2
INSIDE DENTISTRY—APRIL 2007
inside
EnDodoNtics
Resilon Update
Gregori M. Kurtzman, DDS
Traditionally, endodontic treatment requires instrumentation of the root
canal to remove infectious debris, leaving
clean canal walls. After the instrumentation and irrigation of debris from the canal is complete, the root canal is filled with
gutta-percha inserted with an endodontic
sealer. These sealers to be used with gutta
percha have included calcium hydroxides,
zinc-oxide and eugenol cements, and glass
ionomer cements. When Resilon™ (Pentron® Clinical Technologies, LLC, Wallingford, CT) was introduced 4 years ago, much
concern was expressed for this obturation
material, ranging from how would it geometrically fill canals compared to guttapercha to whether it could provide a seal
equal to zinc oxide/eugenol (ZOE) or AH26 (epoxy resin root canal sealer). In the
meantime, the literature has been filled
with numerous peer-reviewed articles reporting on many aspects involving Resilon. This article addresses the concerns and
discusses some of the literature that has
been published on Resilon.
Resilon is a core obturation material alternative to gutta-percha and requires a
sealer to complete obturation of the canal
system. Several studies have used a methacrylate resin sealer, such as Epiphany™
(Pentron Clinical Technologies)—which
is also sold as RealSeal, (SybronEndo, Orange, CA) as a sealer system with Resilon
as the core obturation material. Another
product falling into this category of methacrylate sealers is EndoRez (Ultradent,
South Jordan, UT). Presently, alternatives
to Resilon available on the market consist
of resin-coated gutta-percha cones (EndoRez cones); Resilon is the only solid resin
cone being offered at this time.
LEAKAGE
Coronal leakage has been indicated as a
major determinant of endodontic success or failure. When the coronal portion
of the tooth is not sealed with a restorative
material that resists microleakage, the tooth
is at risk of bacterial infiltration and failure of the endodontic filling. Microleakage
continues to be a main reason for the failure of root canal therapy, where the challenge has been to achieve an adequate seal
between the internal tooth structure and
the main obturation material.
Coronal leakage for even a minimal amount of time may quickly lead to apical
migration of bacteria. Research has demonstrated that when exposed to artificial
and natural saliva for as little as 2 days, a
root canal filling will have leakage and bacterial contamination to the root apex.1
Studies using gutta-percha and various
sealers indicate that gutta-percha will consistently allow bacterial leakage. But use
of an adhesive sealer can significantly slow
or stop coronal-apical bacterial migration.2
Gutta-percha has limitations in its resistance to coronal leakage, which have been
overcome with the newer resin alternatives.
Although sealers can form close adhesion
to the root canal wall, none is able to bond
to the gutta-percha core material. Upon setting, shrinkage of the sealer allows the sealer to pull away from the gutta-percha core,
leaving a microgap through which bacteria may pass.3 In studies performed at the
University of North Carolina, the guttapercha test group demonstrated leakage in
80% of specimens regardless of the obturation technique or which sealer was used.4
A dog model was used to assess and
compare in vivo the efficacy of guttapercha and AH-26 sealer vs Resilon with
Epiphany™ (Pentron Clinical Technologies) primer and sealer-filled roots in
preventing apical periodontitis subsequent to coronal inoculation with oral
microorganisms. Mild inflammation
was reported in 82% of roots filled with
gutta-percha and AH-26 sealer, which
was statistically more than roots filled
with Resilon-obturated teeth (19%).
Resilon was also associated with signifi-
“Coronal leakage for even a minimal
amount of time may quickly lead
to apical migration of bacteria.”
cantly less apical periodontitis (82% vs
19%, McNemar paired analysis, P < .05),
which may be due to its superior resistance to coronal microleakage.5
As measured using dye penetration
methodology, the least apical leakage was
shown with Resilon.6,7 The differences in
leakage among the groups in this study
showed gutta-percha with AH-26 (2.4
mm, standard deviation [SD]: 1.87 mm),
gutta-percha with AH plus (2.1 mm, SD:
1.69 mm), and Resilon (1.7 mm, SD: 1.32
mm) were statistically significant (P <
.001). An alternative study, using the fluid transport method of teeth filled with
gutta-percha and AH-26, exhibited the
most leakage. The least leakage was seen
with Epiphany sealer and Resilon core material. The differences in leakage among the
groups were statistically significant (P <
.05).8 It was concluded that of the materials
tested under the conditions of this study,
Epiphany allowed the least leakage. This
was supported in an independent study
where two-way ANOVA analysis indicated
significantly less (P < .05) leakage using
Resilon with Epiphany sealer compared
to gutta-percha and AH-26 plus sealer.9
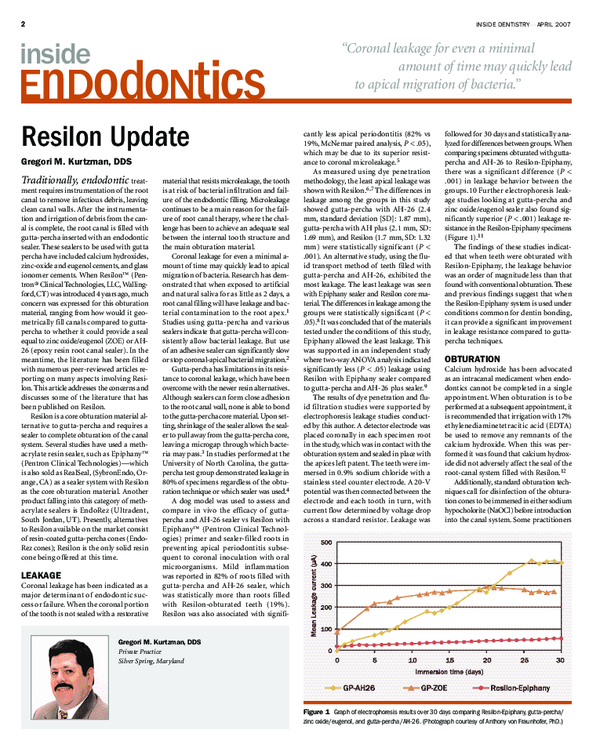
The results of dye penetration and fluid filtration studies were supported by
electrophoresis leakage studies conducted by this author. A detector electrode was
placed coronally in each specimen root
in the study, which was in contact with the
obturation system and sealed in place with
the apices left patent. The teeth were immersed in 0.9% sodium chloride with a
stainless steel counter electrode. A 20-V
potential was then connected between the
electrode and each tooth in turn, with
current flow determined by voltage drop
across a standard resistor. Leakage was
followed for 30 days and statistically analyzed for differences between groups. When
comparing specimens obturated with guttapercha and AH-26 to Resilon-Epiphany,
there was a significant difference (P <
.001) in leakage behavior between the
groups.10 Further electrophoresis leakage studies looking at gutta-percha and
zinc oxide/eugenol sealer also found significantly superior (P < .001) leakage resistance in the Resilon-Epiphany specimens
(Figure 1).11
The findings of these studies indicated that when teeth were obturated with
Resilon-Epiphany, the leakage behavior
was an order of magnitude less than that
found with conventional obturation. These
and previous findings suggest that when
the Resilon-Epiphany system is used under
conditions common for dentin bonding,
it can provide a significant improvement
in leakage resistance compared to guttapercha techniques.
OBTURATION
Calcium hydroxide has been advocated
as an intracanal medicament when endodontics cannot be completed in a single
appointment. When obturation is to be
performed at a subsequent appointment, it
is recommended that irrigation with 17%
ethylenediaminetetracitic acid (EDTA)
be used to remove any remnants of the
calcium hydroxide. When this was performed it was found that calcium hydroxide did not adversely affect the seal of the
root-canal system filled with Resilon.12
Additionally, standard obturation techniques call for disinfection of the obturation cones to be immersed in either sodium
hypocholorite (NaOCl) before introduction
into the canal system. Some practitioners
Gregori M. Kurtzman, DDS
Private Practice
Silver Spring, Maryland
Figure 1 Graph of electrophoresis results over 30 days comparing Resilon-Epiphany, gutta-percha/
zinc oxide/eugenol, and gutta-percha/AH-26. (Photograph courtesy of Anthony von Fraunhofer, PhD.)
�EnDodoNtics
INSIDE DENTISTRY—APRIL 2007
are alternatively using chlorhexidine. One
study found that a 1-minute immersion in
either solution did not show any significant
deterioration on the Resilon cone’s surface.13 However, since sodium hypochlorite affects dentin bonding, chlorhexidine
appears to a better choice as an immersion
agent for cones.
Resin sealers have been shown to have
potential setting issues in oxygen-rich environments (aerobic), but set well in an
anaerobic environment. It has been reported that Resilon sealer sets in 30 minutes in anaerobic environments, such as
those normally found in the canal following obturation. However, in the presence of air, Resilon took 1 week to set.14
The key is limiting oxygen in the canal system. Irrigants and lubricants that can liberate oxygen or inhabit resin setting (ie,
NaOCl, peroxides) in the canal may be
used but flushing out the tooth with a
neutralizing irrigant such as EDTA or
chlorhexidine will create an environment
that will allow setting in the allotted time.
Occasionally an endodontically treated
tooth will require retreatment. The concern
with resin obturation is that the progression of an instrument to working length
may be extremely difficult if not impossible due to the hardness associated with resins. Resilon obturation consists of a soft
core material (Resilon) with a methacrylic
resin sealer (Epiphany). Reports in the literature support the ability of progression of
a file through the Resilon-obturated canal,
permitting retreatment should it be necessary. Actually, Resilon was faster to remove than gutta-percha and resulted in
cleaner canal walls in the apical third of the
teeth obturated with Resilon when compared to gutta-percha.15,16
But what if a perforation occurs during
instrumentation? Can a resin obturation
still be used? A study reported by Maltezos and Glickman found that compared to
mineral trioxalate (MTA) there was no
statistical significance in bacterial leakage, but Resilon leaked significantly less
than Super-EBA™ (Bosworth, Skokie, IL)
when used as a apical filling material.17
Resilon may be a viable option as a retrograde filling material with good surgical
isolation and moisture control. With
regard to perforations, this offers indications that a good seal can be achieved
when exposed to the periodontal ligament
(PDL) space, and placement of MTA to
seal the perforation before obturation
may not be necessary.
FRACTURE RESISTANCE
Consideration of the structural aspects of
the tooth is critical in the long-term management of endodontically treated teeth.
Forces placed on the tooth during function
make the tooth vulnerable to fracture.18,19
Microfractures present prior to endodontic therapy may propagate under load,
leading to clinically significant cracks that
can eventually lead to the loss of the tooth.
The process of instrumentation itself may
weaken the tooth as the canals are enlarged
to properly shape and disinfect the root
canal system.20 Endodontically treated
teeth have been reported in the literature
to be more susceptible to fracture because
they possess reduced dentinal toughness,
lower water content, and deeper cavities.21
Additionally, the cervical aspect of the
tooth is subjected to significant compressive, tensile, and torsional forces during
function and bruxism, which can lead to
the fatigue of the weakened tooth structure, increasing its likelihood of fracture.22
Therefore, root canal treatment should include stabilization of the canal and coronal
aspect. A key element in this methodology
is obturation to assist in reinforcing the
remaining tooth structure.24-26
Studies have reported a significant increase in the fracture resistance of endodontically treated teeth. When restored
with a composite intracoronally with routine acid-etch and bonding procedures,
they can achieve strength levels almost
approximating those of intact teeth.27
Resilon, because of its intracanal bond,
has been shown to increase resistance to
tooth fracture when compared to obturations using gutta-percha and commonly
used sealers (ie, ZOE or AH-26).28 Micro
push-out studies comparing the bond
strength of Resilon to that of gutta-percha
found that mean bond strength to root canal dentin was significantly higher in the
Resilon/Epiphany group.29 The advantage to the use of resin obturation materials in the management of endodontically
treated teeth can result in a stronger, more
retentive restoration. This may be a significant benefit for teeth weakened by endodontic procedures.30 One study found
that canals obturated with Resilon/Epiphany obturation material increased the in
vitro resistance to fracture when compared with standard gutta-percha techniques. Resilon demonstrated a 25% increase
in root strength than gutta-percha samples.28 Indications are that resin obturation may provide enhanced resistance to
tooth fracture.31
3
Figure 2 Pretreatment radiograph of maxillary
right central incisor demonstrating a large
apical lesion. (Photograph courtesy of Dr.
Gilberto Debelian.)
Figure 3 Twenty-four month postendodontic
treatment with Resilon demonstrating complete
resolution of the apical lesion and sealer filling a
lateral canal. (Photograph courtesy of Dr.
Gilberto Debelian.)
Figure 4 Apical lesion present on lower right
second molar before endodontic treatment.
(Photograph courtesy of Dr. Dan Shalkey.)
Figure 5 Radiograph immediately following
Resilon obturation of lower right second molar
with apical lesion present. (Photograph courtesy
of Dr. Dan Shalkey.)
BIOCOMPATIBILITY
Cytotoxicity is an important consideration when selecting an obturation material. The obturation material should not
negatively affect the hosts cells found in
the PDL. The literature has repeatedly
reported gutta-percha as well tolerated
by host cells with no inflammatory reaction noted. Examination of fibroblast
cells found that Resilon was similar to
gutta-percha in how the cells reacted. But
the sealers used can lead to more reactions
as these have to undergo a setting reaction
and may potentially have a cytotoxic potential. Epiphany was found to be less cytotoxic than Grossman’s sealer (zinc oxideand eugenol-based) at both the 1- and
24-hour time periods. But Epiphany was
found to be more cytotoxic than Sealapex (SybronEndo), which is calcium
hydroxide-based, at the 1-hour time period but less cytotoxic at the 24-hour time
period.32
Figure 6 Twenty-nine month postendodontic treatment with Resilon demonstrating complete resolution of the apical lesion. (Photograph courtesy of Dr. Dan Shalkey.)
In evaluating intraosseous biocompatibility that may occur when sealer is
extruded past the apex, Sousa studied AH26, EndoRez, and Epiphany. After analyzing both time periods, the inflammatory
tissue reaction to EndoREZ was considered severe. In the AH Plus group, the reaction changed from severe to moderate,
while biological compatibility to Epiphany was observed with bone formation and
a slight to no inflammatory reaction. The
conclusion was that Epiphany root canal
sealer was the only material that presented intraosseous biocompatibility.33
CONCLUSION
Coronal leakage has been increasingly recognized as a major cause of endodontic failure. Multiple studies have demonstrated
that Resilon offers a significant improvement in leakage resistance compared to
gutta-percha and the traditional sealers
zinc oxide/eugenol or AH-26. Additionally,
resin obturation may strengthen the re-
�4
EnDodoNtics
INSIDE DENTISTRY—APRIL 2007
Figure 7 Large periapical lesion present following Resilon obturation. (Photograph courtesy
of Dr. Winfried Zeppenfeld.)
Figure 8 Ten-month postendodontic obturation demonstrating complete resolution of the
apical lesion. (Photograph courtesy of Dr.
Winfried Zeppenfeld.)
maining tooth structure, improving the
long-term prognosis for teeth obturated
with Resilon (Figure 2 through Figure 8).
For a more complete listing of the literature published regarding Resilon, please
refer to www.resilonresearch.com.
9. Stratton RK, Apicella MJ, Mines P. A fluid filtration comparison of gutta-percha versus
Resilon, a new soft resin endodontic obturation system. J Endod. 2006;32(7):642-645.
10. von Fraunhofer JA, Kurtzman GM, Norby CE.
Resin-based sealing of root canals in endodontic therapy. Gen Dent. 2006;54(4):
243-246.
11. Kurtzman GM, von Fraunhofer JA, Oliveira
DP. Endodontic Leakage Resistance of Fiber Obturators. Poster presentation AADR,
Orlando, FL 2006, #1443.
12. Wang CS, Debelian GJ, Teixeira FB. Effect
of intracanal medicament on the sealing
ability of root canals filled with Resilon. J
Endod. 2006;32(6):532-536. Epub 2006.
13. Isci S, Yoldas O, Dumani A. Effects of sodium hypochlorite and chlorhexidine solutions
on Resilon (synthetic polymer based root canal filling material) cones: an atomic force
microscopy study. J Endod. 2006;32(10):
967-969. Epub 2006.
14. Nielsen BA, Beeler WJ, Vy C, et al. Setting
times of Resilon and other sealers in aerobic and anaerobic environments. J Endod.
2006;32(2):130-132.
15. de Oliveira DP, Barbizam JV, Trope M, et al.
Comparison between gutta-percha and resilon removal using two different techniques
in endodontic retreatment. J Endod. 2006;
32(4):362-364.
16. Ezzie E, Fleury A, Solomon E, et al. Efficacy
of retreatment techniques for a resin-based
root canal obturation material. J Endod.
2006;32(4):341-344. Epub 2006.
17. Maltezos C, Glickman GN, Ezzo P, et al.
Comparison of the sealing of Resilon, Pro
Root MTA, and Super-EBA as root-end filling
materials: a bacterial leakage study. J
Endod. 2006;32(4):324-327. Epub 2006.
18. Gutmann JL. The dentin-root complex: Anatomic and biologic considerations in restoring endodontically treated teeth. J Prosthet
Dent.1992;67(4):458-467.
19. Lindauer PA, Campbell AD, Hicks ML, et al.
Vertical root fractures in curved roots under
DISCLOSURE
The author has received honoraria from
Pentron Clinical Technologies for lecturing and has participated in funded research on Resilon/Epiphany.
REFERENCES
1. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed obturated root canals. J Endod 1993;19(9):
458-461.
2. Britto LR, Grimaudo NJ, Vertucci FJ. Coronal microleakage assessed by polymicrobial markers. J Contemp Dent Pract. 2003;
4(3):1-10.
3. Teixeira FB, Teixeira EC, Thompson J, et al.
Dentinal bonding reaches the root canal
system. J Esthet Restor Dent. 2004;16(6):
348-354.
4. Shipper G, Orstavik D, Teixeira FB, et al. An
evaluation of microbial leakage in roots filled with a thermoplastic synthetic polymerbased root canal filling material (Resilon). J
Endod. 2004;30(5):342-347.
5. Shipper G, Teixeira FB, Arnold RR, et al.
Periapical inflammation after coronal microbial inoculation of dog roots filled with
gutta-percha or resilon. J Endod. 2005;31
(2):91-96.
6. Bodrumlu E, Tunga U. Apical leakage of
Resilon obturation material. J Contemp Dent
Pract. 2006;7(4):45-52.
7. Aptekar A, Ginnan K. Comparative analysis
of microleakage and seal for 2 obturation
materials: Resilon/Epiphany and gutta-percha. J Can Dent Assoc. 2006;72(3):245.
8. Tunga U, Bodrumlu E. Assessment of the
sealing ability of a new root canal obturation
material. J Endod. 2006;32(9):876-878.
Epub 2006.
simulated clinical conditions. J Endod.1989;
15(8):345-349.
20. Trope M, Ray HL Jr. Resistance to fracture
of endodontically treated roots. Oral Surg
Oral Med Oral Pathol. 1992;73(1):99-102.
21. Madison S, Wilcox LR. An evaluation of coronal microleakage in endodontically treated teeth. Part III. In vivo study. J Endod.
1988;14(9):455-458.
22. Caputo AA. Standlee JP. Biomechanics in
Clinical Dentistry. Berlin: Quintessence Publishing; 1987;21-27.
23. Craig RG, Farah JW. Stress analysis and design of single restorations and fixed bridges.
Oral Sci Rev. 1977;10:45-74.
24. Kanca J 3rd. Conservative resin restoration
of endodontically treated teeth. Quintessence Int. 1988;19(1):25-28.
25. Share J, Mishell Y, Nathanson D. Effect of
restorative material on resistance to fracture of tooth structure in vitro. J Dent Res.
1982;61(Special Issue #622):247.
26. Trope M, Maltz DO, Tronstad L. Resistance
to fracture of restored endodontically treated teeth. Endod Dent Traumatol. 1985;1(3):
108-111.
27. Hernandez R, Bader S, Boston D, Trope M. Resistance to fracture of endodontically treated premolars restored with new generation
dentin bonding systems. Int Endod J. 1994;
27(6):281-284.
28. Teixeira FB, Teixeira EC, Thompson JY, et al.
Fracture resistance of roots endodontically
treated with a new resin filling material. J
Am Dent Assoc. 2004;135(5):646-652.
29. Skidmore LJ, Berzins DW, Bahcall JK. An in
vitro comparison of the intraradicular dentin
bond strength of Resilon and gutta-percha.
J Endod. 2006;32(10):963-966. Epub 2006.
30. Teixeira FB. Ideal obturation using synthetic
root-filling systems: coronal sealing and
fracture resistance. Pract Proced Aesthet
Dent. 2006;18(3):S7-11.
31. Hafez et al. Regional Bond Strength of Epiphany/Resilon to Intraradicular Dentin. University of Iowa, Iowa City, IA. Abstract: #PR12,
J Endod. Vol. 32(3), March 2006.
32. Key JE, Rahemtulla FG, Eleazer PD. Cytotoxicity of a new root canal filling material on
human gingival fibroblasts. J Endod. 2006;
32(8):756-758. Epub 2006.
33. Sousa CJ, Montes CR, Pascon EA, et al.
Comparison of the intraosseous biocompatibility of AH Plus, EndoREZ, and Epiphany root canal sealers. J Endod. 2006;32
(7):656-662.
�
 Gregori Kurtzman
Gregori Kurtzman