, 2015
A rerun of the literature search performed in January 2015
found no new studies that would change the treatment recommendation or strength of recommendation.
The 2010 consensus on science treatment recommendation stated that application of topical hemostatic agents to
control life-threatening bleeding not controlled by standard
techniques was “reasonable,” although the best agents and the
conditions under which it should be applied were not known.
For 2015, it remains unclear when hemostatic dressings compared with other interventions, such as direct pressure with or
without gauze dressing and/or tourniquets, should be used for
the control of severe bleeding. However, the task force thinks
that hemostatic dressings may be of greatest use in severe
external bleeding in locations where a tourniquet cannot be
applied, or when a tourniquet is not available and standard
hemorrhage control (direct pressure with or without gauze
dressing) is not effective. Effective use of hemostatic dressings requires that first aid providers be trained in proper application techniques.
Knowledge Gaps
More research is required to establish how much training is
required and what type of training should be used for first aid
providers to apply hemostatic dressings to bleeding wounds,
what should be used, and when it should be used. Specific
questions include
• Which specific hemostatic dressings should be used by
first aid providers?
Downloaded from http://ahajournals.org by on May 27, 2020
• In humans, how do hemostatic dressings compare with
properly applied standard first aid for effective bleeding
cessation, time to cessation, and complications?
• How do hemostatic dressings compare with tourniquet
application by first aid providers?
• Compared with standard hemorrhage control, does the
use of hemostatic dressings lead to differences in mortality in humans?
Use of a Tourniquet (FA 768)
Among adults and children with severe external limb bleeding
(P), does the application of a tourniquet (I), compared with not
applying a tourniquet (C), change hemostasis, overall mortality, vital signs, functional limb recovery, complications, blood
loss, incidence of cardiac arrest (O)?
Introduction
Tourniquets have been used in military settings for severe
external limb bleeding for many years. Various types of tourniquets have been used, including improvised and commercially available devices. Until recently, there have been little
data from the use of tourniquets in the civilian setting to establish their safety and effectiveness, and their use has remained
controversial.
In 2010, the evidence was reviewed for the following
questions: When direct pressure fails to stop bleeding, does
the application of a tourniquet improve outcome? In which
circumstances is the application of a tourniquet appropriate?
At that time, no studies were found on the use of tourniquets
to control hemorrhage in a civilian setting by first aid providers. However, evidence was reviewed from military settings.
In civilian settings, tourniquets were only recommended for
control of extremity hemorrhage if direct pressure is not adequate or possible (eg, multiple injuries, inaccessible wounds,
multiple victims). Further, specifically designed tourniquets
were found to be superior to improvised ones, but they could
be used only with proper training. There was insufficient evidence to determine how long a tourniquet could remain in
place safely.
The objective of the 2015 question was to review the current evidence in the prehospital setting on the use of tourniquets for control of severe external limb bleeding compared
with standard hemorrhage control (such as direct pressure
with or without a dressing) alone. Evaluated studies were
from both civilian EMS and military settings and included
a mix of commercial, improvised, and unspecified types of
tourniquets. The evidence remains unclear regarding which
type of tourniquet (improvised or commercially available)
or specific brand of tourniquet is most effective. The body of
literature on this topic is continuously growing and includes
large civilian series, but controlled studies with a comparison
group are lacking.
Consensus on Science
For the critical outcome of hemostasis, we identified lowquality evidence from 1 human study118 with a comparison
group enrolling 70 patients showing benefit where 83%
of those who had a tourniquet applied (35/42) achieved
hemostasis compared with 61% of those who did not
have a tourniquet applied (17/28) (RR, 10.54; 95% CI,
6.55–16.96), and very-low-quality evidence (downgraded
for risk of bias and indirectness) from 6 human case
series69,119–123 enrolling a total of 750 patients demonstrating that 74.7% of patients who had a tourniquet applied
(560/750) achieved hemostasis (MD not estimable because
control group was lacking).
For the critical outcome of mortality, we identified lowquality evidence (downgraded for risk of bias) from 3 human
studies118,124,125 with a comparison group enrolling 1768
patients showing no difference, where 12% of patients who
had a tourniquet applied (91/791) died compared with 9% of
patients who did not have a tourniquet applied (89/977) (RR,
1.08; 95% CI, 0.82–1.43) and 7 very-low-quality evidence
(downgraded for risk of bias) human case series120–122,126–129
enrolling 903 patients, where 10% of those patients who had a
tourniquet applied (92/903) died.
For the critical outcome of vital signs, we identified lowquality evidence (downgraded for risk of bias) from 3 human
studies with a comparison group118,124,125 enrolling 1642 participants demonstrating no benefit, with an MD in HR of 3 BPM
more (95% CI, 0.21–6.91) if a tourniquet was applied, and
low-quality evidence (downgraded for risk of bias and imprecision) from 2 human studies with a comparison group118,124
enrolling 284 participants demonstrating no benefit, with an
MD in SBP of 9 mm Hg less (95% CI, −14.13 to −3.43) if a
tourniquet was applied.
For the critical outcome of complications, low-quality
evidence (downgraded for risk of bias and imprecision)
from 1 human study with a comparison group118 enrolling 165 patients showed benefit to tourniquet application,
�Singletary et al
where 6% of patients who had a tourniquet applied (6/67)
had complications compared with 9% who did not have
a tourniquet applied (9/98) had complications (RR, 0.19;
95% CI, 0.06–0.55), and very-low-quality evidence (downgraded for risk of bias and imprecision) from 4 human case
series studies121,122,126,128 enrolling 846 patients documented
that complications from tourniquets occurred in 4.3% of
patients (36/846).
Treatment Recommendation
We suggest first aid providers use a tourniquet when standard
first aid hemorrhage control (including direct pressure with or
without a dressing) cannot control severe external limb bleeding (weak recommendation, low-quality evidence).
Downloaded from http://ahajournals.org by on May 27, 2020
Values, Preferences, and Task Force Insights
In making this recommendation, we place increased value on
the benefits of hemostasis, which outweigh the risks (such as
compartment syndrome, nerve palsy, or secondary amputation). The cost of the intervention is moderate.
The tourniquets used in the studies evaluated included a
mix of improvised and commercial devices. The maximum
length of time for leaving a tourniquet in place was not
reviewed.
The literature search was rerun in January 2015, and 2
additional studies were added to the consensus on science
and GRADE table, 1 from the military setting125 and 1 from
the civilian EMS setting,121 both supporting our treatment
recommendation.
The task force believes that application of a tourniquet will
be most effective and safe if the provider is trained with the
type(s) of tourniquet to be used and if the tourniquet is applied
properly and rapidly. Other situations when a tourniquet might
be used instead of direct pressure were discussed. Such situations are thought to include mass casualty incidents, an unsafe
scene, a complex or prolonged transfer, inability to access an
injury, and caring for someone with multiple injuries requiring
triage of injuries.
A major finding in this review is that the rate of adverse
events with tourniquet application is low, and the rate of successful hemostasis is high. However, we did not find a relationship between the application of tourniquet and improved
survival.
Knowledge Gaps
More research is required to establish how much training is
required and what type of training should be used for first aid
providers to apply tourniquets to bleeding wounds.
Specifically research should focus on
• Tourniquet
use versus no tourniquet versus double
tourniquet
• Use in the civilian setting
• Control for confounders, such as concurrent use of
hemostatic dressings
• For major external bleeding, a prospective registry study
would be useful, including a comparison between types
of tourniquets and between commercial tourniquets,
and including injury severity, provider types, time to
surgery, etc.
• Can instructions be given by EMS dispatchers?
Part 9: First Aid
S295
Straightening of an Angulated Fracture (FA 503)
Among adults and children who receive first aid for an angulated long bone fracture (P), does realignment of the fracture
prior to splinting (I), compared with splinting as found (C),
change neurologic injury, vascular injury, splinting, pain, time
to medical transportation (O)?
Introduction
Angulated extremity fractures vary in etiology and outcomes.
In some circumstances, the degree of angulation of a long
bone fracture may limit the ability to splint the extremity or
to move the patient. We sought to learn what outcomes may
result from attempts to gently realign a severely angulated
fracture to facilitate splinting or transportation. Understanding
outcomes from first aid procedures will help in developing
training.
Consensus on Science
For the question of straightening an angulated fracture, compared with splinting as found, the literature search initially
returned 458 citations. After application of inclusion and
exclusion criteria by title and abstract (inclusion: care provided before definitive treatment; exclusion: hospital settings,
use of analgesics), 9 studies were identified for full review.
Upon full review, all 9 studies were excluded because they did
not completely meet criteria for inclusion; thus, no evidence
was found to address the critical outcomes of neurologic
injury, vascular injury, or splinting, nor was there evidence for
the important outcome of pain.
There is no published evidence for or against the realignment of angulated long bone fractures as a first aid procedure
in terms of neurologic or vascular injury, pain, or time to medical transportation outcomes.
Treatment Recommendation
No recommendation; we found no evidence regarding the
risks and benefits of straightening an angulated fracture by
first aid providers.
Values, Preferences, and Task Force Insights
Consistent with the first aid principle of preventing further
harm, and based on training and circumstance, providers may
need to move an injured limb or person. In such situations,
first aid providers should protect the victim, which includes
splinting in a way that limits pain, reduces the chance for further injury, and facilitates safe and prompt transport.
Knowledge Gaps
As ethical and practical considerations prohibit RCTs, highquality non-RCTs comparing realignment versus nonrealignment are important. Describing confounders is important for
developing future outcomes to be studied. If or when realignment is appropriate, what instructions or training might be
given to first aid providers to optimize outcomes?
First Aid Treatment for an Open Chest
Wound (FA 525)
Among adults and children who are being treated for an open
chest wound outside of a hospital (P), does occlusive bandage
application or occlusive device (I), compared with a nonocclusive dressing (C), change or improve survival, respiratory
�S296
Circulation
October 20, 2015
arrest, oxygen saturation, vital signs, the rate of cardiac and
respiratory arrests, improve therapeutic endpoints (oxygenation and ventilation) (O)?
Introduction
This is a new PICO question for 2015. The management of an
open chest wound in the out-of-hospital setting is challenging.
The most worrisome issue is the improper use of an occlusive dressing or device that potentially could lead to a tension
pneumothorax. In this PICO question, we sought to compare
the effects of an occlusive measure as opposed to a nonocclusive measure in individuals being treated for an open chest
wound. Occlusion was the complete sealing of the wound,
and nonocclusion was the maintenance of an open wound in
communication with ambient air. In this review, we included
animal studies because human comparative studies could not
be identified.
Downloaded from http://ahajournals.org by on May 27, 2020
Consensus on Science
For the critical outcome of respiratory arrest, we identified
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 animal study130 showing
benefit from using a nonocclusive device (RR, 0.059; 95% CI,
0.004–0.874).
For the critical outcome of oxygen saturation, we identified very-low-quality evidence (downgraded for risk of bias,
indirectness, and imprecision) from 1 animal study130 showing
benefit from using a nonocclusive device (P<0.05, MD and CI
not available).
For the important outcome of therapeutic endpoint
(tidal volume), we identified very-low-quality evidence
(downgraded for risk of bias, indirectness, and imprecision)
from 1 animal study130 showing benefit from using a nonocclusive device in tidal volume (mL) (MD, 34.7; 95% CI,
28.8–40.6 mL).
For the important outcome of vital signs, we identified
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from the same animal study130
showing benefit from using a nonocclusive device in HR
(BPM) (MD, −32.0; 95% CI, −42.8 to 21.2) and respiratory
rate (respirations per minute) (MD, 3.0; 95% CI, 1.5–4.5).
Finally, for the important outcome of vital signs, we also
identified very-low-quality evidence (downgraded for risk
of bias, indirectness, and imprecision) from the same animal
study130 showing no significant benefit from using a nonocclusive device in MAP (mm Hg) (MD, 4.6; 95% CI, −0.4 to 9.6).
We did not identify any evidence to address the critical
outcome of survival. We did not identify any evidence to
address the important outcome of rate of cardiac and respiratory arrests.
Treatment Recommendations
We suggest against the application of an occlusive dressing or
device by first aid providers to individuals with an open chest
wound (weak recommendation, very-low-quality evidence).
Values, Preferences, and Task Force Insights
In making this recommendation, we place higher value on the
avoidance of the potential life-threatening complication of
tension pneumothorax, compared with other risks associated
with an open chest wound.
Public comments expressed concern about making a
recommendation based solely on a single animal study. The
task force took into consideration the potential life-threatening complication of an unrecognized tension pneumothorax
associated with the use of an occlusive dressing or device in
the first aid setting. In addition, the review recognized the
long-standing accepted clinical practice of treating a tension
pneumothorax by creating and maintaining an open communication between the pneumothorax and ambient air.
Furthermore, while this will require a change for some
in current teaching, there was recognition of the practicality
and acceptance in the first aid setting of leaving an open chest
wound exposed to ambient air without a dressing or seal.
The task force discussed the reality that many dressings,
both initially and over time, may themselves produce inadvertent partial or full occlusion and that this needs to be recognized as a serious potential complication.
Knowledge Gaps
• Does the application of nonocclusive dressings or chest
seals to patients with open chest wounds outside of a
hospital improve survival and the rates of cardiac arrest
and respiratory arrest (out-of-hospital or in-hospital)?
• Do nonocclusive chest seals differ in effects as compared
with nonocclusive dressings?
• Does the application of nonocclusive devices delay the
activation or transportation of EMS?
Cervical Spinal Motion Restriction (FA 772)
Among adults and children with suspected blunt traumatic
cervical spinal injury (P), does cervical spinal motion restriction (I), compared with no cervical spinal motion restriction
(C), change neurologic injury, complications, overall mortality, pain, patient comfort, movement of the spine, hospital
length of stay (O)?
Introduction
For more than 30 years, the cervical collar has been routinely
applied by healthcare providers for patients with suspected
cervical spine injury, with the aim of avoiding additional
injury due to movement of the victim. However, there is no
good quality evidence available showing clinical benefit of
this intervention for injured patients, and this practice is based
primarily on expert consensus and tradition. The 2010 consensus on science for the topic of spinal immobilization noted
that there were no published studies to support or refute the
benefit of spinal immobilization by first aid providers.10 For
2015, the task force evaluated all available evidence focused
on the use of cervical collars and/or sandbags relevant for
patients with blunt traumatic cervical spinal injury.
Consensus on Science
Cervical spinal motion restriction was defined as the reduction
or limitation of cervical spinal movement. This definition may
not be consistent with definitions used in some countries or
by some organizations. Spinal stabilization was defined as the
physical maintenance of the spine in a neutral position before
applying spinal motion restriction devices. This evaluation
was limited to mechanical cervical immobilization devices
�Singletary et al
accessible to first aid providers, including cervical collars and
sandbags with tape, but did not include spine boards.
Downloaded from http://ahajournals.org by on May 27, 2020
(Semi)rigid Collar (I) Compared With No Collar (C)
For the critical outcome of neurologic injury, we identified very-low-quality evidence (downgraded for risk of bias
and imprecision) from 1 nonrandomized study131 with 5138
motorcycle crash victims, showing no difference in neurologic injury (no significant difference according to the article;
however, we were unable to calculate the MD and CI, because
the mean and standard deviation (SD) of the intervention and
control group were not reported).
For the critical outcome of complications (intracranial
pressure), we identified low-quality evidence from 5 nonrandomized studies132–136 with 107 patients in total, showing increased intracranial pressure with the use of a cervical
collar (MD [mm Hg], 4.69; 95% CI, 1.95–7.43; MD [mm
H20], 20.48; 95% CI, 5.62–35.33). We also identified verylow-quality evidence (downgraded for indirectness) from 1
nonrandomized study137 with 42 healthy volunteers showing
increased intracranial pressure (MD [internal jugular vein
cross-sectional area], 0.19; 95% CI, 0.05–0.33) with the application of a cervical collar.
For the critical outcome of complications (tidal volume),
we identified very-low-quality evidence (downgraded for risk
of bias and imprecision) from 1 nonrandomized study138 with
38 patients, showing no decrease in tidal volume (a significant
decrease was reported in the publication; however, we were
unable to calculate the CI because the SD of the intervention
and control group was not reported).
For the important outcome of cervical spine movement,
we identified low-quality evidence from 1 nonrandomized
study139 with 18 head-injured children showing no significant
limitation of flexion (MD, −2.20; 95% CI, −7.75 to 3.35). For
the same outcome, we also identified very-low-quality evidence (downgraded for indirectness) from 13 nonrandomized
studies140–152 with 457 cadavers or healthy volunteers showing significant decrease in flexion, extension, lateral bending,
axial rotation, and flexion/extension (flexion: MD, −12.50;
95% CI, −13.13 to −11.87; extension: MD, −0.91; 95% CI,
−1.18 to −0.64; lateral bending: MD, −1.99; 95% CI, −2.33
to −1.65; axial rotation: MD, −4.73; 95% CI, −5.16 to −4.3;
flexion/extension: MD, −19.13; 95% CI, −19.89 to −18.36]).
Seven additional studies153–159 were not included in the final
analysis because they were missing data (mean and/or SD of
intervention and control group not reported).
For the important outcome of patient comfort, we identified very-low-quality evidence (downgraded for indirectness and imprecision) from 1 nonrandomized study158 with
26 healthy volunteers, showing no change in patient comfort score.
We did not identify any evidence to address the important
outcomes of overall mortality and pain and the less important
outcome of hospital length of stay.
Soft Collar (I) Compared With No Collar (C)
For the important outcome of cervical spine movement,
we identified very-low-quality evidence (downgraded for
indirectness) from 3 nonrandomized studies140,147,151 with 36
cadavers or healthy volunteers showing a significant decrease
Part 9: First Aid
S297
in flexion and axial rotation (flexion: MD, −3.04; 95% CI,
−5.64 to −0.4; axial rotation: MD, −9.07; 95% CI, −14.17 to
−3.96). The same studies showed no significant difference
in terms of limiting extension, flexion/extension, and lateral
bending.
We did not identify any evidence to address the critical
outcomes of neurologic injury and complications; the important outcomes of overall mortality, pain, and patient comfort;
and the less important outcome of hospital length of stay.
Sand Bags and Tape (I) Compared With No Motion
Restriction (C)
For the important outcome of cervical spine movement, we
identified very-low-quality evidence (downgraded for indirectness) from 1 nonrandomized study140 with 25 healthy volunteers showing a significant decrease in flexion, extension,
axial rotation, and lateral bending (flexion: MD, −35.60; 95%
CI, −38.69 to −32.51; extension: MD, −6; 95% CI, −9.53 to
−2.47; axial rotation: MD, −73.30; 95% CI, −75.99 to −70.61;
lateral bending: MD, −19.40; 95% CI, −21.62 to −17.18).
We did not identify any evidence to address the critical
outcomes of neurologic injury and complications; the important outcomes of overall mortality, pain, and patient comfort;
and the less important outcome of hospital length of stay.
Treatment Recommendations
We suggest against the use of cervical collars by first aid providers (weak recommendation, very-low-quality evidence).
Values, Preferences, and Task Force Insights
Consistent with the first aid principle of preventing further
harm, the potential benefits of applying a cervical collar do
not outweigh harms such as increased intracranial pressure
and the consequences of unnecessary neck movement.
We recognize that first aid providers might not be able to
discriminate between high- or low-risk individuals. We also
recognize the potential value of manual stabilization in certain
circumstances, but this was not evaluated in this review.
Task force discussion about this review included the recognition that, although evidence from the few studies that
are available comes primarily from healthy volunteers and
cadavers, there is a growing body of evidence demonstrating
harmful effects, such as the development of raised intracranial
pressure. In addition, there was concern expressed that the
process for application of a cervical collar by a first aid provider to an individual with cervical spinal trauma could result
in further injury. Application of a cervical collar requires
training and regular practice to be performed properly, and
such training may not be a component of every first aid course
curriculum. Another important discussion topic was whether a
first aid provider is able to distinguish between high- and lowrisk injury criteria. As a result of these concerns and the consensus on science findings, the task force suggests against the
routine application of cervical collars by first aid providers.
Knowledge Gaps
More evidence is needed on manual stabilization (using
hands/knees to restrict motion), trauma patients in the prehospital setting, high-risk versus low-risk patients, other forms of
physical cervical spinal stabilization, and implementation and
education. A review of the adverse effects as a consequence
�S298
Circulation
October 20, 2015
of application of a cervical collar could be interesting in the
future.
Concussion (FA 799)
Among adults and children with suspected head injury
without loss of consciousness (P), does use of a simple concussion scoring system (I), compared with standard first aid
assessment without a scoring system (C), change time to
recognition of the deteriorating patient, the likelihood of
a poor neurologic outcome, survival to 30 days with good
neurologic outcome, need for advanced medical care, time
to medical transportation, or likelihood of differentiating
between minor head contusion and more serious concussion (O)?
Introduction
This is a new topic for the 2015 consensus on science.
First aid providers are commonly faced with the need to
identify concussion. The identification of concussion can be
complex, and if concussion is missed, this can lead to a delay
in receiving proper postconcussion advice and a delay in formal assessment and definitive treatment that can result in lifechanging or even life-threatening consequences.
The task force sought to evaluate the effectiveness of early
clinical recognition of concussion by first aid providers using
a simple scoring system.
Downloaded from http://ahajournals.org by on May 27, 2020
Consensus on Science
For the critical outcome of likelihood of differentiating
between minor head contusion and more serious concussion (brain injury), we identified very-low-quality evidence
(downgraded for risk of bias and indirectness) from 1 observational study160 with 19 408 patients in a trauma registry using
a secondary analysis of rescoring prehospital Glasgow Coma
Scale (GCS) scores showing no significant difference between
a simple derived motor score versus the GCS score to determine brain injury.
For the important outcome of need for advanced medical care (neurosurgical intervention and emergency tracheal
intubation), we identified very-low-quality evidence (downgraded for imprecision) from 1 nonrandomized study160 with
19 408 patients in a trauma registry using a secondary analysis
of rescoring the prehospital GCS scores showing no significant difference between a simple derived motor score versus
the GCS score for neurosurgical intervention (MD, 0.04; 95%
CI, 0.01–0.09) and the need for emergency tracheal intubation
(MD, 0.05; 95% CI, 0.01–0.11).
For the critical outcome of change in time to recognition
of the deteriorating patient, for the important outcomes of survival to 30 days with good neurologic outcome, and for the
likelihood of a poor neurologic outcome, we did not identify
any evidence.
Treatment Recommendations
No recommendation; we acknowledge the role that a simple,
validated, single-stage concussion scoring system could play
in the first aid provider’s recognition and referral of victims
of suspected head injury. However, review of the available literature shows no evidence regarding the application of such
scoring systems by the first aid provider.
Values, Preferences, and Task Force Insights
Failure to properly recognize concussion can result in delay or
absence of referral for definitive evaluation and care or inappropriate release to activity, which has the potential to worsen
outcomes. We did identify concussion assessment tools currently recommended for use in sports medicine, but these
require a 2-stage assessment, before competition and after
concussion, and were thought to be inappropriate for use in
the standard first aid setting.
Our extensive search strategy yielded 1837 publications,
but subsequent review resulted in the selection of only 1 published manuscript. Despite the finding of 1 prehospital scientific publication supporting a simplified motor score, it was
decided that this single article, a retrospective observational
study where prehospital GCS scoring extracted from an urban
Level 1 trauma registry was rescored by using a 3-point simplified motor score and compared with 4 hospital-based outcomes, did not formally address the PICO question and was in
itself a very weak level of scientific evidence.
Many of the studies identified in our literature search
used the adult and pediatric GCS to grade concussion. The
GCS was designed as a tool for use by advanced prehospital
and hospital care providers, and it is not commonly used by
first aid providers. The task force thought that this was not
an appropriate tool to be used by first aid providers to assess
concussion.
Our search and analysis did not identify any evidence to
support or refute the use of a simplified scoring system, such
as Sport Concussion Assessment Tool (SCAT); the GCS; or
Alert, responds to Voice, responds to Pain, Unresponsive Scale
(AVPU), versus standard first aid without a scoring system. It
was thought that the serious consequences of not recognizing
concussion in the first aid environment warranted an approach
whereby any individual with a head injury and any alteration
of level of consciousness requires immediate evaluation by an
advanced healthcare provider or at a hospital.
Knowledge Gaps
• There
is a need for a clearer definition of concussion
supported by clinical data that can be used to support
assessment made in the first aid environment.
• There is a need for RCTs to access the efficacy of scoring systems as used by non–healthcare professionals in
prehospital environments.
• There is a need for RCTs to assess the efficacy of SCAT
in the clinical environment and whether it can be applied
to nonsport environments.
Cooling of Burns (FA 770)
Among adults and children with thermal injuries (P), does
active cooling of burns (I), compared with passive cooling
(C), change pain, complications, wound healing, need for
advanced medical care, patient satisfaction, rates of fasciotomy, depth or breadth of burn (O)?
Introduction
The evidence for the first aid care of thermal injuries is limited. For this review, we focused on human studies that used
active forms of cooling, defined as any method undertaken to
�Singletary et al
decrease local tissue temperature. Limited evidence was found
to support cooling of thermal injuries for decreasing the depth
of burns, decreasing the need for advanced medical care, and
improving healing times. It remains unclear what effect cooling may have on the potential for contamination or infection.
Downloaded from http://ahajournals.org by on May 27, 2020
Consensus on Science
After application of inclusion and exclusion criteria, the
search strategy yielded 1 single-blind RCT and 5 observational studies. One of the observational studies was withdrawn
from publication due to inconsistencies in data and was, therefore, withdrawn from the evidence review, leaving a total of 5
studies for inclusion.161–165
For the critical outcome of pain, 1 RCT and 1 observational study were found. Low-quality evidence (downgraded
for risk of bias) from a single RCT161 with 24 subjects showed
no benefit in reduction of tactile pain measurements in cooled
versus noncooled first-degree burns (MD undeterminable).
Low-quality evidence (downgraded for risk of bias) from a
prospective observational study162 with 48 subjects showed no
benefit in reduction of pain at 2, 4, and 24 hours in patients
with active cooling of burns caused by electric cardioversion
versus those without cooling (MD undeterminable).
For the important outcome of depth of burn, 1 RCT and
3 observational studies were found. Low-quality evidence
(downgraded for risk of bias) from a single RCT161 with 24
subjects showed no difference in the amount of erythema
between cooled and noncooled burns (MD undeterminable).
Low-quality evidence (downgraded for risk of bias) from a
prospective observational study162 with 48 patients showed
a reduction in the number and depth of burns in those with
cooling versus those without (12.5% versus 83.3%) (RR, 0.15;
95% CI, 0.05–0.44). Very-low-quality evidence (downgraded
for indirectness) from a retrospective observational study163
with 695 patients reported an association between superficial
burns and cooling and between deep burns and a lack of cooling (33.2% versus 48.5%) (RR, 0.68; 95% CI, 0.55–0.85).
Very-low-quality evidence (downgraded for risk of bias) from
a third observational study164 with 268 patients found no benefit in reducing depth of burns, as measured by the need for
skin grafting, in the cooling versus control group (9.4% versus
10.7%; RR, 0.88; 95% CI, 0.35–2.21).
Regarding the important outcome of need for advanced
medical care, 3 observational studies were identified. Verylow-quality evidence (downgraded for risk of bias) from 1
observational study164 with 268 patients showed no reduction
in the need for advanced medical care after scald burns (including number of follow-up visits and need for scar management)
for patients who received 20 minutes or more of cooling versus those who did not (scar management 20.8% versus 20.9%;
RR, 0.99; 95% CI, 0.55–1.78). Very-low-quality evidence
(downgraded for risk of bias, indirectness, and imprecision)
from another observational study165 comprising 125 patients
showed an association between the use of water for first aid
cooling of burns and decreased average length of hospital stay
(10.3 days versus 5.3 days) for patients with less than 20%
body surface area burns. It also showed a higher percentage
of inpatient stays of less than 10 days in patients receiving
first aid cooling of burns with water (88.5% versus 67.2%)
Part 9: First Aid
S299
(RR, 1.32; 95% CI, 1.09–1.6). In this study, adequate cooling
time was defined as 10 minutes or more. Very-low-quality evidence (downgraded for indirectness and imprecision) from a
third prospective observational study166 enrolling 244 patients
showed a benefit of cooling by demonstrating that a community and media campaign that increased use of first aid cooling
for burns from 40% to 59% was associated with a decreased
percentage of burns requiring hospital admission (64.4% precampaign versus 35.8% postcampaign) (RR, 0.55; 95% CI,
0.42–0.73).
Regarding the important outcome of wound healing, 1
observational study was found. Very-low-quality evidence
(downgraded for risk of bias) from a single observational
study164 showed no benefit in reducing re-epithelialization
time for patients who received 20 minutes or more of cooling
versus those who did not (MD undeterminable).
Regarding the critical outcome of complications, and the
low-priority outcomes of patient satisfaction and rates of fasciotomy, there were no human trials found.
Treatment Recommendations
We recommend that first aid providers actively cool thermal
burns (strong recommendation, low-quality evidence).
Values, Preferences, and Task Force Insights
In making this recommendation, we place higher value on
decreased burn depth over the potential risk of infection or
hypothermia.
• Method/temperature of cooling: Forms of active cooling
evaluated in this review included cool/cold nonfreezing
water and mechanical devices (eg, cold probes, cooled
gel pads), but there is no evidence to recommend a specific temperature or method of cooling.
• Time of cooling: Literature from this review suggests
that active cooling should take place as soon as possible
for a minimum of 10 minutes.
The risk of hypothermia from cooling large burns or in
special populations is also unknown and was a topic of discussion within the task force.
Knowledge Gaps
• When is a burn sufficiently large that cold application
creates risk of hypothermia?
• What is the optimal temperature of cold application for
cooling burns?
• What is the optimal cooling duration?
Wet Compared With Dry Burn Dressings (FA 771)
Among adults and children with thermal injuries (P), does
the use of a wet dressing (I), compared with dry dressing (C),
change complications, pain, tissue healing, need for advanced
medical care, patient satisfaction, rates of fasciotomy (O)?
Introduction
“Wet” and “dry” dressings were difficult to define for this
review. After careful consideration of the PICO wording and
the various available dressings that may be applied to a burn,
the First Aid Task Force thought that this question would
�S300
Circulation
October 20, 2015
benefit from a future revision to one that compares specific
dressings, rather than an arbitrary wet or dry categorization.
Downloaded from http://ahajournals.org by on May 27, 2020
Consensus on Science
There are no studies directly evaluating wet versus dry dressings in the first aid context. All studies were performed in a
healthcare professional setting, and caution should be used in
generalizing findings to the first aid situation.
For the critical outcome of complications (infection), we
identified low-quality evidence (downgraded for risk of bias,
imprecision, and indirectness) from 1 RCT enrolling 104 subjects with superficial burns167 showing benefit with application of honey compared with silver sulfadiazine–impregnated
gauze dressings, with resolution of infection at 7 days (RR,
12.40; 95% CI, 4.15–37.00). A second RCT enrolling 100
patients with partial thickness burns168 found benefit with
application of honey compared with potato peel dressings,
with resolution of infection at 7 days (absolute risk reduction,
0.90; 95% CI, 0.74–0.95).
We also identified very-low-quality evidence (downgraded
for risk of bias and imprecision) from a non-RCT169 with 262
enrolled patients with partial thickness burns of less than 15%
total body surface area, evaluating the difference in infection rates with a topical, nonpenetrating antibacterial agent
(Polysporin, wet; n=102); a topical, penetrating antibacterial
agent (silver sulfadiazine, wet; n=58); and a petrolatum gauze
dressing (Xeroform, dry; n=112). This study showed no statistically significant difference in infection rate for the silver
sulfadiazine wet dressings compared with the dry Xeroform
dressing or for the Polysporin wet dressing compared with the
dry Xeroform dressing.
For the critical outcome of complications (hypergranulation tissue, postburn contracture, or hypertrophic scar),
we identified low-quality evidence (downgraded for risk of
bias, imprecision, and indirectness) from 1 RCT167 showing benefit for honey dressings compared with silver sulfadiazine–impregnated gauze dressings (RR, 0.13; 95% CI,
0.03–0.52).
For the important outcome of tissue healing, we identified low-quality evidence (downgraded for risk of bias,
imprecision, and indirectness) from 1 RCT167 showing benefit with honey (wet) compared with (dry) silver sulfadiazine–impregnated gauze dressing. This study enrolled 104
subjects and showed a decreased mean duration of time to
healing when a honey dressing was used (MD, −7.80; 95%
CI, −8.78 to −6.63). In addition, further low-quality evidence
(downgraded for risk of bias, imprecision, and indirectness) from 1 RCT168 enrolling 100 subjects also showed a
decreased mean duration of time to healing with honey (wet)
compared with (dry) potato peel dressings (MD, −5.80; 95%
CI, −6.68 to −4.92).
We did not identify any evidence to address the important outcome of pain and the less important outcomes of need
for advanced medical care, patient satisfaction, and rates of
fasciotomy.
Treatment Recommendations
No recommendation; there is insufficient evidence to show
any benefits of wet compared with dry dressings applied to
thermal burns in the prehospital setting.
Values, Preferences, and Task Force Insights
Studies included in this review evaluated out-of-hospital use
of dressings and assumed that cooling had taken place before
a dressing was applied. Public comment was made about the
use of plastic wrap for burns. Plastic wrap (a dry dressing) was
included in the search strategy, but no comparative studies to
a wet dressing were identified.
Knowledge Gaps
Further research is needed on the use of burn dressings in the
prehospital setting. Specifically, it is unknown what type of
dressing is optimal for use by first aid providers.
Dental Avulsion (FA 794)
Among adults and children with an avulsed permanent tooth
(P), does storage of the tooth in any solution prior to replantation (I), compared with storage in whole milk or the patient’s
saliva (C), change success of reimplantation, tooth survival
or viability, infection rate, pain, malfunction (eating, speech),
color of the tooth (O)?
Introduction
Immediate reimplantation of an avulsed tooth is thought by
the dental community to result in the greatest chance of tooth
survival. The First Aid Task Force believes that, in reality, few
first aid providers have the skills or willingness to attempt
this painful procedure, especially without protection from
exposure to blood or possible sharp bone spicules. Therefore,
if an avulsed tooth is not immediately reimplanted, the priority is to quickly transfer the patient and the avulsed tooth to
a healthcare professional capable of reimplanting the tooth.
Placing the avulsed tooth in a temporary storage solution
such as milk or saliva has been reported to extend the viability of the tooth before reimplantation. This PICO question
evaluates the effectiveness of alternative solutions to whole
milk or saliva.
Consensus on Science
We did not identify any evidence to address the important
outcomes of infection rate, pain, malfunction, and cosmetic
outcome.
Egg White (I) Compared With Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 2 randomized studies170,171
with 10 extracted teeth in each study, showing benefit in 1
study170 (MD, 91.80; 95% CI, 90.53–93.07 for cell viability after 1 hour of immersion; MD, 90.00; 95% CI, 87.87–
92.13 for cell viability after 2 hours of immersion) and not
showing any benefit in the other study171 (MD, −4.03; 95%
CI, −10.39 to 2.33 for cell viability after 1 hour of immersion; MD, 15.74; 95% CI, −9.76 to 41.24 after 3 hours of
immersion).
Ricetral (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
and imprecision) from 1 randomized study172 with 20 extracted
teeth, showing benefit (MD, 44.3; 95% CI, 12.82–75.78) for
cell viability after 45 minutes of immersion.
�Singletary et al
Coconut Water (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
and imprecision) from 1 randomized study173 with 30 extracted
teeth, showing benefit (MD, 339.4; 95% CI, 331.65–347.15)
for cell viability after 45 minutes of immersion.
Lactobacillus reuteri Solution (I) Compared With Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 observational study174 with 12
extracted teeth, but the MD for cell viability was not estimable
(median difference 116 000).
Saliva and Thereafter Hank’s Balanced Salt Solution (I)
Compared With Saliva and Thereafter Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 observational study175 with 10
extracted teeth. The study found a lower MD for cell viability
(MD 1% lower) after 30 minutes and a higher MD (MD, 2.4%
higher) after 60 minutes, but the CI was not estimable.
Saliva (I) Compared With Saliva and Thereafter Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 observational study175 with 10
extracted teeth. The study found a lower MD for cell viability
(MD, 8.4% lower after 30 minutes, 2% lower after 60 minutes), but the CI was not estimable.
Downloaded from http://ahajournals.org by on May 27, 2020
Eagle’s Medium (aMEM) (I) Compared With Saliva and
Thereafter Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 observational study175 with 10
extracted teeth. The study found a higher MD for cell viability
(MD, 5% higher after 30 minutes, 12.5% higher after 60 minutes), but the CI was not estimable.
EGCG (Epigallocatechin-3-Gallate) (I) Compared With Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 randomized study176 with 20
extracted teeth, showing no benefit (MD, 0.1; 95% CI, −0.09
to 0.28) for cell viability after 2 hours of immersion.
Tap Water (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
and imprecision) from 1 observational study,177 but the MD
for cell viability was not estimable (mean percentage of
45.17±12.03 SD for intervention group compared with the
mean percentage of 90.59±3.77 SD for control group).
Propolis 10% (I) Compared With Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 randomized study171 with 10
extracted teeth, showing benefit for cell viability after 1 hour
of immersion (MD, 14.73; 95% CI, 9.53–19.93), and for cell
viability after 3 hours of immersion (MD, 45.33; 95% CI,
21.73–68.93).
Part 9: First Aid
S301
Propolis 50% (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
and imprecision) from 2 randomized studies171,178 with 24 and
10 extracted teeth, showing benefit for cell viability after 45
minutes of immersion (MD, 1 192 290; 95% CI, 720 274.12–1
664 305.28), for cell viability after 1 hour of immersion (MD,
13.96; 95% CI, 4.9–23.02), and for cell viability after 3 hours
of immersion (MD, 29.36; 95% CI, 2.37–56.35).
Propolis 100% (I) Compared With Milk (C)
For the critical outcome of viability, we identified verylow-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 1 randomized study178
with 24 extracted teeth, showing benefit for cell viability
after 45 minutes of immersion (MD, 1 077 710; 95% CI,
266 920.68–1 888 499.32).
Phosphate Buffered Saline (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
and imprecision) from 1 randomized study179 with 10 extracted
teeth, showing no benefit for cell viability after 30 minutes
of dry time followed by a 15-minute immersion (MD, 8.31;
95% CI, −0.09 to 16.71), but showing benefit for cell viability
after both 60 minutes (MD, 8.76; 95% CI, 4.03–13.49) and
90 minutes of dry time (MD, −5.17; 95% CI, −9.93 to −0.41)
followed by a 15-minute immersion.
Saline (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
and imprecision) from 1 randomized study with 24 extracted
teeth178 showing no benefit for cell viability after 45 minutes of immersion (MD, −143 540; 95% CI, −210 604.01 to
−76 475.99). We identified very-low-quality evidence (downgraded for indirectness and imprecision) from 1 observational
study180 with 24 teeth in which benefit for cell viability was
not shown after 2 hours of immersion (MD, −161 000; 95%
CI, −362 186.91 to 40 186.91). We identified very-low-quality
evidence (downgraded for indirectness and imprecision) from
2 other observational studies174,177 in which the MD for cell
viability was not estimable (median difference 376 000; mean
percentage of 77.8±2.92 SD for intervention group versus
mean percentage of 90.59±3.77 SD for control group).
For the critical outcome of viability (periodontal healing), we identified very-low-quality evidence (downgraded
for risk of bias and imprecision) from 1 observational study181
with 25 avulsed teeth showing no benefit (RR, 0.99; 95% CI,
0.48–2.04).
For the critical outcome of success of reimplantation
(replacement resorption and extraction due to replacement
resorption), we identified very-low-quality evidence (downgraded for risk of bias and imprecision) from 1 observational study181 with 25 avulsed teeth showing no benefit (RR,
1.07; 95% CI, 0.33–3.46; and RR, 0.89; 95% CI, 0.09–8.50,
respectively).
Hank’s Balanced Salt Solution (I) Compared With Milk (C)
For the critical outcome of viability, we identified very-lowquality evidence (downgraded for risk of bias, indirectness,
�S302
Circulation
October 20, 2015
and imprecision) from 4 randomized studies170–173 including
10 to 30 extracted teeth, showing benefit for cell viability
after 45 minutes of immersion (MD, 261.13; 95% CI, 249.7–
272.56),173 for cell viability after 45 minutes of immersion
(MD, 64.2; 95% CI, 32.59–95.81),172 for cell viability after
1 hour of immersion (MD, 93.4; 95% CI, 91.81–94.99),170
for cell viability after 2 hours of immersion (MD, 89.8; 95%
CI, 87.95–91.65),170 and for cell viability after 3 hours of
immersion (MD, 25.59; 95% CI, 1.13–50.05).171 We identified
very-low-quality evidence (downgraded for risk of bias, indirectness, and imprecision) from 3 studies171,176,178 that did not
show benefit for cell viability after 45 minutes of immersion
(MD, 22 090; 95% CI, −64 812.53 to 108 992.53178; MD, 0.85;
95% CI, −9.31 to 7.61171; MD, 0.05; 95% CI, −0.16 to 0.25176).
We identified very-low-quality evidence (downgraded for
indirectness and imprecision) from 1 study, from which the
MD for cell viability was not estimable (mean percentage of
87.04±5.7 SD for intervention group versus mean percentage
of 90.59±3.77 SD for control group).177
Another’s Saliva (I) Compared With Storage in the Patient’s
Mouth (C)
For the critical outcome of viability (pulpal healing), we identified very-low-quality evidence (downgraded for risk of bias
and imprecision) from 1 observational study182 with 10 avulsed
teeth, showing no benefit (RR, 1; 95% CI, 0.08–11.93).
Downloaded from http://ahajournals.org by on May 27, 2020
Saline (I) Compared With Saliva (C)
For the critical outcome of viability (pulpal and periodontal
ligament healing), we identified very-low-quality evidence
(downgraded for risk of bias and imprecision) from 2 observational studies182,183 with 24 and 66 avulsed teeth, showing
no benefit (RR, 0.6; 95% CI, 0.18–1.97 for pulpal healing
and RR, 0.67; 95% CI, 0.21–2.15 for periodontal ligament
healing).
Storage in Another Person’s Mouth (I) Compared With
Storage in the Patient’s Mouth (C)
For the critical outcome of viability (periodontal ligament
healing), we identified very-low-quality evidence (downgraded for risk of bias and imprecision) from 1 observational
study183 with 18 avulsed teeth, showing no benefit (RR, 1;
95% CI, 0.27–3.96).
Dentosafe Box Compared With Milk
For the critical outcome of viability (periodontal healing),
we identified very-low-quality evidence (downgraded for
risk of bias and imprecision) from 1 observational study181
with 24 avulsed teeth showing no benefit (RR, 1.33; 95% CI,
0.74–2.40).
For the critical outcome of success of replantation
(replacement resorption and extraction due to replacement
resorption), we identified very-low-quality evidence (downgraded for risk of bias and imprecision) from 1 observational study181 with 24 avulsed teeth showing no benefit (RR,
0.40; 95% CI, 0.06–2.87 and RR, 1.00; 95% CI, 0.11–9.44,
respectively).
Treatment Recommendations
We suggest the use of Hank’s Balanced Salt Solution, propolis, egg white, coconut water, or ricetral in comparison with
Table 4. Composition of Temporary Storage Solutions for
Avulsed Tooth, in Order of Preference*
Temporary Storage Solution
Composition
Hank’s Balanced Salt Solution
Group of salts rich in bicarbonate ions:
0.14 g/L CaCl2, 0.40 g/L KCl, 0.06 g/L KH2PO4,
0.10 g/L MgCl2-6H20, 0.10 g/L MgSO4-7H2O,
8.00 g/L NaCl, 0.35 g/L NaHCO3, 0.048 g/L
Na2HPO4, 1.00 g/L glucose, 0.01 g/L
phenol red
Propolis
Resinous mixture that honey bees collect
from tree buds, sap flows, or other botanical
sources
Egg white
Coconut water
Clear liquid from young green coconuts
Ricetral
Sodium chloride, sodium citrate, potassium
chloride, extruded rice
Whole milk
Saline
Sodium chloride: 9.0 g/L NaCl; home-made
saline: dissolving approximately half a
teaspoon of table salt into 240 mL of clean
tap water
Phosphate-buffered saline
Water-based salt solution containing sodium
phosphate, sodium chloride: 8.0 g/L NaCl, 0.2
g/L KCl, 1.44 g/L Na2HPO4, 0.24 g/L KH2PO4
*Based on the evidence alone, it was not possible to decide which solution
will result in the longest tooth survival. The order of preference proposed in this
table is based on the evidence evaluated, availability, and feasibility.
whole milk as a temporary storage solution for an avulsed
tooth that cannot be immediately reimplanted (weak recommendation, very-low-quality evidence). The solutions used
and the order of priority for tooth storage are listed in Table 4.
We suggest the use of whole milk in comparison with
saline as a temporary storage solution for an avulsed tooth if
none of the above solutions are available (weak recommendation, very-low-quality evidence).
There is insufficient evidence for or against temporary
storage of an avulsed tooth in saliva compared with alternative
solutions.
Values, Preferences, and Task Force Insights
In making this recommendation, we recognize that survival
of an avulsed tooth requires that it must be reimplanted as
soon as possible, but this procedure may not be possible in
the first aid setting. The use of a suitable temporary storage
solution for an avulsed tooth should not delay efforts at reimplantation, but it may aid in the survival of the tooth before
reimplantation.
No treatment recommendation was formulated regarding the use of phosphate-buffered saline (PBS) as a storage
solution, as in the PBS study there was a dry time from 60 to
90 minutes, which is not representative of a typical situation.
However, this could be relevant for settings where it is not
possible to immediately store the tooth in a storage solution.
Knowledge Gaps
• There
is a lack of observational studies with avulsed
teeth (instead of extracted teeth), measuring tooth viability (not cell viability), and success of replantation.
�Singletary et al
• In a future PICO question, reimplanting the tooth in the
mouth (in dental socket) versus storage in a temporary
storage medium could be compared.
• Is training in dental reimplantation for first aid providers
feasible and effective?
Education
Education in first aid continues to be a topic with few scientific studies. In the 2010 review of educational topics, no
evidence was found to support or recommend any method of
evaluating or monitoring a first aid trainee’s educational progress or the specific frequency of retraining to retain skills and
knowledge.10 The task force decided to investigate the basic
question, “Is there documented evidence of benefit in terms of
patient outcomes as a result of first aid training?”
Many questions remain, and research is desperately
needed, particularly in the realm of teaching techniques for
first aid and methods to evaluate the retention of skills.
First Aid Training (FA 773)
Among adults and children receiving first aid (P), does care
from a trained first aid provider (I), compared with care from
an untrained person (C), change survival rates, recognition
of acute injury or illness, prevent further illness or injury (ie,
harm), time to resolution of injury, the likelihood of harm (eg,
infection), time to resolution of symptoms (O)?
Downloaded from http://ahajournals.org by on May 27, 2020
Introduction
In the ILCOR 2015 review process, first aid is defined as the
helping behaviors and initial care provided for an acute illness or injury. Training is, therefore, an essential core element
of the practice of first aid. The task force thought that it was
important to verify the impact of both formal and informal
first aid training of individuals and communities.
Consensus on Science
For the critical outcome of increased survival rates from
trauma, we identified low-quality evidence (downgraded for
risk of bias) from 1 observational study184 enrolling 1341
patients showing a reduced mortality rate among patients initially managed by trained first aid providers of 9.8% (32/325)
compared with 15.6% (158/101) for patients without trained
first aid support (OR, 0.59; 95% CI, 0.40–0.89).
For the important outcome of time to resolution of
symptoms, we identified very-low-quality evidence (downgraded for indirectness and imprecision) from 1 observational
study174 with 125 subjects with burns of less than 20% total
body surface area showing benefit from first aid training, with
88.5% of patients who received first aid treatment of cooling
the burn with water requiring hospitalization of less than 10
days, compared with only 67.2% who received no treatment
requiring less than 10 days’ hospitalization (RR, 0.35; 95%
CI, 0.16–0.76).
For the important outcome of preventing further injury,
we identified very-low-quality evidence (downgraded for
indirectness and imprecision) from 1 observational study175
with 244 patients (121 precampaign, 123 postcampaign) with
acute burn injury treated either before or after a burn first aid
treatment public education campaign, showing benefit with
Part 9: First Aid
S303
burn first aid treatment by reduction of the percent of those
burned requiring inpatient wound care or surgery from 64.2%
(78/121) precampaign compared with 35.6% (44/123) postcampaign (OR, 0.307; 95% CI, 0.18–0.52).
Furthermore, we identified very-low-quality evidence
(downgraded for risk of bias and imprecision) from 1 observational study185 with 39 subjects without formal/advanced
medical training who performed reduction of shoulder dislocations in a wilderness environment. This study found no
statistically significant difference in the rate of successful
reduction by laypersons without first aid training (17/24,
70.8%) compared with the successful reduction rate when
individuals with either wilderness first aid or first responder
training were present or performed the reduction (11/15, 73%;
OR, 0.88; 95% CI, 0.21–3.74).
For the critical outcome of recognition of acute injury or
illness, and the important outcome of the likelihood of harm,
there were no studies identified.
Treatment Recommendations
We suggest that education and training in first aid is undertaken to improve morbidity and mortality from injury and illness (weak recommendation, low-quality evidence).
Values, Preferences, and Task Force Insights
Positive outcomes were identified in both public health campaigns for specific injuries and course-based training for
general trauma. Although no other formal PICO questions
related to first aid education were evaluated, the review of
stroke assessment systems (above) incidentally discovered
that training of lay providers in a stroke assessment system
led to improved ability to identify the signs of a stroke when
assessed immediately after training (94.4% in those trained
versus 76.4% in untrained lay providers), and that 96.9%
of the trained lay providers were able to identify signs of
stroke when assessed 3 months after training.69 This study
supports the recommendation in this review, and specifically shows that public health campaigns aimed at first aid
for specific illnesses and injuries, as well as course-based
first aid training, can positively impact outcomes of morbidity and mortality.
Knowledge Gaps
Individual domains of first aid (eg, recognizing an emergency,
calling for additional help, specific skills such as direct pressure) have not been studied as to what contributes to a victim’s
health outcomes. Future reviews comparing first aid education modalities and context of first aid settings may contribute
to developing training guidelines. Additionally, the period of
time between a first aid provider’s initial training and refreshing those first aid skills to maintain competency needs to be
identified. Along with patient outcomes, public health outcomes and cost-analysis of training versus no training may
help prioritize resources. These questions and opportunities
for research can also be valuable as new modalities emerge for
learning (eg, social media or just-in-time).
Acknowledgments
We acknowledge the helpfulness of the insightful comments received
during the public comment period. We thank the following individuals (the First Aid Chapter Collaborators) for their collaborations on
�S304
Circulation
October 20, 2015
the systematic reviews contained in this section: L. Kristian Arnold,
Richard N. Bradley, Barbara C. Caracci, Jestin N. Carlson, Pascal
Cassan, Athanasios F. Chalkias, Nathan P. Charlton, Justin M.
DeVoge, Tessa A. Y. Dieltjens, Thomas R. Evans, Jeffrey D. Ferguson,
Ryan C. Fringer, Christina M. Hafner, Kyee H. Han, Anthony J.
Handley, Bryan B. Kitch, Danita N. Koehler, Amy Kule, Andrew I.
MacPherson, Daniel Meyran, Michael A. Nemeth, Catherine Patocka,
Nele S. Pauwels, Michael J. Reilly, Richard C. Rusk, Susanne
Schunder-Tatzber, Samuel R. Seitz, Ralph M. Shenefelt, Chih-Hung
Wang, and Jae-Hyug Woo.
The authors acknowledge the outstanding assistance of Emmy
DeBuck in the production of numerous GRADE Summary of
Evidence tables for the 2015 First Aid science reviews.
The authors also acknowledge the contributions of Jorge Neira,
MD, of the InterAmerican Heart Foundation, to the early work of the
ILCOR First Aid Task Force.
Disclosures
2015 CoSTR Part 9: First Aid: Writing Group Disclosures
Speakers’
Bureau/
Honoraria
Expert
Witness
Ownership
Interest
Consultant/
Advisory Board
Other
American Red
Cross*
None
None
None
None
None
None
None
None
None
None
None
None
University of
Calgary
None
None
None
None
None
None
None
Wei-Tien Chang
National Taiwan
University Hospital
Research grants
from government
and university
hospital*
None
None
None
Patent for
Leverage-assisted
ACD CPR device*
None
None
Emmy D. J. De
Buck
Belgian Red
Cross-Flanders
None
None
None
None
None
None
Belgian Red
Cross-Flanders*
Writing Group
Member
Employment
Research Grant
Eunice M.
Singletary
University of
Virginia
None
David A. Zideman
Imperial College
Healthcare NHS
Trust
Ian E. Blanchard
Other Research
Support
Downloaded from http://ahajournals.org by on May 27, 2020
Rita A. Herrington
Indiana University
None
None
None
None
None
None
None
Natalie A. Hood
Monash Medical
Centre
None
None
None
None
None
None
None
Jan L. Jensen
Emergency
Health Services,
Dalhousie
University
None
None
None
None
None
None
Emergency Health
Services*
Luis F.
Lojero-Wheatley
Swiss Hospital
None
None
None
None
None
None
None
David S.
Markenson
Sky Ridge Medical
Center
None
American Red
Cross*
None
None
None
None
None
Jeffrey L.
Pellegrino
Kent State
University
None
None
None
None
None
None
None
Janel M. Swain
Emergency Health
Services
None
None
None
None
None
None
None
Hyuk Jun Yang
Gachon University
None
None
None
None
None
None
None
Tualatin Valley
Fire & Rescue
None
None
None
None
None
American Heart
Association†
None
Consultant
Jeff A. Woodin
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the
Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (a) the person
receives $10 000 or more during any 12-month period, or 5% or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of
the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding
definition.
*Modest.
†Significant.
�Singletary et al
Part 9: First Aid
S305
Appendix
CoSTR Part 9: PICO Appendix
Part
Downloaded from http://ahajournals.org by on May 27, 2020
Task Force
PICO ID
Short Title
PICO Question
Evidence Reviewers
Part 9
First Aid
FA 500
Second Dose of
Epinephrine for Anaphylaxis
Among adults and children experiencing severe anaphylaxis
requiring the use of epinephrine (P), does administration of a
second dose of epinephrine (I), compared with administration
of only 1 dose (C), change resolution of symptoms, adverse
effects, complications (O)?
Athanasios Chalkias,
Barbara Caracci,
Emmy De Buck
Part 9
First Aid
FA 503
Straightening of an
Angulated Fracture
Among adults and children who receive first aid for an
angulated long bone fracture (P), does realignment of the
fracture prior to splinting (I), compared with splinting as found
(C), change neurologic injury, vascular injury, splinting, pain,
time to medical transportation (O)?
Ryan Fringer,
Catherine Patocka
Part 9
First Aid
FA 517
Recovery Position
Among adults who are breathing and unresponsive outside
of a hospital (P), does positioning in a lateral, side-lying,
recovery position (I), compared with supine position (C),
change overall mortality, need for airway management, the
incidence of aspiration, the likelihood of cervical spinal injury,
complications, incidence of cardiac arrest (O)?
Janel Swain, S Seitz
Part 9
First Aid
FA 519
Oxygen Administration for
First Aid
Among adults and children who exhibit symptoms or signs
of shortness of breath, difficulty breathing, or hypoxemia
outside of a hospital (P), does administration of supplementary
oxygen (I), compared with no administration of oxygen (C),
change survival with favorable neurologic/functional outcome
at discharge, 30 days, 60 days, 180 days, and/or 1 year;
survival only at discharge, 30 days, 60 days, 180 days, and/or
1 year; shortness of breath; time to resolution of symptoms; or
therapeutic endpoints (eg, oxygenation and ventilation) (O)?
Michael Nemeth,
Chih-Hung Wang
Part 9
First Aid
FA 520
Optimal Position for Shock
Among adults and children who receive first aid for shock
(P), does positioning of the patient (I), compared with
not positioning the patient (C), change overall mortality,
complications, incidence of cardiac arrest, vital signs, hospital
length of stay (O)?
Anthony Handley,
Luis Lojero-Wheatley,
Justin DeVoge
Part 9
First Aid
FA 525
First Aid Treatment for an
Open Chest Wound
Among adults and children who are being treated for an
open chest wound outside of a hospital (P), does occlusive
bandage application or occlusive device (I), compared with
a nonocclusive dressing (C), change or improve survival,
respiratory arrest, oxygen saturation, vital signs, the rate of
cardiac and respiratory arrests, improve therapeutic endpoints
(oxygenation and ventilation) (O)?
Wei-tien Chang, Kyee Han
Part 9
First Aid
FA 530
Control of Bleeding
Among adults and children with bleeding (P), does application
of localized cold therapy, elevation of extremity, and/or
application of pressure over proximal pressure points (I),
compared with direct pressure alone (C), change overall
mortality, hemostasis, major bleeding, complications, hospital
length of stay (O)?
Richard Bradley,
Jae-Hyug Woo
Part 9
First Aid
FA 534
Bronchodilator Use for
Asthma with Difficulty
Breathing
Among adults and children in the prehospital setting who
have asthma and are experiencing difficulty in breathing (P),
does bronchodilator administration (I), compared with no
bronchodilator administration (C), change time to resolution of
symptoms, time to resumption of usual activity, complications,
harm to patient, therapeutic endpoints (eg, oxygenation and
ventilation), need for advanced medical care (O)?
Andrew MacPherson,
Nathan Charlton,
Ian Blanchard
Part 9
First Aid
FA 540
Eye Chemical Injury:
Irrigation
Among adults and children who have a chemical or other
unknown substance enter the conjunctival sac (P), does
irrigation with isotonic saline, balanced salt solution, or other
commercial eye irrigation solutions (I), compared with irrigation
with water (C), change tissue healing, functional recovery,
pain, complications, time to resumption of usual activity,
restoration to the preexposure condition, time to resolution of
symptoms (O)?
Ralph Shenefelt,
L. Kristian Arnold,
Janel Swain
(Continued )
�S306
Circulation
October 20, 2015
CoSTR Part 9: PICO Appendix, Continued
Part
Downloaded from http://ahajournals.org by on May 27, 2020
Task Force
PICO ID
Short Title
PICO Question
Evidence Reviewers
Part 9
First Aid
FA 584
Exertional Dehydration and
Oral Rehydration
Among adults and children with exertion-related dehydration
(P), does drinking oral carbohydrate-electrolyte (CE) liquids (I),
compared with drinking water (C), change volume/hydration
status, vital signs, development of hyperthermia, development
of hyponatremia, need for advanced medical care, blood
glucose, patient satisfaction (O)?
Rita Herrington, Amy Kule,
Jestin Carlson
Part 9
First Aid
FA 586
Aspirin for Chest Pain (Early
vs. Late)
Among adults who are experiencing chest pain outside of a
hospital (P), does early administration of aspirin (I), compared
with later administration of aspirin (C), change cardiovascular
mortality, complications, incidence of cardiac arrest, cardiac
functional outcome, infarct size, hospital length of stay, chest
pain resolution (O)?
Janel Swain,
Thomas Evans
Part 9
First Aid
FA 768
Use of a Tourniquet
Among adults and children with severe external limb bleeding
(P), does the application of a tourniquet (I), compared with not
applying a tourniquet (C), change hemostasis, overall mortality,
vital signs, functional limb recovery, complications, blood loss,
incidence of cardiac arrest (O)?
Jan Jensen, Michael Reilly
Part 9
First Aid
FA 769
Hemostatic Dressings
In patients with severe external bleeding (P), does the
application of topical hemostatic dressings plus standard first
aid (I), compared with standard first aid alone (C), change
overall mortality, vital signs, hemostasis, complications, blood
loss, major bleeding, incidence of cardiac arrest (O)?
Jan Jensen,
Richard Bradley
Part 9
First Aid
FA 770
Cooling of Burns
Among adults and children with thermal injuries (P), does
active cooling of burns (I), compared with passive cooling (C),
change pain, complications, wound healing, need for advanced
medical care, patient satisfaction, rates of fasciotomy, depth or
breadth of burn (O)?
Natalie Hood,
Nathan Charlton
Part 9
First Aid
FA 771
Wet Compared With Dry
Burn Dressings
Among adults and children with thermal injuries (P), does
the use of a wet dressing (I), compared with dry dressing (C),
change complications, pain, tissue healing, need for advanced
medical care, patient satisfaction, rates of fasciotomy (O)?
Emmy De Buck,
Ian Blanchard
Part 9
First Aid
FA 772
Cervical Spinal Motion
Restriction
Among adults and children with suspected blunt traumatic
cervical spinal injury (P), does cervical spinal motion restriction
(I), compared with no cervical spinal motion restriction (C),
change neurologic injury, complications, overall mortality,
pain, patient comfort, movement of the spine, hospital length
of stay (O)?
Tessa Dieltjens,
Jeff Woodin
Part 9
First Aid
FA 773
First Aid Training
Among adults and children receiving first aid (P), does care
from a trained first aid provider (I), compared with care from
an untrained person (C), change increase survival rates,
recognition of acute injury or illness, prevent further illness or
injury (ie, harm), time to resolution of injury, the likelihood of
harm (eg, infection), time to resolution of symptoms (O)?
Jeffrey Pellegrino,
Danita Koehler
Part 9
First Aid
FA 794
Dental Avulsion
Among adults and children with an avulsed permanent
tooth (P), does storage of the tooth in any solution prior to
replantation (I), compared with storage in whole milk or the
patient’s saliva (C), change success of reimplantation, tooth
survival or viability, infection rate, pain, malfunction (eating,
speech), color of the tooth (O)?
Nele Pauwels, Bryan Kitch
Part 9
First Aid
FA 795
Hypoglycemia Treatment
Among adults and children with symptomatic hypoglycemia
(P), does administration of dietary forms of sugar (I), compared
with standard dose (15–20 g) of glucose tablets (C), change
time to resolution of symptoms, risk of complications (eg,
aspiration), blood glucose, hypoglycemia, hospital length of
stay (O)?
Jestin Carlson,
Susanne Schunder-Tatzber
(Continued )
�Singletary et al
Part 9: First Aid
S307
CoSTR Part 9: PICO Appendix, Continued
Part
Task Force
PICO ID
Part 9
First Aid
FA 799
Part 9
First Aid
Part 9
First Aid
Short Title
PICO Question
Evidence Reviewers
Concussion
Among adults and children with suspected head injury
without loss of consciousness (P), does use of a simple
concussion scoring system (I), compared with standard first
aid assessment without a scoring system (C), change time to
recognition of the deteriorating patient, the likelihood of a poor
neurologic outcome, survival to 30 days with good neurologic
outcome, need for advanced medical care, time to medical
transportation, or likelihood of differentiating between minor
head contusion and more serious concussion (O)?
Richard Rusk,
Christina Gruber
FA 801
Stroke Recognition
Among adults with suspected acute stroke (P), does the use
of a rapid stroke scoring system or scale (I), compared with
standard first aid assessment (C), change time to treatment
(eg, door to drug), recognition of acute injury or illness,
discharge with favorable neurologic status, survival with
favorable neurologic outcome, or increased public/layperson
recognition of stroke signs (O)?
Pascal Cassan,
Jeffrey Ferguson,
Daniel Meyran
FA 871
Aspirin for Chest Pain:
Administration
Among adults experiencing chest pain due to suspected MI (P),
does administration of aspirin (I), compared with no administration
of aspirin (C), change cardiovascular mortality, complications,
adverse effects, incidence of cardiac arrest, cardiac functional
outcome, infarct size, hospital length of stay (O)?
References
Downloaded from http://ahajournals.org by on May 27, 2020
1. Institute of Medicine. Standards for Systematic Reviews. http://www.iom.
edu/Reports/2011/Finding-What-Works-in-Health-Care-Standards-forSystematic-Reviews/Standards.aspx. Accessed May 6, 2015.
2. Schünemann H, Brożek J, Guyatt G, Oxman A. GRADE Handbook.
2013. http://www.guidelinedevelopment.org/handbook/. Accessed May
6, 2015.
3. O’Connor D, Green S, Higgins JPT, eds. Chapter 5: Defining the review
questions and developing criteria for including studies. In: The Cochrane
Collaboration. Higgins JPT, Green, S, eds. Cochrane Handbook for
Systematic Reviews of Interventions. Version 5.1.0. 2011. http://handbook.
cochrane.org/. Accessed May 6, 2015.
4. Higgins JPT, Altman DG, Sterne J, eds. Chapter 8.5: The Cochrane
Collaboration’s tool for assessing risk of bias. In: The Cochrane
Collaboration. Higgins JPT, Green, S, eds. Cochrane Handbook for
Systematic Reviews of Interventions. Version 5.1.0. 2011. http://handbook.
cochrane.org/. Accessed May 6, 2015.
5. Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma
JB, Leeflang MM, Sterne JA, Bossuyt PM; QUADAS-2 Group.
QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–536. doi:
10.7326/0003-4819-155-8-201110180-00009.
6. Schünemann H, Brożek J, Guyatt G, Oxman A. 5.2.1 Study limitations
(risk of bias). In: GRADE Handbook 2013. http://www.guidelinedevelopment.org/handbook/#h.m9385o5z3li7. Accessed May 6, 2015.
7. Evidence Prime Inc. GRADEpro Guideline Development Tool. http://
www.guidelinedevelopment.org/. Accessed May 6, 2015.
8. Schünemann H, Brożek J, Guyatt G, Oxman A. 5. Quality of evidence.
In: GRADE Handbook. 2013. http://www.guidelinedevelopment.org/
handbook/#h.9rdbelsnu4iy. Accessed May 6, 2015.
9. Schünemann H, Brożek J, Guyatt G, Oxman A. 5.1 Factors determining
the quality of evidence. In: GRADE Handbook. 2013. http://www.guidelinedevelopment.org/handbook/#h.9rdbelsnu4iy. Accessed May 6, 2015.
10. Markenson D, Ferguson JD, Chameides L, Cassan P, Chung KL, Epstein
JL, Gonzales L, Hazinski MF, Herrington RA, Pellegrino JL, Ratcliff N,
Singer AJ; First Aid Chapter Collaborators. Part 13: first aid: 2010 American
Heart Association and American Red Cross International Consensus
on First Aid Science With Treatment Recommendations. Circulation.
2010;122(Suppl 2):S582–S605. doi: 10.1161/CIRCULATIONAHA.
110.971168.
11. Adnet F, Borron SW, Finot MA, Minadeo J, Baud FJ. Relation of body
position at the time of discovery with suspected aspiration pneumonia in
poisoned comatose patients. Crit Care Med. 1999;27:745–748.
Thomas Evans,
Janel Swain
12. Litman RS, Wake N, Chan LM, McDonough JM, Sin S, Mahboubi S,
Arens R. Effect of lateral positioning on upper airway size and morphology in sedated children. Anesthesiology. 2005;103:484–488.
13. Arai YC, Fukunaga K, Hirota S, Fujimoto S. The effects of chin lift and
jaw thrust while in the lateral position on stridor score in anesthetized children with adenotonsillar hypertrophy. Anesth Analg. 2004;99:1638–41,
table of contents. doi: 10.1213/01.ANE.0000135637.95853.1C.
14. Gunn BD, Eizenberg N, Silberstein M, McMeeken JM, Tully EA,
Stillman BC, Brown DJ, Gutteridge GA. How should an unconscious person with a suspected neck injury be positioned? Prehosp Disaster Med.
1995;10:239–244.
15. Del Rossi G, Dubose D, Scott N, Conrad BP, Hyldmo PK, Rechtine
GR, Horodsyki M. Motion produced in the unstable cervical spine
by the HAINES and lateral recovery positions. Prehosp Emerg Care.
2014;18:539–543. doi: 10.3109/10903127.2014.916019.
16. Fulstow R, Smith GB. The new recovery position, a cautionary tale.
Resuscitation. 1993;26:89–91.
17. Doxey J. Comparing 1997 Resuscitation Council (UK) recovery position
with recovery position of 1992 European Resuscitation Council guidelines: a user’s perspective. Resuscitation. 1998;39:161–169.
18. Rathgeber J, Panzer W, Günther U, Scholz M, Hoeft A, Bahr J, Kettler D.
Influence of different types of recovery positions on perfusion indices of
the forearm. Resuscitation. 1996;32:13–17.
19. Kyriakides ZS, Koukoulas A, Paraskevaidis IA, Chrysos D, Tsiapras D,
Galiotos C, Kremastinos DT. Does passive leg raising increase cardiac
performance? A study using Doppler echocardiography. Int J Cardiol.
1994;44:288–293.
20. Wong DH, O’Connor D, Tremper KK, Zaccari J, Thompson P, Hill D.
Changes in cardiac output after acute blood loss and position change in
man. Crit Care Med. 1989;17:979–983.
21. Gaffney FA, Bastian BC, Thal ER, Atkins JM, Blomqvist CG. Passive leg
raising does not produce a significant or sustained autotransfusion effect.
J Trauma. 1982;22:190–193.
22. Kamran H, Salciccioli L, Kumar P, Pushilin S, Namana V, Trotman S,
Lazar J. The relation between blood pressure changes induced by passive
leg raising and arterial stiffness. J Am Soc Hypertens. 2010;4:284–289.
doi: 10.1016/j.jash.2010.09.002.
23. Jabot J, Teboul JL, Richard C, Monnet X. Passive leg raising for predicting
fluid responsiveness: importance of the postural change. Intensive Care
Med. 2009;35:85–90. doi: 10.1007/s00134-008-1293-3.
24. Boulain T, Achard JM, Teboul JL, Richard C, Perrotin D, Ginies G.
Changes in BP induced by passive leg raising predict response to fluid
loading in critically ill patients. Chest. 2002;121:1245–1252.
�S308
Circulation
October 20, 2015
Downloaded from http://ahajournals.org by on May 27, 2020
25. Wijesinghe M, Perrin K, Healy B, Hart K, Clay J, Weatherall M, Beasley
R. Pre-hospital oxygen therapy in acute exacerbations of chronic
obstructive pulmonary disease. Intern Med J. 2011;41:618–622. doi:
10.1111/j.1445-5994.2010.02207.x.
26. Bruera E, de Stoutz N, Velasco-Leiva A, Schoeller T, Hanson J. Effects
of oxygen on dyspnoea in hypoxaemic terminal-cancer patients. Lancet.
1993;342:13–14.
27. Uronis HE, Currow DC, McCrory DC, Samsa GP, Abernethy AP. Oxygen
for relief of dyspnoea in mildly- or non-hypoxaemic patients with cancer:
a systematic review and meta-analysis. Br J Cancer. 2008;98:294–299.
doi: 10.1038/sj.bjc.6604161.
28. Philip J, Gold M, Milner A, Di Iulio J, Miller B, Spruyt O. A randomized,
double-blind, crossover trial of the effect of oxygen on dyspnea in patients
with advanced cancer. J Pain Symptom Manage. 2006;32:541–550. doi:
10.1016/j.jpainsymman.2006.06.009.
29. Booth S, Kelly MJ, Cox NP, Adams L, Guz A. Does oxygen help dyspnea
in patients with cancer? Am J Respir Crit Care Med. 1996;153:1515–
1518. doi: 10.1164/ajrccm.153.5.8630595.
30. Ahmedzai SH, Laude E, Robertson A, Troy G, Vora V. A double-blind,
randomised, controlled Phase II trial of Heliox28 gas mixture in lung cancer patients with dyspnoea on exertion. Br J Cancer. 2004;90:366–371.
doi: 10.1038/sj.bjc.6601527.
31. Longphre JM, Denoble PJ, Moon RE, Vann RD, Freiberger JJ. First
aid normobaric oxygen for the treatment of recreational diving injuries.
Undersea Hyperb Med. 2007;34:43–49.
32. 2005 International Consensus on Cardiopulmonary Resuscitation and
Emergency Cardiovascular Care Science with Treatment Recommendations,
Section 2 part 10: first aid. Circulation. 2005;112:III115–III125.
33. Bentur L, Canny GJ, Shields MD, Kerem E, Schuh S, Reisman JJ,
Fakhoury K, Pedder L, Levison H. Controlled trial of nebulized albuterol
in children younger than 2 years of age with acute asthma. Pediatrics.
1992;89:133–137.
34. van der Woude HJ, Postma DS, Politiek MJ, Winter TH, Aalbers R. Relief
of dyspnoea by beta2-agonists after methacholine-induced bronchoconstriction. Respir Med. 2004;98:816–820.
35. Littner MR, Tashkin DP, Siegel SC, Katz R. Double-blind comparison of
acute effects of inhaled albuterol, isoproterenol and placebo on cardiopulmonary function and gas exchange in asthmatic children. Ann Allergy.
1983;50:309–316.
36. Karpel JP, Aldrich TK, Prezant DJ, Guguchev K, Gaitan-Salas A, Pathiparti
R. Emergency treatment of acute asthma with albuterol metered-dose
inhaler plus holding chamber: how often should treatments be administered? Chest. 1997;112:348–356.
37. Berger WE, Milgrom H, Skoner DP, Tripp K, Parsey MV, Baumgartner
RA; Xopenex Pediatric Asthma Group. Evaluation of levalbuterol metered
dose inhaler in pediatric patients with asthma: a double-blind, randomized,
placebo- and active-controlled trial. Curr Med Res Opin. 2006;22:1217–
1226. doi: 10.1185/030079906X112534.
38. Politiek MJ, Boorsma M, Aalbers R. Comparison of formoterol, salbutamol and salmeterol in methacholine-induced severe bronchoconstriction.
Eur Respir J. 1999;13:988–992.
39. Hermansen MN, Nielsen KG, Buchvald F, Jespersen JJ, Bengtsson
T, Bisgaard H. Acute relief of exercise-induced bronchoconstriction by inhaled formoterol in children with persistent asthma. Chest.
2006;129:1203–1209. doi: 10.1378/chest.129.5.1203.
40. Amirav I, Yacobov R, Luder AS. Formoterol turbuhaler is as effective as
salbutamol diskus in relieving adenosine-induced bronchoconstriction in
children. J Aerosol Med. 2007;20:1–6. doi: 10.1089/jam.2006.0561.
41. Emerman CL, Shade B, Kubincanek J. A controlled trial of nebulized isoetharine in the prehospital treatment of acute asthma. Am J Emerg Med.
1990;8:512–514.
42. Weiss SJ, Anand P, Ernst AA, Orgeron D, May WL. Effect of out-of-hospital albuterol inhalation treatments on patient comfort and morbidity. Ann
Emerg Med. 1994;24:873–878.
43. Osmond MH, Klassen TP. Efficacy of ipratropium bromide in acute childhood asthma: a meta-analysis. Acad Emerg Med. 1995;2:651–656.
44. Harbison J, Hossain O, Jenkinson D, Davis J, Louw SJ, Ford GA.
Diagnostic accuracy of stroke referrals from primary care, emergency
room physicians, and ambulance staff using the face arm speech test.
Stroke. 2003;34:71–76.
45. Iguchi Y, Kimura K, Watanabe M, Shibazaki K, Aoki J. Utility of the
Kurashiki Prehospital Stroke Scale for hyperacute stroke. Cerebrovasc
Dis. 2011;31:51–56. doi: 10.1159/000320854.
46. Chenkin J, Gladstone DJ, Verbeek PR, Lindsay P, Fang J, Black SE,
Morrison L. Predictive value of the Ontario prehospital stroke screening
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
tool for the identification of patients with acute stroke. Prehosp Emerg
Care. 2009;13:153–159. doi: 10.1080/10903120802706146.
Wojner-Alexandrov AW, Alexandrov AV, Rodriguez D, Persse D,
Grotta JC. Houston paramedic and emergency stroke treatment and outcomes study (HoPSTO). Stroke. 2005;36:1512–1518. doi: 10.1161/01.
STR.0000170700.45340.39.
Frendl DM, Strauss DG, Underhill BK, Goldstein LB. Lack of impact of
paramedic training and use of the cincinnati prehospital stroke scale on
stroke patient identification and on-scene time. Stroke. 2009;40:754–756.
doi: 10.1161/STROKEAHA.108.531285.
O’Brien W, Crimmins D, Donaldson W, Risti R, Clarke TA, Whyte S,
Sturm J. FASTER (Face, Arm, Speech, Time, Emergency Response):
experience of Central Coast Stroke Services implementation of a pre-hospital notification system for expedient management of acute stroke. J Clin
Neurosci. 2012;19:241–245. doi: 10.1016/j.jocn.2011.06.009.
You JS, Chung SP, Chung HS, Lee HS, Park JW, Kim HJ, Lee SH, Park
I, Lee HS. Predictive value of the Cincinnati Prehospital Stroke Scale for
identifying thrombolytic candidates in acute ischemic stroke. Am J Emerg
Med. 2013;31:1699–1702. doi: 10.1016/j.ajem.2013.08.029.
Asimos AW, Ward S, Brice JH, Rosamond WD, Goldstein LB, Studnek
J. Out-of-hospital stroke screen accuracy in a state with an emergency
medical services protocol for routing patients to acute stroke centers. Ann
Emerg Med. 2014;64:509–515. doi: 10.1016/j.annemergmed.2014.03.024.
Bergs J, Sabbe M, Moons P. Prehospital stroke scales in a Belgian prehospital setting: a pilot study. Eur J Emerg Med. 2010;17:2–6. doi: 10.1097/
MEJ.0b013e32831040ec.
Bray JE, Coughlan K, Barger B, Bladin C. Paramedic diagnosis of
stroke: examining long-term use of the Melbourne Ambulance Stroke
Screen (MASS) in the field. Stroke. 2010;41:1363–1366. doi: 10.1161/
STROKEAHA.109.571836.
Bray JE, Martin J, Cooper G, Barger B, Bernard S, Bladin C. Paramedic
identification of stroke: community validation of the melbourne ambulance
stroke screen. Cerebrovasc Dis. 2005;20:28–33. doi: 10.1159/000086201.
Buck BH, Starkman S, Eckstein M, Kidwell CS, Haines J, Huang R,
Colby D, Saver JL. Dispatcher recognition of stroke using the National
Academy Medical Priority Dispatch System. Stroke. 2009;40:2027–2030.
doi: 10.1161/STROKEAHA.108.545574.
Chen S, Sun H, Lei Y, Gao D, Wang Y, Wang Y, Zhou Y, Wang A, Wang W,
Zhao X. Validation of the Los Angeles pre-hospital stroke screen (LAPSS)
in a Chinese urban emergency medical service population. PLoS One.
2013;8:e70742. doi: 10.1371/journal.pone.0070742.
De Luca A, Giorgi Rossi P, Villa GF; Stroke group Italian Society pre hospital emergency Services. The use of Cincinnati Prehospital Stroke Scale
during telephone dispatch interview increases the accuracy in identifying
stroke and transient ischemic attack symptoms. BMC Health Serv Res.
2013;13:513. doi: 10.1186/1472-6963-13-513.
Fothergill RT, Williams J, Edwards MJ, Russell IT, Gompertz P. Does
use of the recognition of stroke in the emergency room stroke assessment tool enhance stroke recognition by ambulance clinicians? Stroke.
2013;44:3007–3012. doi: 10.1161/STROKEAHA.13.000851.
Jiang HL, Chan CP, Leung YK, Li YM, Graham CA, Rainer TH. Evaluation
of the Recognition of Stroke in the Emergency Room (ROSIER) scale
in Chinese patients in Hong Kong. PLoS One. 2014;9:e109762. doi:
10.1371/journal.pone.0109762.
Kidwell CS, Starkman S, Eckstein M, Weems K, Saver JL. Identifying
stroke in the field. Prospective validation of the Los Angeles prehospital
stroke screen (LAPSS). Stroke. 2000;31:71–76.
Kleindorfer DO, Miller R, Moomaw CJ, Alwell K, Broderick JP, Khoury
J, Woo D, Flaherty ML, Zakaria T, Kissela BM. Designing a message for
public education regarding stroke: does FAST capture enough stroke?
Stroke. 2007;38:2864–2868. doi: 10.1161/STROKEAHA.107.484329.
Kothari RU, Pancioli A, Liu T, Brott T, Broderick J. Cincinnati
Prehospital Stroke Scale: reproducibility and validity. Ann Emerg Med.
1999;33:373–378.
Nazliel B, Starkman S, Liebeskind DS, Ovbiagele B, Kim D, Sanossian N,
Ali L, Buck B, Villablanca P, Vinuela F, Duckwiler G, Jahan R, Saver JL.
A brief prehospital stroke severity scale identifies ischemic stroke patients
harboring persisting large arterial occlusions. Stroke. 2008;39:2264–2267.
doi: 10.1161/STROKEAHA.107.508127.
Nor AM, Davis J, Sen B, Shipsey D, Louw SJ, Dyker AG, Davis M, Ford
GA. The Recognition of Stroke in the Emergency Room (ROSIER) scale:
development and validation of a stroke recognition instrument. Lancet
Neurol. 2005;4:727–734. doi: 10.1016/S1474-4422(05)70201-5.
Ramanujam P, Guluma KZ, Castillo EM, Chacon M, Jensen MB, Patel
E, Linnick W, Dunford JV. Accuracy of stroke recognition by emergency
�Singletary et al
66.
67.
68.
69.
70.
71.
72.
73.
74.
Downloaded from http://ahajournals.org by on May 27, 2020
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
medical dispatchers and paramedics–San Diego experience. Prehosp
Emerg Care. 2008;12:307–313. doi: 10.1080/10903120802099526.
Studnek JR, Asimos A, Dodds J, Swanson D. Assessing the validity of the
Cincinnati prehospital stroke scale and the medic prehospital assessment
for code stroke in an urban emergency medical services agency. Prehosp
Emerg Care. 2013;17:348–353. doi: 10.3109/10903127.2013.773113.
Whiteley WN, Wardlaw JM, Dennis MS, Sandercock PA. Clinical scores
for the identification of stroke and transient ischaemic attack in the emergency department: a cross-sectional study. J Neurol Neurosurg Psychiatry.
2011;82:1006–1010. doi: 10.1136/jnnp.2010.235010.
Yock-Corrales A, Babl FE, Mosley IT, Mackay MT. Can the FAST
and ROSIER adult stroke recognition tools be applied to confirmed
childhood arterial ischemic stroke? BMC Pediatr. 2011;11:93. doi:
10.1186/1471-2431-11-93.
Wall HK, Beagan BM, O’Neill J, Foell KM, Boddie-Willis CL. Addressing
stroke signs and symptoms through public education: the Stroke Heroes
Act FAST campaign. Prev Chronic Dis. 2008;5:A49.
Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS2. ISIS-2 (Second International Study of Infarct Survival) Collaborative
Group. Lancet. 1988;2:349-360.
Verheugt FW, van der Laarse A, Funke-Küpper AJ, Sterkman LG, Galema
TW, Roos JP. Effects of early intervention with low-dose aspirin (100 mg)
on infarct size, reinfarction and mortality in anterior wall acute myocardial
infarction. Am J Cardiol. 1990;66:267–270.
Elwood PC, Williams WO. A randomized controlled trial of aspirin in the
prevention of early mortality in myocardial infarction. J R Coll Gen Pract.
1979;29:413–416.
Frilling B, Schiele R, Gitt AK, Zahn R, Schneider S, Glunz HG, Gieseler
U, Baumgärtel B, Asbeck F, Senges J; Maximum Individual Therapy in
Acute Myocardial Infarction (MITRA); Myocardial Infarction Registry
(MIR) Study Groups. Characterization and clinical course of patients
not receiving aspirin for acute myocardial infarction: results from the
MITRA and MIR studies. Am Heart J. 2001;141:200–205. doi: 10.1067/
mhj.2001.112681.
Quan D, LoVecchio F, Clark B, Gallagher JV 3rd. Prehospital use of
aspirin rarely is associated with adverse events. Prehosp Disaster Med.
2004;19:362–365.
Freimark D, Matetzky S, Leor J, Boyko V, Barbash IM, Behar S, Hod H.
Timing of aspirin administration as a determinant of survival of patients
with acute myocardial infarction treated with thrombolysis. Am J Cardiol.
2002;89:381–385.
Barbash I, Freimark D, Gottlieb S, Hod H, Hasin Y, Battler A, Crystal E,
Matetzky S, Boyko V, Mandelzweig L, Behar S, Leor J; Israeli working
group on intensive cardiac care, Israel heart society. Outcome of myocardial infarction in patients treated with aspirin is enhanced by pre-hospital
administration. Cardiology. 2002;98:141–147. doi: 66324.
Inoue N, Yamamoto A. Clinical evaluation of pediatric anaphylaxis
and the necessity for multiple doses of epinephrine. Asia Pac Allergy.
2013;3:106–114. doi: 10.5415/apallergy.2013.3.2.106.
Järvinen KM, Sicherer SH, Sampson HA, Nowak-Wegrzyn A. Use
of multiple doses of epinephrine in food-induced anaphylaxis in children. J Allergy Clin Immunol. 2008;122:133–138. doi: 10.1016/j.
jaci.2008.04.031.
Noimark L, Wales J, Du Toit G, Pastacaldi C, Haddad D, Gardner J, Hyer
W, Vance G, Townshend C, Alfaham M, Arkwright PD, Rao R, Kapoor S,
Summerfield A, Warner JO, Roberts G. The use of adrenaline autoinjectors by children and teenagers. Clin Exp Allergy. 2012;42:284–292. doi:
10.1111/j.1365-2222.2011.03912.x.
Korenblat P, Lundie MJ, Dankner RE, Day JH. A retrospective study of
epinephrine administration for anaphylaxis: how many doses are needed?
Allergy Asthma Proc. 1999;20:383–386.
Oren E, Banerji A, Clark S, Camargo CA Jr. Food-induced anaphylaxis
and repeated epinephrine treatments. Ann Allergy Asthma Immunol.
2007;99:429–432. doi: 10.1016/S1081-1206(10)60568-6.
Banerji A, Rudders SA, Corel B, Garth AM, Clark S, Camargo CA Jr.
Repeat epinephrine treatments for food-related allergic reactions that present to the emergency department. Allergy Asthma Proc. 2010;31:308–316.
doi: 10.2500/aap.2010.31.3375.
Rudders SA, Banerji A, Corel B, Clark S, Camargo CA Jr. Multicenter
study of repeat epinephrine treatments for food-related anaphylaxis.
Pediatrics. 2010;125:e711–e718. doi: 10.1542/peds.2009-2832.
Tsuang A, Menon N, Setia N, Geyman L, Nowak-Wegrzyn AH. Multiple
epinephrine doses in food-induced anaphylaxis in children. J. Allergy
Clin. Immunol. 2013;131:AB90.
Part 9: First Aid
S309
85. Rudders SA, Banerji A, Katzman DP, Clark S, Camargo CA Jr. Multiple
epinephrine doses for stinging insect hypersensitivity reactions treated in
the emergency department. Ann Allergy Asthma Immunol. 2010;105:85–
93. doi: 10.1016/j.anai.2010.05.004.
86. Ellis BC, Brown SG. Efficacy of intramuscular epinephrine for the treatment of severe anaphylaxis: a comparison of two ambulance services
with different protocols. Ann. Emerg. Med. 2013;62:S146.
87. Brodows RG, Williams C, Amatruda JM. Treatment of insulin reactions
in diabetics. JAMA. 1984;252:3378–3381.
88. Husband AC, Crawford S, McCoy LA, Pacaud D. The effectiveness
of glucose, sucrose, and fructose in treating hypoglycemia in children with type 1 diabetes. Pediatr Diabetes. 2010;11:154–158. doi:
10.1111/j.1399-5448.2009.00558.x.
89. McTavish L, Wiltshire E. Effective treatment of hypoglycemia in children with type 1 diabetes: a randomized controlled
clinical trial. Pediatr Diabetes. 2011;12(4 Pt 2):381–387. doi:
10.1111/j.1399-5448.2010.00725.x.
90. Slama G, Traynard PY, Desplanque N, Pudar H, Dhunputh I, Letanoux
M, Bornet FR, Tchobroutsky G. The search for an optimized treatment
of hypoglycemia. Carbohydrates in tablets, solutin, or gel for the correction of insulin reactions. Arch Intern Med. 1990;150:589–593.
91. Osterberg KL, Pallardy SE, Johnson RJ, Horswill CA. Carbohydrate
exerts a mild influence on fluid retention following exercise-induced
dehydration. J Appl Physiol (1985). 2010;108:245–250. doi: 10.1152/
japplphysiol.91275.2008.
92. Saat M, Singh R, Sirisinghe RG, Nawawi M. Rehydration after exercise
with fresh young coconut water, carbohydrate-electrolyte beverage and
plain water. J Physiol Anthropol Appl Human Sci. 2002;21:93–104.
93. Ismail I, Singh R, Sirisinghe RG. Rehydration with sodium-enriched
coconut water after exercise-induced dehydration. Southeast Asian J
Trop Med Public Health. 2007;38:769–785.
94. González-Alonso J, Heaps CL, Coyle EF. Rehydration after exercise
with common beverages and water. Int J Sports Med. 1992;13:399–406.
95. Wong SH, Williams C, Adams N. Effects of ingesting a large volume
of carbohydrate-electrolyte solution on rehydration during recovery and subsequent exercise capacity. Int J Sport Nutr Exerc Metab.
2000;10:375–393.
96. Kalman DS, Feldman S, Krieger DR, Bloomer RJ. Comparison of coconut water and a carbohydrate-electrolyte sport drink on measures of
hydration and physical performance in exercise-trained men. J Int Soc
Sports Nutr. 2012;9:1. doi: 10.1186/1550-2783-9-1.
97. Chang CQ, Chen YB, Chen ZM, Zhang LT. Effects of a carbohydrateelectrolyte beverage on blood viscosity after dehydration in healthy
adults. Chin Med J (Engl). 2010;123:3220–3225.
98. Seifert J, Harmon J, DeClercq P. Protein added to a sports drink improves
fluid retention. Int J Sport Nutr Exerc Metab. 2006;16:420–429.
99. Wong SH, Chen Y. Effect of a carbohydrate-electrolyte beverage, lemon
tea, or water on rehydration during short-term recovery from exercise.
Int J Sport Nutr Exerc Metab. 2011;21:300–310.
100. Shirreffs SM, Watson P, Maughan RJ. Milk as an effective post-exercise rehydration drink. Br J Nutr. 2007;98:173–180. doi: 10.1017/
S0007114507695543.
101. Hostler D, Bednez JC, Kerin S, Reis SE, Kong PW, Morley J, Gallagher
M, Suyama J. Comparison of rehydration regimens for rehabilitation of
firefighters performing heavy exercise in thermal protective clothing: a
report from the fireground rehab evaluation (FIRE) trial. Prehosp Emerg
Care. 2010;14:194–201. doi: 10.3109/10903120903524963.
102. Miccheli A, Marini F, Capuani G, Miccheli AT, Delfini M, Di Cocco
ME, Puccetti C, Paci M, Rizzo M, Spataro A. The influence of a sports
drink on the postexercise metabolism of elite athletes as investigated by
NMR-based metabolomics. J Am Coll Nutr. 2009;28:553–564.
103. Kompa S, Redbrake C, Hilgers C, Wüstemeyer H, Schrage N, Remky
A. Effect of different irrigating solutions on aqueous humour pH
changes, intraocular pressure and histological findings after induced
alkali burns. Acta Ophthalmol Scand. 2005;83:467–470. doi:
10.1111/j.1600-0420.2005.00458.x.
104. King NA, Philpott SJ, Leary A. A randomized controlled trial assessing
the use of compression versus vasoconstriction in the treatment of femoral hematoma occurring after percutaneous coronary intervention. Heart
Lung. 2008;37:205–210. doi: 10.1016/j.hrtlng.2007.05.008.
105. Levy AS, Marmar E. The role of cold compression dressings in the postoperative treatment of total knee arthroplasty. Clin Orthop Relat Res.
1993:174–178.
�S310
Circulation
October 20, 2015
Downloaded from http://ahajournals.org by on May 27, 2020
106. Cox ED, Schreiber MA, McManus J, Wade CE, Holcomb JB. New
hemostatic agents in the combat setting. Transfusion. 2009;49 Suppl
5:248S–255S. doi: 10.1111/j.1537-2995.2008.01988.x.
107. Acheson EM, Kheirabadi BS, Deguzman R, Dick EJ Jr, Holcomb JB.
Comparison of hemorrhage control agents applied to lethal extremity arterial hemorrhages in swine. J Trauma. 2005;59:865–74; discussion 874.
108. Alam HB, Uy GB, Miller D, Koustova E, Hancock T, Inocencio R,
Anderson D, Llorente O, Rhee P. Comparative analysis of hemostatic
agents in a swine model of lethal groin injury. J Trauma. 2003;54:1077–
1082. doi: 10.1097/01.TA.0000068258.99048.70.
109. Arnaud F, Parreño-Sadalan D, Tomori T, Delima MG, Teranishi K, Carr
W, McNamee G, McKeague A, Govindaraj K, Beadling C, Lutz C, Sharp
T, Mog S, Burris D, McCarron R. Comparison of 10 hemostatic dressings in a groin transection model in swine. J Trauma. 2009;67:848–855.
doi: 10.1097/TA.0b013e3181b2897f.
110. Arnaud F, Teranishi K, Tomori T, Carr W, McCarron R. Comparison of
10 hemostatic dressings in a groin puncture model in swine. J Vasc Surg.
2009;50:632–9, 639.e1. doi: 10.1016/j.jvs.2009.06.010.
111. Devlin JJ, Kircher S, Kozen BG, Littlejohn LF, Johnson AS. Comparison
of ChitoFlex®, CELOX™, and QuikClot® in control of hemorrhage. J
Emerg Med. 2011;41:237–245. doi: 10.1016/j.jemermed.2009.02.017.
112. Kheirabadi BS, Scherer MR, Estep JS, Dubick MA, Holcomb JB.
Determination of efficacy of new hemostatic dressings in a model of
extremity arterial hemorrhage in swine. J Trauma. 2009;67:450–9; discussion 459. doi: 10.1097/TA.0b013e3181ac0c99.
113. Kozen BG, Kircher SJ, Henao J, Godinez FS, Johnson AS.
An alternative hemostatic dressing: comparison of CELOX,
HemCon, and QuikClot. Acad Emerg Med. 2008;15:74–81. doi:
10.1111/j.1553-2712.2007.00009.x.
114. Brown MA, Daya MR, Worley JA. Experience with chitosan dressings
in a civilian EMS system. J Emerg Med. 2009;37:1–7. doi: 10.1016/j.
jemermed.2007.05.043.
115. Ran Y, Hadad E, Daher S, Ganor O, Kohn J, Yegorov Y, Bartal C, Ash
N, Hirschhorn G. QuikClot Combat Gauze use for hemorrhage control
in military trauma: January 2009 Israel Defense Force experience in the
Gaza Strip–a preliminary report of 14 cases. Prehosp Disaster Med.
2010;25:584–588.
116. Wedmore I, McManus JG, Pusateri AE, Holcomb JB. A special
report on the chitosan-based hemostatic dressing: experience in current combat operations. J Trauma. 2006;60:655–658. doi: 10.1097/01.
ta.0000199392.91772.44.
117. Causey MW, McVay DP, Miller S, Beekley A, Martin M. The efficacy of Combat Gauze in extreme physiologic conditions. J Surg Res.
2012;177:301–305. doi: 10.1016/j.jss.2012.06.020.
118. Beekley AC, Sebesta JA, Blackbourne LH, Herbert GS, Kauvar
DS, Baer DG, Walters TJ, Mullenix PS, Holcomb JB; 31st Combat
Support Hospital Research Group. Prehospital tourniquet use in
Operation Iraqi Freedom: effect on hemorrhage control and outcomes.
J Trauma. 2008;64(2 Suppl):S28–37; discussion S37. doi: 10.1097/
TA.0b013e318160937e.
119. Guo JY, Liu Y, Ma YL, Pi HY, Wang JR. Evaluation of emergency tourniquets for prehospital use in China. Chin J Traumatol.
2011;14:151–155.
120. King DR, van der Wilden G, Kragh JF Jr, Blackbourne LH. Forward
assessment of 79 prehospital battlefield tourniquets used in the current
war. J Spec Oper Med. 2012;12:33–38.
121. Kue RC, Temin ES, Weiner SG, Gates J, Coleman MH, Fisher J, Dyer
S. Tourniquet Use in a Civilian Emergency Medical Services Setting: A
Descriptive Analysis of the Boston EMS Experience. Prehosp Emerg
Care. 2015;19:399–404. doi: 10.3109/10903127.2014.995842.
122. Lakstein D, Blumenfeld A, Sokolov T, Lin G, Bssorai R, Lynn M, BenAbraham R. Tourniquets for hemorrhage control on the battlefield: a
4-year accumulated experience. J Trauma. 2003;54(5 Suppl):S221–
S225. doi: 10.1097/01.TA.0000047227.33395.49.
123. Swan KG Jr, Wright DS, Barbagiovanni SS, Swan BC, Swan KG.
Tourniquets revisited. J Trauma. 2009;66:672–675. doi: 10.1097/
TA.0b013e3181986959.
124. Passos E, Dingley B, Smith A, Engels PT, Ball CG, Faidi S, Nathens
A, Tien H; Canadian Trauma Trials Collaborative. Tourniquet use for
peripheral vascular injuries in the civilian setting. Injury. 2014;45:573–
577. doi: 10.1016/j.injury.2013.11.031.
125. Kragh JF Jr, Nam JJ, Berry KA, Mase VJ Jr, Aden JK 3rd, Walters TJ,
Dubick MA, Baer DG, Wade CE, Blackbourne LH. Transfusion for shock
in US military war casualties with and without tourniquet use. Ann Emerg
Med. 2015;65:290–296. doi: 10.1016/j.annemergmed.2014.10.021.
126. Brodie S, Hodgetts TJ, Ollerton J, McLeod J, Lambert P, Mahoney P.
Tourniquet use in combat trauma: UK military experience. J R Army
Med Corps. 2007;153:310–313.
127. Kragh JF Jr, Littrel ML, Jones JA, Walters TJ, Baer DG, Wade CE,
Holcomb JB. Battle casualty survival with emergency tourniquet use
to stop limb bleeding. J Emerg Med. 2011;41:590–597. doi: 10.1016/j.
jemermed.2009.07.022.
128. Kragh JF Jr, Cooper A, Aden JK, Dubick MA, Baer DG, Wade CE,
Blackbourne LH. Survey of trauma registry data on tourniquet use in
pediatric war casualties. Pediatr Emerg Care. 2012;28:1361–1365. doi:
10.1097/PEC.0b013e318276c260.
129. Tien HC, Jung V, Rizoli SB, Acharya SV, MacDonald JC. An evaluation of tactical combat casualty care interventions in a combat
environment. J Am Coll Surg. 2008;207:174–178. doi: 10.1016/j.
jamcollsurg.2008.01.065.
130. Kheirabadi BS, Terrazas IB, Koller A, Allen PB, Klemcke HG,
Convertino VA, Dubick MA, Gerhardt RT, Blackbourne LH. Vented versus unvented chest seals for treatment of pneumothorax and prevention
of tension pneumothorax in a swine model. J Trauma Acute Care Surg.
2013;75:150–156.
131. Lin HL, Lee WC, Chen CW, Lin TY, Cheng YC, Yeh YS, Lin YK, Kuo
LC. Neck collar used in treatment of victims of urban motorcycle accidents: over- or underprotection? Am J Emerg Med. 2011;29:1028–1033.
doi: 10.1016/j.ajem.2010.06.003.
132. Davies G, Deakin C, Wilson A. The effect of a rigid collar on intracranial
pressure. Injury. 1996;27:647–649.
133. Hunt K, Hallworth S, Smith M. The effects of rigid collar placement on intracranial and cerebral perfusion pressures. Anaesthesia.
2001;56:511–513.
134. Mobbs RJ, Stoodley MA, Fuller J. Effect of cervical hard collar on intracranial pressure after head injury. ANZ J Surg. 2002;72:389–391.
135. Kolb JC, Summers RL, Galli RL. Cervical collar-induced changes in
intracranial pressure. Am J Emerg Med. 1999;17:135–137.
136. Raphael JH, Chotai R. Effects of the cervical collar on cerebrospinal
fluid pressure. Anaesthesia. 1994;49:437–439.
137. Stone MB, Tubridy CM, Curran R. The effect of rigid cervical collars on
internal jugular vein dimensions. Acad Emerg Med. 2010;17:100–102.
doi: 10.1111/j.1553-2712.2009.00624.x.
138. Dodd FM, Simon E, McKeown D, Patrick MR. The effect of a cervical
collar on the tidal volume of anaesthetised adult patients. Anaesthesia.
1995;50:961–963.
139. Treloar DJ, Nypaver M. Angulation of the pediatric cervical spine with
and without cervical collar. Pediatr Emerg Care. 1997;13:5–8.
140. Podolsky S, Baraff LJ, Simon RR, Hoffman JR, Larmon B, Ablon
W. Efficacy of cervical spine immobilization methods. J Trauma.
1983;23:461–465.
141. Tescher AN, Rindflesch AB, Youdas JW, Jacobson TM, Downer LL,
Miers AG, Basford JR, Cullinane DC, Stevens SR, Pankratz VS, Decker
PA. Range-of-motion restriction and craniofacial tissue-interface pressure from four cervical collars. J Trauma. 2007;63:1120–1126. doi:
10.1097/TA.0b013e3180487d0f.
142. Zhang S, Wortley M, Clowers K, Krusenklaus JH. Evaluation of
efficacy and 3D kinematic characteristics of cervical orthoses.
Clin Biomech (Bristol, Avon). 2005;20:264–269. doi: 10.1016/j.
clinbiomech.2004.09.015.
143. Horodyski M, DiPaola CP, Conrad BP, Rechtine GR 2nd. Cervical collars are insufficient for immobilizing an unstable cervical spine injury.
J Emerg Med. 2011;41:513–519. doi: 10.1016/j.jemermed.2011.02.001.
144. Conrad BP, Rechtine G, Weight M, Clarke J, Horodyski M. Motion
in the unstable cervical spine during hospital bed transfers. J Trauma.
2010;69:432–436. doi: 10.1097/TA.0b013e3181e89f58.
145. Del Rossi G, Heffernan TP, Horodyski M, Rechtine GR. The effectiveness of extrication collars tested during the execution of spineboard transfer techniques. Spine J. 2004;4:619–623. doi: 10.1016/j.
spinee.2004.06.018.
146. Rosen PB, McSwain NE Jr, Arata M, Stahl S, Mercer D. Comparison of
two new immobilization collars. Ann Emerg Med. 1992;21:1189–1195.
147. Bednar DA. Efficacy of orthotic immobilization of the unstable subaxial
cervical spine of the elderly patient: investigation in a cadaver model.
Can J Surg. 2004;47:251–256.
148. Evans NR, Hooper G, Edwards R, Whatling G, Sparkes V, Holt C,
Ahuja S. A 3D motion analysis study comparing the effectiveness of
cervical spine orthoses at restricting spinal motion through physiological ranges. Eur Spine J. 2013;22 Suppl 1:S10–S15. doi: 10.1007/
s00586-012-2641-0.
�Singletary et al
Downloaded from http://ahajournals.org by on May 27, 2020
149. DiPaola MJ, DiPaola CP, Conrad BP, Horodyski M, Del Rossi G,
Sawers A, Bloch D, Rechtine GR 2nd. Cervical spine motion in manual versus Jackson table turning methods in a cadaveric global instability model. J Spinal Disord Tech. 2008;21:273–280. doi: 10.1097/
BSD.0b013e31811513a4.
150. Fisher SV, Bowar JF, Awad EA, Gullickson G Jr. Cervical orthoses effect
on cervical spine motion: roentgenographic and goniometric method of
study. Arch Phys Med Rehabil. 1977;58:109–115.
151. Sandler AJ, Dvorak J, Humke T, Grob D, Daniels W. The effectiveness
of various cervical orthoses. An in vivo comparison of the mechanical
stability provided by several widely used models. Spine (Phila Pa 1976).
1996;21:1624–1629.
152. Hughes SJ. How effective is the Newport/Aspen collar? A prospective radiographic evaluation in healthy adult volunteers. J Trauma.
1998;45:374–378.
153. Gavin TM, Carandang G, Havey R, Flanagan P, Ghanayem A,
Patwardhan AG. Biomechanical analysis of cervical orthoses in flexion
and extension: a comparison of cervical collars and cervical thoracic
orthoses. J Rehabil Res Dev. 2003;40:527–537.
154. Askins V, Eismont FJ. Efficacy of five cervical orthoses in restricting cervical
motion. A comparison study. Spine (Phila Pa 1976). 1997;22:1193–1198.
155. Cline JR, Scheidel E, Bigsby EF. A comparison of methods of cervical immobilization used in patient extrication and transport. J Trauma.
1985;25:649–653.
156. Ben-Galim P, Dreiangel N, Mattox KL, Reitman CA, Kalantar SB, Hipp
JA. Extrication collars can result in abnormal separation between vertebrae in the presence of a dissociative injury. J Trauma. 2010;69:447–
450. doi: 10.1097/TA.0b013e3181be785a.
157. Burl MM. Effectiveness of cervical collars in limiting movement
Physiotherapy. 1991;77:308–310.
158. Hamilton RS, Pons PT. The efficacy and comfort of full-body
vacuum splints for cervical-spine immobilization. J Emerg Med.
1996;14:553–559.
159. Richter D, Latta LL, Milne EL, Varkarakis GM, Biedermann L,
Ekkernkamp A, Ostermann PA. The stabilizing effects of different orthoses in the intact and unstable upper cervical spine: a cadaver study. J
Trauma. 2001;50:848–854.
160. Thompson DO, Hurtado TR, Liao MM, Byyny RL, Gravitz C, Haukoos
JS. Validation of the Simplified Motor Score in the out-of-hospital setting
for the prediction of outcomes after traumatic brain injury. Ann Emerg
Med. 2011;58:417–425. doi: 10.1016/j.annemergmed.2011.05.033.
161. Werner MU, Lassen B, Pedersen JL, Kehlet H. Local cooling does
not prevent hyperalgesia following burn injury in humans. Pain.
2002;98:297–303.
162. Yava A, Koyuncu A, Tosun N, Kiliç S. Effectiveness of local cold application on skin burns and pain after transthoracic cardioversion. Emerg
Med J. 2012;29:544–549. doi: 10.1136/emj.2010.098053.
163. Nguyen NL, Gun RT, Sparnon AL, Ryan P. The importance of immediate cooling–a case series of childhood burns in Vietnam. Burns.
2002;28:173–176.
164. Cuttle L, Kravchuk O, Wallis B, Kimble RM. An audit of first-aid treatment of pediatric burns patients and their clinical outcome. J Burn Care
Res. 2009;30:1028–1034. doi: 10.1097/BCR.0b013e3181bfb7d1.
165. Sunder S, Bharat R. Industrial burns in Jamshedpur, India: epidemiology, prevention and first aid. Burns. 1998;24:444–447.
166. Skinner AM, Brown TL, Peat BG, Muller MJ. Reduced hospitalisation
of burns patients following a multi-media campaign that increased adequacy of first aid treatment. Burns. 2004;30:82–85.
167. Subrahmanyam M. Topical application of honey in treatment of burns.
Br J Surg. 1991;78:497–498.
Part 9: First Aid
S311
168. Subrahmanyam M. Honey dressing versus boiled potato peel in the treatment of burns: a prospective randomized study. Burns. 1996;22:491–493.
169. Heinrich JJ, Brand DA, Cuono CB. The role of topical treatment as a
determinant of infection in outpatient burns. J Burn Care Rehabil.
1988;9:253–257.
170. Khademi AA, Saei S, Mohajeri MR, Mirkheshti N, Ghassami F, Torabi
nia N, Alavi SA. A new storage medium for an avulsed tooth. J Contemp
Dent Pract. 2008;9:25–32.
171. Ahangari Z, Alborzi S, Yadegari Z, Dehghani F, Ahangari L, Naseri
M. The effect of propolis as a biological storage media on periodontal ligament cell survival in an avulsed tooth: an in vitro study. Cell J.
2013;15:244–249.
172. Rajendran P, Varghese NO, Varughese JM, Murugaian E. Evaluation,
using extracted human teeth, of Ricetral as a storage medium for
avulsions–an in vitro study. Dent Traumatol. 2011;27:217–220. doi:
10.1111/j.1600-9657.2011.00988.x.
173. Gopikrishna V, Thomas T, Kandaswamy D. A quantitative analysis of
coconut water: a new storage media for avulsed teeth. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod. 2008;105:e61–e65. doi: 10.1016/j.
tripleo.2007.08.003.
174. Caglar E, Sandalli N, Kuscu OO, Durhan MA, Pisiriciler R, Caliskan EA,
Kargul B. Viability of fibroblasts in a novel probiotic storage media. Dent
Traumatol. 2010;26:383–387. doi: 10.1111/j.1600-9657.2010.00914.x.
175. Lekic PC, Kenny DJ, Barrett EJ. The influence of storage conditions on
the clonogenic capacity of periodontal ligament cells: implications for
tooth replantation. Int Endod J. 1998;31:137–140.
176. Chen H, Huang B. (-)-Epigallocatechin-3-gallate: a novel storage
medium for avulsed teeth. Dent Traumatol. 2012;28:158–160. doi:
10.1111/j.1600-9657.2011.01066.x.
177. Pileggi R, Dumsha TC, Nor JE. Assessment of post-traumatic
PDL cells viability by a novel collagenase assay. Dent Traumatol.
2002;18:186–189.
178. Martin MP, Pileggi R. A quantitative analysis of Propolis: a promising
new storage media following avulsion. Dent Traumatol. 2004;20:85–89.
doi: 10.1111/j.1600-4469.2004.00233.x.
179. Doyle DL, Dumsha TC, Sydiskis RJ. Effect of soaking in Hank’s balanced salt solution or milk on PDL cell viability of dry stored human
teeth. Endod Dent Traumatol. 1998;14:221–224.
180. Patel S, Dumsha TC, Sydiskis RJ. Determining periodontal ligament
(PDL) cell vitality from exarticulated teeth stored in saline or milk using
fluorescein diacetate. Int Endod J. 1994;27:1–5.
181. Werder P, von Arx T, Chappuis V. Treatment outcome of 42 replanted
permanent incisors with a median follow-up of 2.8 years. Schweiz
Monatsschr Zahnmed. 2011;121:312–320.
182. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation
of 400 avulsed permanent incisors. 2. Factors related to pulpal healing.
Endod Dent Traumatol. 1995;11:59–68.
183. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation
of 400 avulsed permanent incisors. 4. Factors related to periodontal ligament healing. Endod Dent Traumatol. 1995;11:76–89.
184. Murad MK, Husum H. Trained lay first responders reduce trauma mortality: a controlled study of rural trauma in Iraq. Prehosp Disaster Med.
2010;25:533–539.
185. Ditty J, Chisholm D, Davis SM, Estelle-Schmidt M. Safety and efficacy
of attempts to reduce shoulder dislocations by non-medical personnel in
the wilderness setting. Wilderness Environ Med. 2010;21:357–361.e2.
doi: 10.1016/j.wem.2010.06.010.
KEY WORDS: anaphylaxis ◼ asthma ◼ burns ◼ hypoglycemia ◼ shock
◼ trauma emergencies
�
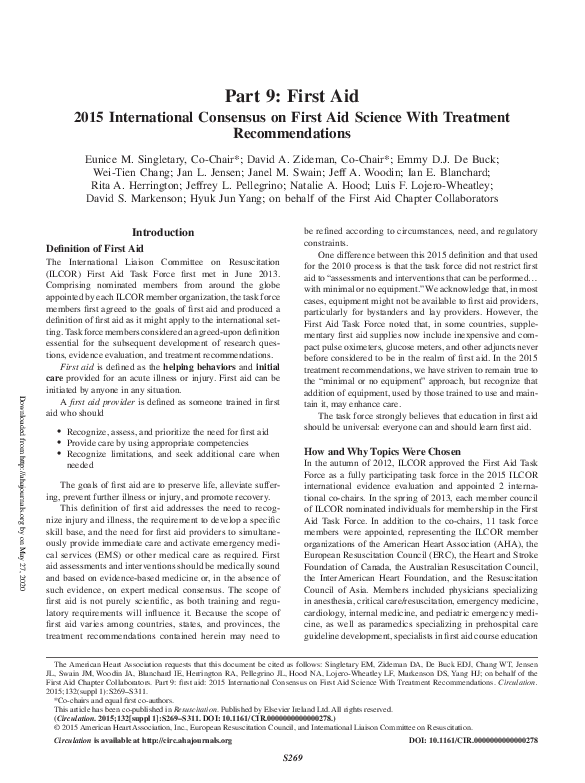
 Anthony Handley
Anthony Handley