Hindawi
Canadian Journal of Infectious Diseases and Medical Microbiology
Volume 2021, Article ID 4914371, 5 pages
https://doi.org/10.1155/2021/4914371
Research Article
Iranian Pediatric COVID-19 Epidemiology and
Clinical Characteristics
Shahnaz Armin ,1 Mohammadreza Mirkarimi ,2 Zahra Pourmoghaddas ,3
Marjan Tariverdi ,4 Azadeh Jafrasteh ,5 Noushin Marhamati ,1 Armin Shirvani ,6
Abdollah Karimi ,1 Sedigheh Rafiei Tabatabaei ,1 Roxana Mansour Ghanaei ,1
SeyedAlireza Fahimzad ,1 Fariba Shirvani ,1 and Seyedeh Mahsan Hoseini-Alfatemi 1
1
Pediatric Infections Research Center, Research Institute for Children’s Health, Shahid Beheshti University of Medical Sciences,
Tehran, Iran
2
Aboozar Children’s Medical Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
3
Pediatrics Infectious Disease Department, Isfahan University of Medical Sciences, Isfahan, Iran
4
Department of Pediatric, Clinical Research Development Center of Children Hospital,
Hormozgan University of Medical Sciences, Bandar Abbas, Iran
5
Department of Pediatrics, School of Medicine, Lorestan University of Medical Sciences, Khorramabad, Iran
6
Virtual School of Medical Education and Management, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence should be addressed to Seyedeh Mahsan Hoseini-Alfatemi; mahsan.hoseinialfatemi@gmail.com
Received 8 September 2021; Accepted 25 November 2021; Published 15 December 2021
Academic Editor: Louis Detolla
Copyright © 2021 Shahnaz Armin et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Background. Despite the worldwide spread of Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2), information
about the epidemiological and clinical patterns of this infection is still largely unknown in children. In addition, the prevalence of
this disease is still very high in some parts of the world, including Iran. Thus, this study aims to evaluate the epidemiological
features, laboratory and imaging findings, and the type of treatments in children with novel coronavirus 2019 (COVID-19).
Method. This study is conducted from March 2020–March 2021 by using the medical records of hospitalized confirmed COVID19 children younger than 18 years in five cities of Iran: Tehran, Ahwaz, Isfahan, Bandar-Abbas, and Khorramabad. In addition to
demographic and epidemiological data, we also studied clinical signs and treatments. Results. In total 278 confirmed COVID-19
children, the average age was 5.3 years, and 59.4%were boys. A total of 37.8% had an underlying disease, in which the most
common was a malignancy. The most common symptoms were fever and cough. In this group of pediatrics, some abnormal
laboratory findings have been seen. GGO (Ground-Glass Opacity) had been diagnosed in 58.6% of children. 3.6% needed oxygen
therapy with ventilators, and 83.09% had received antibiotic treatments with the majority of ceftriaxone. Also, 10% had got
steroids. In this study, the mortality rate was 4.3%. Conclusion. In this study, most of the children who died had an underlying
disease, so timely care and action is important in them. Most children admitted to our study received antibiotics and were
prescribed antivirals and steroids for a smaller number. Also, a small number of children received oxygen therapy, most of whom
were in the age group of 1 to 5 years.
1. Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe
acute respiratory syndrome coronavirus-2 (SARS-CoV-2).
Because of the intensity and alarming level of spread, the
World Health Organization (WHO) deemed it a pandemic
[1]. The first pandemic infection to occur due to a coronavirus [2], SARS-CoV-2, is a factor that effects all age
groups.
COVID-19 has a low incidence of severe cases among
children. Children have a milder clinical course than adults
[3–6]. Children and adults have different levels of immune
�Canadian Journal of Infectious Diseases and Medical Microbiology
maturity, which may be the reason for differences in the
prevalence and type of clinical manifestations of COVID-19
[7]. However, it is also important to note that even mild
COVID-19 can cause transmission [8]. According to the
work of Gandhi et al., asymptomatic transmission is the
Achilles’ heel of this pandemic [9].
In other words, children can cause cluster propagation in
the home environment [10]. Furthermore, children with
gastrointestinal symptoms can transmit the virus through
their feces for weeks, which is dangerous in some places such
as kindergartens or elementary schools [11–13].
In addition to acute COVID-19 in children, there are
several reports of multisystemic involvement, which complicates the diagnosis and management of this disease in
pediatrics.
First cases of COVID-19 were observed in Iran in
January 2020, but the country began reporting cases to the
WHO on February 2020 [14]. Since then, the disease has
spread rapidly across the country, infecting many children
[5]. The purpose of this study was to determine the clinical
presentation and treatment pattern of COVID-19 among
children admitted to 5 major cities in Iran.
2. Method
We conducted a retrospective, cross-sectional, multicenter
study from March 2020 to March 2021 in several Iranian
cities (Tehran, Ahwaz, Isfahan, Bandar-Abbas, and Khorramabad). During the study period, all children hospitalized
with confirmed SARS-CoV-2 infection in one of the participating centers were included. Data were extracted from
medical records of children younger than 18 years diagnosed
with confirmed cases of COVID-19 with positive real-time
reverse transcription polymerase chain reaction (RT-PCR)
results on nasopharyngeal samples. Besides demographic
and epidemiological data, we also studied clinical symptoms
and treatments. Data were collected from medical forms and
records by a pediatrician. No written consent has been
obtained from the patients as there are no patient identifiable
data included in this research.
The research ethics committee of Shahid Beheshti
University of Medical Sciences approved the study (Ethical
code: IR.SBMU.RICH.REC.1400.007).
3. Result
The average age of the 278 children and adolescents hospitalized with COVID-19 was 5.3 years. Of the 278 patients,
56 (20.1%) were under one year of age, 95 (34.2%) were
between 1 and 5 years of age, and 127 (45.7%) were over five
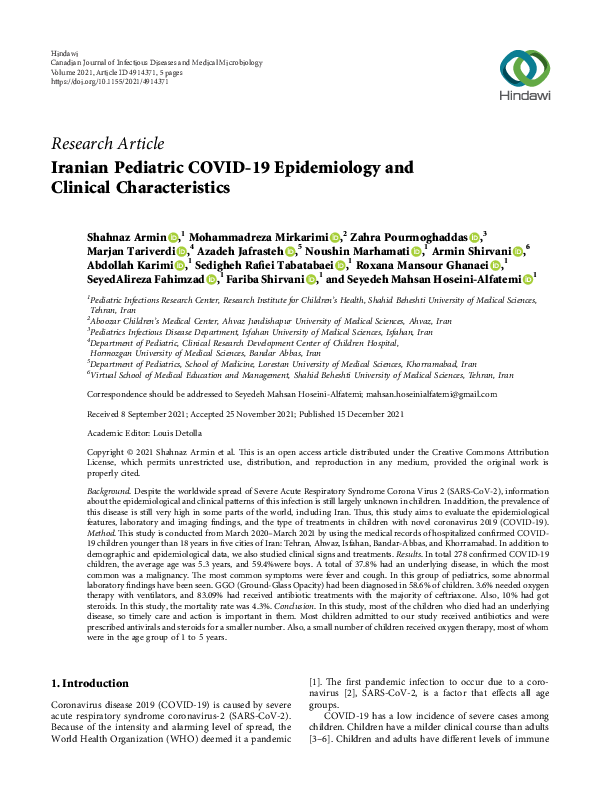
years of age. There were 59.4% boys among the cases. Results
of the study, which include general information and clinical
signs, are divided into 3 age groups (under 1 year, 1 to 5
years, and over 5 years) in Figure 1.
A total of 37.8% of children hospitalized had an underlying disease. By far, the most common condition was
malignancy (10%), followed by diabetes (5%). We estimate
that the mortality rate was 4.3% (12 patients) as 8 of them
had an underlying disease, and half of the dead were over 5
90
80
70
60
50
40
30
20
10
0
Abnormal Chest x ray
Abnormal Lungct scan
Steroid
Heparin
IVIG
Hydroxychloroquine
Ventilator
Proteinuria
Hematuria
Abnormal GCS
Convulsions
Cyanosis
Retraction
Hypotension
Tachypnea
Skin rash
Vomiting
Diarrhea
Redness of the eyes
Runny nose
Sneeze
Cough
Chill
Fever
Contact History
Underlying Disease
Female
2
<1
1_5
>5
Figure 1: General information and clinical symptoms of pediatric
patients with confirmed COVID-19 in 3 age groups (<1, 1–5, >5).
years of age. Approximately 40% of our study population
was exposed to an indicator case or an adult with suspected
SARS-CoV-2 infection. 3.6% of hospitalized children needed
oxygen therapy with ventilators, most of whom were 1 to 5
years old.
Children with COVID-19 tend to experience fewer
symptoms than adults. Fever was the most common
symptom (77.3%), according to the information obtained.
Cough was another symptom (43.8%). Both diarrhea and
vomiting were present in 22.3% and 30.3% of cases, respectively. In 20.9% of cases, tachypnea was reported.
Infection was also associated with sneezing and runny
nose in 3.2% and 6.5% of children, respectively. A skin
rash was reported in 11.2% of children hospitalized with
COVID-19 and red eyes in 7.2%. The mean O2 level was
93.6% (with a minimum of 68 and a maximum of 99%). O2
was below 93% in 22.6% of cases. Frequently, children
hospitalized for illnesses have elevated inflammatory
markers, such as ESR, CRP, and liver enzyme. The mean
initial CRP in the under one age group was lower than in
other age groups. BUN and Cr were abnormal in 13.6%
and 8% patients, respectively. In our research, based on
the division of LDH into two groups above 500 and above
1000, patients were included in 56.88 and 8.3%, respectively. Abnormal AST and ALT were found in 37.17% and
15.03%, respectively. Laboratory findings are presented in
Table 1. In our review, leukocytosis had been reported in
24.5% of the patients, while 9.33% of our pediatrics had
leukopenia. Different age groups have reported lymphopenia: 44% under one year of age, 28.04% in 1 to 5 years,
and 34.25% in people 5 years and older. GGO has been
diagnosed in 58.6% of children with lung involvement,
mainly in RLL and LLL.
A total of 231 patients (83.09%) were treated with antibiotics, with the most common drug used being ceftriaxone
(161), followed by vancomycin (67), meropenem (48), and
azithromycin (42), given as a two- or three-medicine regimen. There were also 100 patients given antivirals (35.97%),
most of whom were given Kaletra (52 patients) and atazanavir (22 patients). Also 10% had steroid treatments.
�Canadian Journal of Infectious Diseases and Medical Microbiology
Table 1: Laboratory findings of the hospitalized COVID-19 pediatric patients.
Laboratory data
Number
Minimum
Maximum
Mean
137
68
99
93.66
O2sat in room temperature
WBC
257
120
43600
8979.96
ALC
242
86
16947
3063.30
Hb
257
4.50
17.70
11.12
PLT
256
6000
838000
271807.46
CRP
208
0
178
19.28
ESR
226
1
210.7
26.90
BS
201
1
891.5
124.93
BUN
249
3
1542
24.11
Cr
249
0.10
54
1.04
SGOT
155
5
232
42.62
SGPT
152
3
1478
36.53
ALK.P
103
93
1822
477.08
PT
78
10
32
13.70
PTT
74
12.20
70
32.74
INR
77
0.78
1.50
1.07
LDH
167
6.90
2697
623.62
Ferritin
65
4
1714
311.25
Fibrinogen
20
67
1000
330.30
CPK
113
16
2126
155.53
D.dimer
45
0.09
3327
581.64
Troponin
53
0
28.80
5.03
PH
81
6.91
7.70
7.34
PCO2
81
14
98
35.53
HCO3
80
5.70
27.70
19.35
4. Discussion
In Wenjun et al.’s retrospective study, the median age was
6.2 years [15], while in ours, the mean age was 5.3 years. The
study showed that boys made up the majority (59.4%), as in
other studies including the work of Dong et al. (56.6%) [5].
Hua et al. in an epidemiological study reported the mean age
in children was 8.16 years (in the range of 3.66 months–14
years) and 60.5% were male [16].
In the study by Tezer and Bedir Demirdağ, among 345
confirmed children, 23% had underlying diseases and the
most common ones were chronic pulmonary disease
(counting asthma), cardiovascular disease, and immunosuppression (caused by cancer, chemotherapy, etc.) [17]. In
addition, in Kompaniyets et al.’s cross-sectional study,
among 43,465 patients with COVID-19 pediatrics, 28.7%
had underlying medical conditions, mostly asthma, neurodevelopmental disorders, anxiety-related disorders, depressive disorders, and obesity [18]. Also, we found that
37.8% of our hospitalized children had an underlying disease
with the most common being malignancy followed by a
chronic disease such as diabetes. The differences likely arise
from the type of underlying conditions that researchers are
searching for.
Hoang et al.’s study had reported 0·09% deaths among
the COVID-19 children [19], while by our results, the estimated mortality rate was below 5 percent.
According to Chang et al.’s systematic literature (with
last updates on 15 March 2020), as well as Ansel et al.’s
systematic search (with last searched 14 May 2020) and
Hoseinyazdi et al.’s pediatric study in Shiraz (March–May
2020), like ours, fever and cough were the most common
clinical symptoms [19–21]. Although Chang et al.’s study
3
Std. deviation
5.379
5415.383
2527.806
2.068
144975.231
27.452
27.78
96.95
110.221
3.584
31.750
119.919
299.025
4.114
9.504
0.139
387.434
386.216
196.052
230.546
776.268
6.903
0.143
12.199
4.323
reported few gastrointestinal symptoms (12%) [20], in our
study, diarrhea and vomiting were reported in 22.3% and
30.3% of cases, respectively. Possibly because we studied at a
different time and place, the predominant virus strain may
have been different.
Two systematic reviews have shown that most children
with COVID-19 have a normal WBC count and the most
common abnormality is leukopenia [22, 23]; this variance
may be due to differences in age group or severity of the
infection or virus.
In our review, 24.5% of the patients had leukocytosis,
while only 9.33% had shown leukopenia. In a systematic
review by Henry et al., leukocyte counts were normal in most
children, and lymphopenia was present in only 3%, none of
whom had severe disease [24].
In our investigations, out of 240 patients, 34.16% had
been shown with lymphopenia and only 2% had lymphocytosis. Based on Hoseinyazdi et al.’s pediatric study in
Namazi and Ali-Asghar Hospitals, lymphocytosis has been
shown in severe cases [21]. Additionally, another study by
Du et al. in Shandong Province in China found
increased lymphocyte counts in children compared to adults
[15]. According to Kosmeri et al., lymphocytosis was the
most common findings in neonates and infants with
COVID-19. Moreover, anemia and thrombocytopenia were
rarely seen in COVID-19 children [25].
In Hoseinyazdi’s study, CRP levels were normal in patients under two years of age, whereas they were significantly
higher in those aged over 3 years [21]. Also, in our study, the
mean range of initial CRP was lower in the group under 1
years of age than that of those over this age.
Abnormal levels of LDH were seen in fifty percent of
children with COVID-19 in the study by Du et al. and also
�4
Canadian Journal of Infectious Diseases and Medical Microbiology
showed that positive LDH levels were significantly higher in
children than in adults [15]. In ours, more than half of the
study population had an LDH above 500 and less than a
tenth had it above 1000. Furthermore 37.17% and 15.03%
had abnormal AST and ALT in that order; while in Esmaeili
et al.’s retrospective study, 27.8% and 38.9% of cases showed
abnormally high ALT and AST levels, respectively [26].
According to an Italian report from an emergency department for children, 4% of children had oxygen saturation
below 95%. All of these patients also had imaging evidence of
lung involvement [4]. In our observations, the mean
O2saturation level was 93.66% and O2sat was below 93% in
22.6% of reported cases. Since our data pertain to sick patients admitted to hospitals, the figure is higher than Italian
rates, even though most Italian patients had not been in a
bad situation.
The most common radiographic finding in Chang et al.’s
investigations was ground-glass opacities (48%) [20]. In
Samy and Khalaf’s investigations, 44 (83%) patients had
normal CT and only 9 patients presented lung opacities in
which 5 cases showed consolidation and 2 cases were with
GGO, while in another 2 cases, consolidation with GGO was
noted. The most involved lobes were the right and left lower
lobes [27]. In our study, GGO was the most commonly
reported finding in 58.6% of children with pulmonary involvement (in RLL and LLL).
In one of the observational studies in Wuhan, China, six
of the eight patients received high-flow oxygen therapy and
two critically ill patients were mechanically ventilated.
Antiviral therapies (Verazole, oseltamivir, and interferon)
were administered to all patients. Antibiotics (in 5/8), traditional Chinese medicine (in 4/8), intravenous immunoglobulins (in 4/8), and glucocorticoids (in 5/8) were also
used according to the children’s condition [28].
In our education, a total of 231 patients (83.09%) received antibiotic treatment, the majority of which were
ceftriaxone. vancomycin, meropenem, and azithromycin; on
the other hand, they were also commonly administered in
combination with each other. A total of 100 patients were
also prescribed antiviral medicines, the majority of whom
took Kaletra or atazanavir based on national protocols at the
time of the study. In addition, about 10% of our patients
received steroid medication. Fewer than 4% of hospitalized
children required respiratory oxygen therapy, most of whom
were between the ages of 1 and 5 years.
Based on a retrospective study by Zhang et al., ribavirin
was given to 44% of patients. 85% had received antibiotic
therapy. Corticosteroids (15%) and supportive oxygen inhalation therapy (9%) were also used [29].
5. Conclusions
Among the children who died in this study, the majority had
the comorbidities. In order to protect children with underlying diseases, care and isolation must be provided in a
timely manner. Cough and fever were the most common
clinical symptoms. Leukocyte changes, especially lymphopenia, have been reported less frequently in children under 1
year of age with COVID-19, possibly due to their immature
immune systems and ACE2 expression. Most patients
received antibiotics, and relatively fewer antivirals and
steroids were administered. Also, oxygen therapy was used
to a much lesser extent in our patients, most of whom were
in the age group of 1–5 years. Therefore, paying attention to
the abovementioned results can help us reduce the prevalence of this disease.
Data Availability
The authors declare the data used to support the findings of
this study are available from the corresponding author upon
request.
Additional Points
Because this is a retrospective study that collected information from medical records in different cities, some data
and variables were not available; in addition, it was not
possible to complete it (for example, some tests were not
performed in all patients).
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1] E. Livingston and K. Bucher, “Coronavirus disease 2019
(COVID-19) in Italy,” Journal of the American Medical Association, vol. 323, no. 14, p. 1335, 2020.
[2] WHO, Coronavirus Disease (COVID-19), WHO, Geneva,
Switzerland, 2020.
[3] X. Lu, L. Zhang, H. Du et al., “SARS-CoV-2 infection in
children,” New England Journal of Medicine, vol. 382, no. 17,
pp. 1663–1665, 2020.
[4] N. Parri, M. Lenge, and D. Buonsenso, “Children with covid19 in pediatric emergency departments in Italy,” New England
Journal of Medicine, vol. 383, no. 2, pp. 187–190, 2020.
[5] Y. Dong, X. Mo, Y. Hu et al., “Epidemiology of COVID-19
among children in China,” Pediatrics, vol. 145, no. 6, 2020.
[6] CDC COVID-19 Response Team, “Coronavirus disease 2019
in children—United States, february 12–april 2, 2020,”
Morbidity & Mortality Weekly Report, vol. 69, pp. 422–426,
2020.
[7] D. Raoult, A. Zumla, F. Locatelli, G. Ippolito, and G. Kroemer,
“Coronavirus infections: epidemiological, clinical and immunological features and hypotheses,” Cell Stress, vol. 4, no. 4,
pp. 66–75, 2020.
[8] W.-j. Guan, Z.-y. Ni, Y. Hu et al., “Clinical characteristics of
coronavirus disease 2019 in China,” New England Journal of
Medicine, vol. 382, no. 18, pp. 1708–1720, 2020.
[9] M. Gandhi, D. S. Yokoe, and D. V. Havlir, “Asymptomatic
transmission, the Achilles’ heel of current strategies to control
covid-19,” New England Journal of Medicine, vol. 382, no. 22,
pp. 2158–2160, 2020.
[10] “Questions and answers on COVID-19: children aged 1–18
years and the role of school settings,” 2020, https://www.ecdc.
europa.eu/en/covid-19/questions-answers/questionsanswers-school-transmission.
[11] Y. Xu, X. Li, B. Zhu et al., “Characteristics of pediatric SARSCoV-2 infection and potential evidence for persistent fecal
�Canadian Journal of Infectious Diseases and Medical Microbiology
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
[20]
[21]
[22]
[23]
[24]
[25]
[26]
[27]
[28]
viral shedding,” Nature Medicine, vol. 26, no. 4, pp. 502–505,
2020.
X. Ma, L. Su, Y. Zhang, X. Zhang, Z. Gai, and Z. Zhang, “Do
children need a longer time to shed SARS-CoV-2 in stool than
adults?” Journal of Microbiology, Immunology, and Infection,
vol. 53, no. 3, pp. 373–376, 2020.
Y.-H. Xing, W. Ni, Q. Wu et al., “Prolonged viral shedding in
feces of pediatric patients with coronavirus disease 2019,”
Journal of Microbiology, Immunology, and Infection, vol. 53,
no. 3, pp. 473–480, 2020.
World Health Organization, Coronavirus Disease (COVID2019) Situation reportsWorld Health Organization, Geneva,
Switzerland, 2020.
W. Du, J. Yu, H. Wang et al., “Clinical characteristics of
COVID-19 in children compared with adults in Shandong
Province, China,” Infection, vol. 48, no. 3, pp. 445–452, 2020.
C. Z. Hua, Z. P. Miao, J. S. Zheng et al., “Epidemiological
features and viral shedding in children with SARS-CoV-2
infection,” Journal of Medical Virology, vol. 92, no. 11,
pp. 2804–2812, 2020.
H. Tezer and T. Bedir Demirdağ, “Novel coronavirus disease
(COVID-19) in children,” Turkish Journal of Medical Sciences,
vol. 50, no. SI-1, pp. 592–603, 2020.
L. Kompaniyets, N. T. Agathis, J. M. Nelson et al., “Underlying medical conditions associated with severe COVID-19
illness among children,” JAMA Network Open, vol. 4, no. 6,
pp. e2111182–e, 2021.
A. Hoang, K. Chorath, A. Moreira et al., “COVID-19 in 7780
pediatric patients: a systematic review,” EClinicalMedicine,
vol. 24, Article ID 100433, 2020.
T.-H. Chang, J.-L. Wu, and L.-Y. Chang, “Clinical characteristics and diagnostic challenges of pediatric COVID-19: a
systematic review and meta-analysis,” Journal of the Formosan
Medical Association, vol. 119, no. 5, pp. 982–989, 2020.
M. Hoseinyazdi, S. Esmaeilian, R. Jahankhah et al., “Clinical,
laboratory, and chest CT features of severe versus non-severe
pediatric patients with COVID-19 infection among different
age groups,” BMC Infectious Diseases, vol. 21, no. 1,
pp. 560–612, 2021.
J. Meena, J. Yadav, L. Saini, A. Yadav, and J. Kumar, “Clinical
features and outcome of SARS-CoV-2 infection in children: a
systematic review and meta-analysis,” Indian Pediatrics,
vol. 57, no. 9, pp. 820–826, 2020.
N. A. Patel, “Pediatric COVID-19: systematic review of the
literature,” American Journal of Otolaryngology, vol. 41, no. 5,
Article ID 102573, 2020.
B. M. Henry, G. Lippi, and M. Plebani, “Laboratory abnormalities in children with novel coronavirus disease 2019,”
Clinical Chemistry and Laboratory Medicine, vol. 58, no. 7,
pp. 1135–1138, 2020.
C. Kosmeri, E. Koumpis, S. Tsabouri, E. Siomou, and
A. Makis, “Hematological manifestations of SARS-CoV-2 in
children,” Pediatric Blood & Cancer, vol. 67, no. 12, Article ID
e28745, 2020.
M. Esmaeili Dooki, S. Mehrabani, H. Sorkhi et al., “COVID-19
and digestive system in children: a retrospective study,” Archives of Iranian Medicine, vol. 23, no. 11, pp. 782–786, 2020.
M. Samy and L. M. Khalaf, “Chest CT features of COVID-19
pediatric patients presented with upper respiratory symptoms,” Egyptian Journal of Radiology and Nuclear Medicine,
vol. 52, no. 1, pp. 1–5, 2021.
D. Sun, H. Li, X.-X. Lu et al., “Clinical features of severe
pediatric patients with coronavirus disease 2019 in Wuhan: a
5
single center’s observational study,” World Journal of Pediatrics, vol. 16, p. 1, 2020.
[29] C. Zhang, J. Gu, Q. Chen et al., “Clinical and epidemiological
characteristics of pediatric SARS-CoV-2 infections in China: a
multicenter case series,” PLoS Medicine, vol. 17, no. 6, Article
ID e1003130, 2020.
�
 zahra pourmoghaddas
zahra pourmoghaddas