Correspondence
2
1·00
ODA/GNI %
0·80
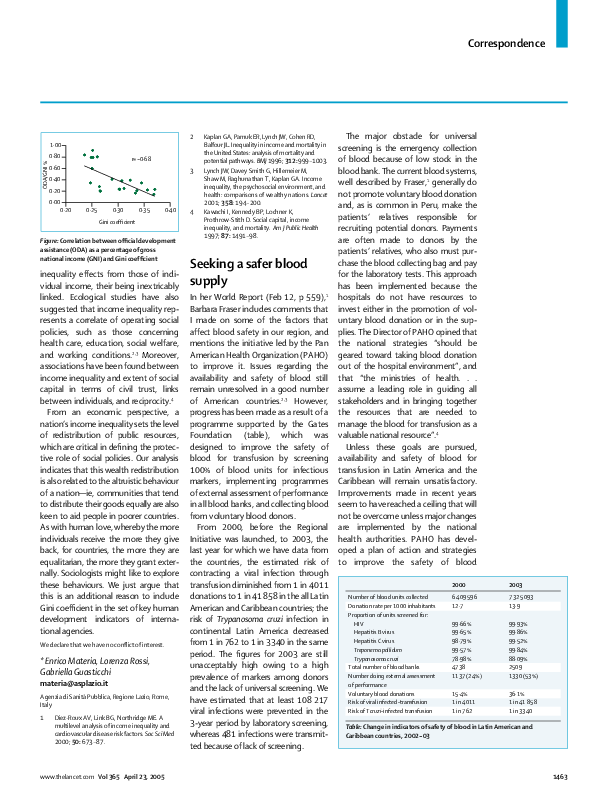
r=–0·68
0·60
3
0·40
0·20
0·00
0·20
0·25
0·30
0·35
0·40
Gini coefficient
Figure: Correlation between official development
assistance (ODA) as a percentage of gross
national income (GNI) and Gini coefficient
inequality effects from those of individual income, their being inextricably
linked. Ecological studies have also
suggested that income inequality represents a correlate of operating social
policies, such as those concerning
health care, education, social welfare,
and working conditions.2,3 Moreover,
associations have been found between
income inequality and extent of social
capital in terms of civil trust, links
between individuals, and reciprocity.4
From an economic perspective, a
nation’s income inequality sets the level
of redistribution of public resources,
which are critical in defining the protective role of social policies. Our analysis
indicates that this wealth redistribution
is also related to the altruistic behaviour
of a nation—ie, communities that tend
to distribute their goods equally are also
keen to aid people in poorer countries.
As with human love, whereby the more
individuals receive the more they give
back, for countries, the more they are
equalitarian, the more they grant externally. Sociologists might like to explore
these behaviours. We just argue that
this is an additional reason to include
Gini coefficient in the set of key human
development indicators of international agencies.
We declare that we have no conflict of interest.
*Enrico Materia, Lorenza Rossi,
Gabriella Guasticchi
materia@asplazio.it
Agenzia di Sanità Pubblica, Regione Lazio, Rome,
Italy
1
Diez-Roux AV, Link BG, Northridge ME. A
multilevel analysis of income inequality and
cardiovascular disease risk factors. Soc Sci Med
2000; 50: 673–87.
www.thelancet.com Vol 365 April 23, 2005
4
Kaplan GA, Pamuk ER, Lynch JW, Cohen RD,
Balfour JL. Inequality in income and mortality in
the United States: analysis of mortality and
potential pathways. BMJ 1996; 312: 999–1003.
Lynch JW, Davey Smith G, Hillemeier M,
Shaw M, Raghunathan T, Kaplan GA. Income
inequality, the psychosocial environment, and
health: comparisons of wealthy nations. Lancet
2001; 358: 194–200.
Kawachi I, Kennedy BP, Lochner K,
Prothrow-Stith D. Social capital, income
inequality, and mortality. Am J Public Health
1997; 87: 1491–98.
Seeking a safer blood
supply
In her World Report (Feb 12, p 559),1
Barbara Fraser includes comments that
I made on some of the factors that
affect blood safety in our region, and
mentions the initiative led by the Pan
American Health Organization (PAHO)
to improve it. Issues regarding the
availability and safety of blood still
remain unresolved in a good number
of American countries.2,3 However,
progress has been made as a result of a
programme supported by the Gates
Foundation (table), which was
designed to improve the safety of
blood for transfusion by screening
100% of blood units for infectious
markers, implementing programmes
of external assessment of performance
in all blood banks, and collecting blood
from voluntary blood donors.
From 2000, before the Regional
Initiative was launched, to 2003, the
last year for which we have data from
the countries, the estimated risk of
contracting a viral infection through
transfusion diminished from 1 in 4011
donations to 1 in 41 858 in the all Latin
American and Caribbean countries; the
risk of Trypanosoma cruzi infection in
continental Latin America decreased
from 1 in 762 to 1 in 3340 in the same
period. The figures for 2003 are still
unacceptably high owing to a high
prevalence of markers among donors
and the lack of universal screening. We
have estimated that at least 108 217
viral infections were prevented in the
3-year period by laboratory screening,
whereas 481 infections were transmitted because of lack of screening.
The major obstacle for universal
screening is the emergency collection
of blood because of low stock in the
blood bank. The current blood systems,
well described by Fraser,1 generally do
not promote voluntary blood donation
and, as is common in Peru, make the
patients’ relatives responsible for
recruiting potential donors. Payments
are often made to donors by the
patients’ relatives, who also must purchase the blood collecting bag and pay
for the laboratory tests. This approach
has been implemented because the
hospitals do not have resources to
invest either in the promotion of voluntary blood donation or in the supplies. The Director of PAHO opined that
the national strategies “should be
geared toward taking blood donation
out of the hospital environment”, and
that “the ministries of health. . .
assume a leading role in guiding all
stakeholders and in bringing together
the resources that are needed to
manage the blood for transfusion as a
valuable national resource”.4
Unless these goals are pursued,
availability and safety of blood for
transfusion in Latin America and the
Caribbean will remain unsatisfactory.
Improvements made in recent years
seem to have reached a ceiling that will
not be overcome unless major changes
are implemented by the national
health authorities. PAHO has developed a plan of action and strategies
to improve the safety of blood
Number of blood units collected
Donation rate per 1000 inhabitants
Proportion of units screened for:
HIV
Hepatitis B virus
Hepatitis C virus
Treponema pallidum
Trypanosoma cruzi
Total number of blood banks
Number doing external assessment
of performance
Voluntary blood donations
Risk of viral infected-transfusion
Risk of T cruzi-infected transfusion
2000
2003
6 409 596
12·7
7 325 093
13·9
99·66%
99·65%
98·79%
99·57%
78·98%
4738
1137 (24%)
99·93%
99·86%
99·52%
99·84%
88·09%
2509
1330 (53%)
15·4%
1 in 4011
1 in 762
36·1%
1 in 41 858
1 in 3340
Table: Change in indicators of safety of blood in Latin American and
Caribbean countries, 2002–03
1463
�Correspondence
transfusion—not just the transfused
products—in the next 5 years. This
plan is expected to be implemented as
a Regional Program.
I declare that I have no conflict of interest.
José Ramiro Cruz
cruzjose@paho.org
Regional Advisor Laboratory and Blood Services, Pan
American Health Organization, 525 23rd Street NW,
Washington, DC 20037, USA
1
2
3
4
Fraser B. Seeking a safer blood supply. Lancet
2005; 365: 559–60.
Cruz JR, Perez-Rosales MD. Availability, safety
and quality of blood for transfusion in the
Americas. Pan Am J Public Health 2003; 13:
103–09.
Schmunis GA, Cruz JR. Safety of the blood
supply in Latin America. Clin Rev Microbiol
2005; 18: 12–29.
Roses Periago M. Promoting quality blood
services in the Region of the Americas.
Pan Am J Public Health 2003; 13: 73–74.
Barbara Fraser’s World Report1 on blood
transfusion safety highlights the critical
shortcomings of transfusion practices
in the developing world. More than
80% of the world’s population has
access to only 20% of the world’s safe
blood supply.2 And it is this population
that has a high demand for blood products. Southeast Asia, for example, collects only 7 million units of the
15 million units of blood that it requires
annually. Many of the 150 000 women
who die each year from blood loss due
to pregnancy-associated causes might
live if sufficient blood is available.3
This gap between supply and
demand further compromises the adequate provision of safe blood. In such
situations, blood is more likely to be
bought from private blood banks,
which are more inclined to compromise safety standards. The global contribution of developing countries to
blood collection from altruistic donors
stands at a meagre 16%.3 Replacement
and paid donors provide the bulk of
donations. Indeed, unsafe blood
accounts for 8–16 million hepatitis B
virus infections, 2·3–4·7 million
hepatitis C virus infections, and
80 000–160 000 HIV infections annually.3 Aside from the shortage problem
and transfusion-transmitted infections, the complications associated
1464
with transfusion reactions in these
settings are largely unknown.
Pakistan is a country with a human
development index of 142. The
reported prevalences of hepatitis B and
C are 5–8% and 7–10%, respectively.
About 50% of blood banks in Karachi,
the largest city in Pakistan, regularly
employ paid blood donors.4 An average
patient receiving two units of blood has
a 10% chance of acquiring hepatitis C
infection.4 Altruistic donors account for
only 5% of all donors. The national
blood policy announced in 2003 has
been termed a step in the right direction. As a result, more than 90% of the
blood is properly screened in public hospitals. However, there are shortcomings
in implementation, particularly relating
to the private blood banks which
greatly outnumber public blood banks.
It is important to remember that
poverty remains the underlying cause
in the developing world for the present situation. Weak infrastructure, illequipped centres, poorly trained staff,
inadequate policy implementation,
and frequent power breakdowns are
problems needing rectification for a
sustainable solution.
Although badly needed, altruistic
donors in developing countries will be
difficult to come by owing to wellestablished traditional beliefs and practices.5 The perceptions and concerns of
people regarding transfusions must be
assessed to formulate targeted educational strategies and mobilise donors. It
is also important to enforce transfusion
guidelines strictly to avoid unnecessary
transfusions. Donor screening is an
effective although underused strategy
in the developing countries. Questions
about high-risk behaviour are seldom
asked.4,5 The high cost of screening
assays often leads to blood being
screened only if the patient is willing to
pay.4 Screening costs must be reduced
by developing cost-effective assays,
pooled testing,5 and eliminating
import duties on essential equipment.
A concerted effort to address these
problems will significantly improve the
situation in the years to come.
We declare that we have no conflict of interest.
*Fawad Aslam, Junaid Ali Syed
fawadaslam2@hotmail.com
Male Hostel, Aga Khan University Medical College,
Stadium Road, Karachi 74800, Pakistan
1
2
3
4
5
Fraser B. Seeking a safer blood supply. Lancet
2005; 365: 559–60.
Larkin M. WHO’s blood-safety initiative: a vain
effort? Lancet 2000; 355: 1245.
World Health Organization. Safe blood starts
with me! Blood saves lives! Stories and
souvenirs from World Health Day 2000
together with useful information on blood
safety. http://www.who.int/bloodsafety/en/
WHD_Safe_Blood_2000.pdf (accessed Feb 21,
2005).
Luby S, Khanani R, Zia M, et al. Evaluation of
blood bank practices in Karachi, Pakistan, and
the government’s response. Health Policy Plan
2000; 15: 217–22.
Wake DJ, Cutting WA. Blood transfusion in
developing countries: problems, priorities and
practicalities. Trop Doct 1998; 28: 4–8.
CT colonography for
detection of colon
polyps and cancer
The mediocre results obtained for
computed tomographic colonography
(CTC) by D C Rockey and colleagues
(Jan 22, p 305)1 raise questions about
the examination techniques used in
conducting this important new imaging procedure. Rockey and colleagues
do not provide key data in several
areas. The first is colon preparation.
What measure was used to assess
adequacy of gas insufflation? This is
an essential part of “preparation”, but
was not directly addressed in the
report. Also, was there any attempt to
score retained fluid which is commonly
found with preparation regimens
used for colonoscopy? Polyps are
sometimes hidden by dependent fluid
collections.
Were there explicit formal criteria by
which a site or reader could initially
participate in the study and then be
retained subsequently on the basis of
number of patients contributed and
performance? Are there any readerspecific or site-specific performance
data to further illuminate the apparent
lack of effect of previous experience?
Moreover, the radiologists were not
www.thelancet.com Vol 365 April 23, 2005
�
 jose cruz
jose cruz