JP2022530963A - Inhaler system - Google Patents
Inhaler system Download PDFInfo
- Publication number
- JP2022530963A JP2022530963A JP2021564397A JP2021564397A JP2022530963A JP 2022530963 A JP2022530963 A JP 2022530963A JP 2021564397 A JP2021564397 A JP 2021564397A JP 2021564397 A JP2021564397 A JP 2021564397A JP 2022530963 A JP2022530963 A JP 2022530963A
- Authority
- JP
- Japan
- Prior art keywords
- inhalation
- probability
- exacerbation
- emergency
- subject
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Granted
Links
Images























Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/009—Inhalators using medicine packages with incorporated spraying means, e.g. aerosol cans
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/08—Measuring devices for evaluating the respiratory organs
- A61B5/0826—Detecting or evaluating apnoea events
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/08—Measuring devices for evaluating the respiratory organs
- A61B5/087—Measuring breath flow
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/48—Other medical applications
- A61B5/4836—Diagnosis combined with treatment in closed-loop systems or methods
- A61B5/4839—Diagnosis combined with treatment in closed-loop systems or methods combined with drug delivery
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/48—Other medical applications
- A61B5/4842—Monitoring progression or stage of a disease
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/48—Other medical applications
- A61B5/4848—Monitoring or testing the effects of treatment, e.g. of medication
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/72—Signal processing specially adapted for physiological signals or for diagnostic purposes
- A61B5/7271—Specific aspects of physiological measurement analysis
- A61B5/7275—Determining trends in physiological measurement data; Predicting development of a medical condition based on physiological measurements, e.g. determining a risk factor
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/13—Amines
- A61K31/135—Amines having aromatic rings, e.g. ketamine, nortriptyline
- A61K31/138—Aryloxyalkylamines, e.g. propranolol, tamoxifen, phenoxybenzamine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/007—Pulmonary tract; Aromatherapy
- A61K9/0073—Sprays or powders for inhalation; Aerolised or nebulised preparations generated by other means than thermal energy
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0001—Details of inhalators; Constructional features thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0001—Details of inhalators; Constructional features thereof
- A61M15/0021—Mouthpieces therefor
- A61M15/0025—Mouthpieces therefor with caps
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0028—Inhalators using prepacked dosages, one for each application, e.g. capsules to be perforated or broken-up
- A61M15/003—Inhalators using prepacked dosages, one for each application, e.g. capsules to be perforated or broken-up using capsules, e.g. to be perforated or broken-up
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0065—Inhalators with dosage or measuring devices
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0091—Inhalators mechanically breath-triggered
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0091—Inhalators mechanically breath-triggered
- A61M15/0093—Inhalators mechanically breath-triggered without arming or cocking, e.g. acting directly on the delivery valve
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M16/00—Devices for influencing the respiratory system of patients by gas treatment, e.g. ventilators; Tracheal tubes
- A61M16/0003—Accessories therefor, e.g. sensors, vibrators, negative pressure
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P11/00—Drugs for disorders of the respiratory system
- A61P11/06—Antiasthmatics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P11/00—Drugs for disorders of the respiratory system
- A61P11/08—Bronchodilators
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/24—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against cytokines, lymphokines or interferons
- C07K16/244—Interleukins [IL]
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/24—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against cytokines, lymphokines or interferons
- C07K16/244—Interleukins [IL]
- C07K16/247—IL-4
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2866—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against receptors for cytokines, lymphokines, interferons
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/42—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against immunoglobulins
- C07K16/4283—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against immunoglobulins against an allotypic or isotypic determinant on Ig
- C07K16/4291—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against immunoglobulins against an allotypic or isotypic determinant on Ig against IgE
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H20/00—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance
- G16H20/10—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance relating to drugs or medications, e.g. for ensuring correct administration to patients
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H20/00—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance
- G16H20/10—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance relating to drugs or medications, e.g. for ensuring correct administration to patients
- G16H20/13—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance relating to drugs or medications, e.g. for ensuring correct administration to patients delivered from dispensers
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H40/00—ICT specially adapted for the management or administration of healthcare resources or facilities; ICT specially adapted for the management or operation of medical equipment or devices
- G16H40/60—ICT specially adapted for the management or administration of healthcare resources or facilities; ICT specially adapted for the management or operation of medical equipment or devices for the operation of medical equipment or devices
- G16H40/63—ICT specially adapted for the management or administration of healthcare resources or facilities; ICT specially adapted for the management or operation of medical equipment or devices for the operation of medical equipment or devices for local operation
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/20—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for computer-aided diagnosis, e.g. based on medical expert systems
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/30—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for calculating health indices; for individual health risk assessment
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/70—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for mining of medical data, e.g. analysing previous cases of other patients
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/74—Details of notification to user or communication with user or patient; User input means
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M11/00—Sprayers or atomisers specially adapted for therapeutic purposes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0001—Details of inhalators; Constructional features thereof
- A61M15/0021—Mouthpieces therefor
- A61M15/0025—Mouthpieces therefor with caps
- A61M15/0026—Hinged caps
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0065—Inhalators with dosage or measuring devices
- A61M15/0068—Indicating or counting the number of dispensed doses or of remaining doses
- A61M15/007—Mechanical counters
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M15/00—Inhalators
- A61M15/0065—Inhalators with dosage or measuring devices
- A61M15/0068—Indicating or counting the number of dispensed doses or of remaining doses
- A61M15/008—Electronic counters
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M16/00—Devices for influencing the respiratory system of patients by gas treatment, e.g. ventilators; Tracheal tubes
- A61M16/0003—Accessories therefor, e.g. sensors, vibrators, negative pressure
- A61M2016/0015—Accessories therefor, e.g. sensors, vibrators, negative pressure inhalation detectors
- A61M2016/0018—Accessories therefor, e.g. sensors, vibrators, negative pressure inhalation detectors electrical
- A61M2016/0021—Accessories therefor, e.g. sensors, vibrators, negative pressure inhalation detectors electrical with a proportional output signal, e.g. from a thermistor
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M16/00—Devices for influencing the respiratory system of patients by gas treatment, e.g. ventilators; Tracheal tubes
- A61M16/0003—Accessories therefor, e.g. sensors, vibrators, negative pressure
- A61M2016/0015—Accessories therefor, e.g. sensors, vibrators, negative pressure inhalation detectors
- A61M2016/0018—Accessories therefor, e.g. sensors, vibrators, negative pressure inhalation detectors electrical
- A61M2016/0024—Accessories therefor, e.g. sensors, vibrators, negative pressure inhalation detectors electrical with an on-off output signal, e.g. from a switch
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M16/00—Devices for influencing the respiratory system of patients by gas treatment, e.g. ventilators; Tracheal tubes
- A61M16/0003—Accessories therefor, e.g. sensors, vibrators, negative pressure
- A61M2016/0027—Accessories therefor, e.g. sensors, vibrators, negative pressure pressure meter
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M16/00—Devices for influencing the respiratory system of patients by gas treatment, e.g. ventilators; Tracheal tubes
- A61M16/0003—Accessories therefor, e.g. sensors, vibrators, negative pressure
- A61M2016/003—Accessories therefor, e.g. sensors, vibrators, negative pressure with a flowmeter
- A61M2016/0033—Accessories therefor, e.g. sensors, vibrators, negative pressure with a flowmeter electrical
- A61M2016/0039—Accessories therefor, e.g. sensors, vibrators, negative pressure with a flowmeter electrical in the inspiratory circuit
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2202/00—Special media to be introduced, removed or treated
- A61M2202/06—Solids
- A61M2202/064—Powder
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/05—General characteristics of the apparatus combined with other kinds of therapy
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/18—General characteristics of the apparatus with alarm
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3306—Optical measuring means
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3327—Measuring
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3331—Pressure; Flow
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3331—Pressure; Flow
- A61M2205/3334—Measuring or controlling the flow rate
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3331—Pressure; Flow
- A61M2205/3358—Measuring barometric pressure, e.g. for compensation
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3368—Temperature
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/33—Controlling, regulating or measuring
- A61M2205/3375—Acoustical, e.g. ultrasonic, measuring means
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/35—Communication
- A61M2205/3546—Range
- A61M2205/3553—Range remote, e.g. between patient's home and doctor's office
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/35—Communication
- A61M2205/3546—Range
- A61M2205/3561—Range local, e.g. within room or hospital
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/35—Communication
- A61M2205/3576—Communication with non implanted data transmission devices, e.g. using external transmitter or receiver
- A61M2205/3584—Communication with non implanted data transmission devices, e.g. using external transmitter or receiver using modem, internet or bluetooth
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/35—Communication
- A61M2205/3576—Communication with non implanted data transmission devices, e.g. using external transmitter or receiver
- A61M2205/3592—Communication with non implanted data transmission devices, e.g. using external transmitter or receiver using telemetric means, e.g. radio or optical transmission
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/50—General characteristics of the apparatus with microprocessors or computers
- A61M2205/502—User interfaces, e.g. screens or keyboards
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/50—General characteristics of the apparatus with microprocessors or computers
- A61M2205/502—User interfaces, e.g. screens or keyboards
- A61M2205/505—Touch-screens; Virtual keyboard or keypads; Virtual buttons; Soft keys; Mouse touches
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/50—General characteristics of the apparatus with microprocessors or computers
- A61M2205/52—General characteristics of the apparatus with microprocessors or computers with memories providing a history of measured variating parameters of apparatus or patient
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/58—Means for facilitating use, e.g. by people with impaired vision
- A61M2205/581—Means for facilitating use, e.g. by people with impaired vision by audible feedback
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/58—Means for facilitating use, e.g. by people with impaired vision
- A61M2205/583—Means for facilitating use, e.g. by people with impaired vision by visual feedback
- A61M2205/584—Means for facilitating use, e.g. by people with impaired vision by visual feedback having a color code
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2205/00—General characteristics of the apparatus
- A61M2205/82—Internal energy supply devices
- A61M2205/8206—Internal energy supply devices battery-operated
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2230/00—Measuring parameters of the user
- A61M2230/30—Blood pressure
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M2230/00—Measuring parameters of the user
- A61M2230/40—Respiratory characteristics
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/20—Immunoglobulins specific features characterized by taxonomic origin
- C07K2317/21—Immunoglobulins specific features characterized by taxonomic origin from primates, e.g. man
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/20—Immunoglobulins specific features characterized by taxonomic origin
- C07K2317/24—Immunoglobulins specific features characterized by taxonomic origin containing regions, domains or residues from different species, e.g. chimeric, humanized or veneered
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/50—Immunoglobulins specific features characterized by immunoglobulin fragments
- C07K2317/52—Constant or Fc region; Isotype
Landscapes
- Health & Medical Sciences (AREA)
- Engineering & Computer Science (AREA)
- Life Sciences & Earth Sciences (AREA)
- Public Health (AREA)
- General Health & Medical Sciences (AREA)
- Biomedical Technology (AREA)
- Veterinary Medicine (AREA)
- Animal Behavior & Ethology (AREA)
- Medical Informatics (AREA)
- Chemical & Material Sciences (AREA)
- Pulmonology (AREA)
- Heart & Thoracic Surgery (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Biophysics (AREA)
- Medicinal Chemistry (AREA)
- Pathology (AREA)
- Epidemiology (AREA)
- Molecular Biology (AREA)
- Organic Chemistry (AREA)
- Hematology (AREA)
- Anesthesiology (AREA)
- Primary Health Care (AREA)
- Surgery (AREA)
- Physics & Mathematics (AREA)
- Immunology (AREA)
- Data Mining & Analysis (AREA)
- Pharmacology & Pharmacy (AREA)
- Physiology (AREA)
- Databases & Information Systems (AREA)
- Genetics & Genomics (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Biochemistry (AREA)
- Chemical Kinetics & Catalysis (AREA)
- General Chemical & Material Sciences (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Artificial Intelligence (AREA)
- Computer Vision & Pattern Recognition (AREA)
- Psychiatry (AREA)
- Signal Processing (AREA)
- General Business, Economics & Management (AREA)
Abstract
対象者における喘息の増悪の確率を計算するシステム(10)が提供される。システムは、対象者に救急薬を投与するための第1の吸入器(100)を備える。救急薬は、例えば薬剤の吸入時に気管支または細気管支を迅速に拡張することによって、対象者の切迫した呼吸器疾患を治療するのに適している。第1の吸入器は、対象者が第1の吸入器を用いて行った救急吸入の回数を計測するように構成された使用検出システム(12B)を有する。システムは、選択的に、定期吸入の間に対象者に維持管理薬を投与するための第2の吸入器を有する。センサーシステム(12A)は、第2の吸入器がシステムに含まれるとき、救急吸入の間および/または定期吸入の間の気流に関するパラメータを測定するように構成される。システムは、さらに、第1の期間内の救急吸入の回数を計測し、少なくとも数回の救急吸入および/または定期吸入の間に測定されたパラメータを受け取るように構成されたプロセッサー(14)を有する。プロセッサーは、重みづけされたモデルを用いて、救急吸入の回数およびパラメータに基づき喘息の増悪の確率を計算する。モデルは、救急吸入の回数が、確率計算においてパラメータよりも有意となるように重みづけされる。さらに、対象者における喘息の増悪の確率を計算するための方法が提供される。方法は重みづけされたモデルを用いる。【選択図】図2A system (10) is provided for calculating the probability of an asthma exacerbation in a subject. The system comprises a first inhaler (100) for administering rescue medication to a subject. Rescue drugs are suitable for treating impending respiratory ailments in a subject, for example, by rapidly dilating the bronchi or bronchioles upon inhalation of the drug. The first inhaler has a use detection system (12B) configured to count the number of rescue inhalations made by the subject using the first inhaler. The system optionally has a second inhaler for administering a maintenance medication to the subject during scheduled inhalation. The sensor system (12A) is configured to measure parameters related to airflow during emergency inhalation and/or during routine inhalation when a second inhaler is included in the system. The system further comprises a processor (14) configured to measure the number of emergency inhalations within the first period of time and receive parameters measured during at least some emergency inhalations and/or routine inhalations. . The processor uses the weighted model to calculate the probability of asthma exacerbation based on the number of rescue inhalations and parameters. The model is weighted so that the number of rescue inhalations is more significant than the parameters in the probability calculation. Further provided is a method for calculating the probability of an asthma exacerbation in a subject. The method uses a weighted model. [Selection drawing] Fig. 2
Description
本発明は、吸入器システム、特に、呼吸器疾患の増悪の確率を計算するシステムおよび方法に関するものである。 The present invention relates to inhaler systems, in particular systems and methods for calculating the probability of exacerbations of respiratory disease.
喘息または慢性閉塞性肺疾患(COPD)等の多くの呼吸器疾患は、治療が、患者の症状の管理と、回復不能な病変のリスクを減らすための薬剤の生涯にわたる投与とを含む、生涯にわたる病気である。現在、喘息およびCOPDのような病気に対する治療法は存在しない。
治療は2つの形態をとる。第1に、維持管理的な治療の側面では、気道の炎症を減らし、その結果、将来的に症状をコントロールすることが意図されている。維持管理的治療は、典型的に、吸入コルチコステロイドを単独で、あるいは長時間作用性気管支拡張剤および/またはムスカリン拮抗薬と組み合わせて処方することによって行われる。第2に、治療は救急(または救援)治療の側面も有し、この場合、患者は、喘息、咳、胸部圧迫および呼吸困難の激しい発作を緩和するための即効性の気管支拡張剤を投与される。
喘息またはCOPDのような呼吸器疾患を患った患者は、また、呼吸器疾患の症状をより悪化させる一時的な再燃あるいは増悪を経験するかもしれない。最悪の場合、増悪は患者の生命を脅かし得る。
Many respiratory disorders, such as asthma or chronic obstructive pulmonary disease (COPD), are lifelong, with treatment including lifelong administration of drugs to manage the patient's symptoms and reduce the risk of irreversible lesions. I'm sick. Currently, there is no cure for diseases like asthma and COPD.
Treatment takes two forms. First, in terms of maintenance treatment, it is intended to reduce airway inflammation and, as a result, control symptoms in the future. Maintenance treatment is typically given by prescribing inhaled corticosteroids alone or in combination with long-acting bronchodilators and / or muscarinic antagonists. Second, the treatment also has an aspect of emergency (or rescue) treatment, in which the patient is administered a fast-acting bronchial dilator to relieve severe attacks of asthma, cough, chest compressions and dyspnea. To.
Patients with respiratory illnesses such as asthma or COPD may also experience a temporary relapse or exacerbation that exacerbates the symptoms of the respiratory illness. In the worst case, exacerbations can be life-threatening for the patient.
切迫した呼吸器疾患の増悪を特定することができれば、行動計画を改善し、患者の症状が要求する前に、例えば、医師へのまたは医師からの予定外の訪問、入院およびステロイドの全身投与のような先行的治療の機会をもたらすことが可能になる。 If an exacerbation of an imminent respiratory illness can be identified, the action plan can be improved and, for example, unscheduled visits to or from a doctor, hospitalization and systemic administration of steroids before the patient's symptoms require. It will be possible to provide opportunities for such advanced treatment.
それ故、従来技術においては、切迫した呼吸器疾患の増悪のリスクを特定するための改善された方法が必要とされている。 Therefore, there is a need for improved methods to identify the risk of exacerbation of imminent respiratory illness in the prior art.
したがって、本発明は、対象者における喘息の増悪の確率を計算するシステムであって、対象者に救急薬を投与するための第1の吸入器を備え、第1の吸入器は対象者が第1の吸入器を使用することで実行される救急吸入を計測するように構成された使用検出システムを有し、さらに、定期吸入の間に対象者に維持管理薬を投与するための選択的な第2の吸入器と、第2の吸入器がシステムにおいて使用される場合に、第2の吸入器を使用した救急吸入および/または定期吸入の間に気流に関するパラメータを測定するように構成されたセンサーシステムと、第1の期間内に救急吸入の回数を測定し、少なくとも数回の救急および/または定期吸入の間のパラメータの測定値を受け取り、重みづけされたモデルを用いて、救急吸入の回数およびパラメータの測定値に基づき喘息の増悪の確率を計算するように構成されたプロセッサーと、を備え、モデルは、救急吸入の回数が確率の計算においてパラメータの測定値よりも有意となるように重みづけされていることを特徴とするシステムを提供したものである。 Therefore, the present invention is a system for calculating the probability of exacerbation of asthma in a subject, comprising a first inhaler for administering an emergency drug to the subject, and the first inhaler is the subject. It has a use detection system configured to measure the emergency inhalation performed by using one inhaler and is also selective for administering maintenance medication to the subject during routine inhalation. A second inhaler and, when the second inhaler is used in the system, was configured to measure airflow parameters during emergency inhaler and / or regular inhaler using the second inhaler. Using a sensor system and a weighted model that measures the number of emergency inhalations during the first period, receives parameter measurements during at least several emergency and / or regular inhalations, and uses an emergency inhaler Equipped with a processor configured to calculate the probability of asthma exacerbation based on the number of times and parameter measurements, the model allows the number of emergency inhalations to be more significant than the parameter measurements in the probability calculation. It provides a system characterized by being weighted.
救急吸入の回数と、救急および/または定期吸入の間の気流に関するパラメータの測定値とを用いることによって、喘息の増悪を予測するためのモデルであって、例えば、これらの因子のいずれかを無視したモデルよりも高い精度で予測が可能なモデルを提供することができる。
さらには、喘息の増悪を予測する場合、確率の計算において、救急吸入の回数が、気流に関するパラメータよりも有意となるようにした。結果的に、救急吸入の回数が確率の計算において吸入のパラメータよりも有意となるようにモデルを重みづけしたことから、確率の計算の精度が上がる。これは、吸入のパラメータが増悪の予測において救急吸入の回数よりも有意とされた、COPDの増悪を予測するトレンドと対照的である。
A model for predicting exacerbation of asthma by using the number of emergency inhalations and measurements of airflow parameters during emergency and / or regular inhalations, eg, ignoring any of these factors. It is possible to provide a model that can be predicted with higher accuracy than the model.
Furthermore, when predicting the exacerbation of asthma, the number of emergency inhalations was made more significant than the airflow parameters in the probability calculation. As a result, the model is weighted so that the number of emergency inhalations is more significant than the inhalation parameters in the probability calculation, which improves the accuracy of the probability calculation. This is in contrast to the trend of predicting exacerbations of COPD, where inhalation parameters were more significant than the number of emergency inhalations in predicting exacerbations.
装置、システムおよび方法を例示しつつなされる詳細な説明および具体例は、単に本発明の説明を目的としたものであって、本発明の範囲を限定するものではないことが理解されるべきである。本発明の装置、システムおよび方法のそれらのおよび別の特徴、態様および長所が、明細書の以下の説明、添付の特許請求の範囲および図面からより良く理解されるだろう。図面は概略的なものにすぎず、実際の寸法に合わせて描かれていないことが理解されるべきである。また、全図面を通じて同一または類似の構成要素には同一の番号が付されていることが理解されるべきである。 It should be understood that the detailed description and examples provided exemplifying the devices, systems and methods are solely for the purpose of explaining the present invention and do not limit the scope of the present invention. be. Those and other features, aspects and advantages of the devices, systems and methods of the invention will be better understood from the following description of the specification, the appended claims and drawings. It should be understood that the drawings are only schematic and are not drawn to the actual dimensions. It should also be understood that the same or similar components are numbered the same throughout the drawings.
喘息およびCOPDは気道の慢性炎症性疾患である。それらは共に気道閉塞および気管支麻痺の変化しやすく、再発する症状によって特徴づけられる。症状は、喘鳴、咳、胸部圧迫および呼吸困難の発作を含んでいる。 Asthma and COPD are chronic inflammatory diseases of the airways. They are both variable and characterized by recurrent symptoms of airway obstruction and bronchial paralysis. Symptoms include wheezing, coughing, chest compressions and dyspnea attacks.
症状は、トリガーを回避することおよび薬剤、特に吸入薬を使用することによってコントロールされる。薬剤は、吸入コルチコステロイドおよび吸入気管支拡張剤を含んでいる。 Symptoms are controlled by avoiding triggers and using medications, especially inhaled medications. Drugs include inhaled corticosteroids and inhaled bronchodilators.
吸入コルチコステロイド(ICS)は、呼吸器疾患を長期間コントロールする場合に使用されるステロイドホルモン剤である。それらは、気道炎症を弱めることで機能する。吸入コルチコステロイドは、例えば、ブデソニド、ベクロメタゾン(ジプロピオン酸ベクロメタゾン)、フルチカゾン(フルチカゾンプロピオン酸エステル)、モメタゾン(モメタゾンフランカルボン酸エステル)、シクレソニドおよびデクサメタゾン(デクサメタゾンナトリウム)を含んでいる。括弧は、好ましい塩またはエステルの形態を表す。 Inhaled corticosteroids (ICS) are steroid hormones used for long-term control of respiratory illness. They work by reducing airway inflammation. Inhaled corticosteroids include, for example, budesonide, beclomethasone (beclomethasone dipropionate), fluticasone (fluticasone propionate), mometasone (mometasone furancarboxylic acid ester), ciclesonide and dexametasone (sodium dexametasone). Parentheses represent the preferred salt or ester form.
分類が異なる気管支拡張剤は、気道内の異なる受容体をターゲットにしている。一般に使用される2つの分類は、β2刺激薬と抗コリン薬である。 Bronchodilators of different classifications target different receptors in the airways. The two commonly used categories are β 2 stimulants and anticholinergic drugs.
β2アドレナリン刺激薬(β2刺激薬)は円滑な筋肉弛緩を誘発するアドレナリン受容体に作用し、気道を拡張させる。長時間作用性β2刺激薬(LABA)は、例えば、ホルモテロール(フマル酸ホルモテロール)、サルメテロール(サルメテロールキシナホ酸塩)、インダカテロール(インダカテロールマレイン酸塩)、バンブテロール(バンブテロール塩酸塩)、クレンブテロール(クレンブテロール塩酸塩)、オロダテロール(オロダテロール塩酸塩)、カルモテロール(カルモテロール塩酸塩)、ツロブテロール(ツロブテロール塩酸塩)およびビランテロール(ビランテロールトリフェニル酢酸塩)を含んでいる。短時間作用性β2刺激薬(SABA)は、例えば、アルブテロール(硫酸アルブテロール)を含んでいる。 β 2 adrenergic stimulants (β 2 stimulants) act on adrenergic receptors that induce smooth muscle relaxation and dilate the airways. Long-acting β 2 stimulants (LABA) include, for example, formosterol (formotelol fumarate), salmesterol (salmeterol xinafoate), indacaterol (indacaterol maleate), vanbuterol (banbuterol hydrochloride), It contains clinbuterol (clinbuterol hydrochloride), odoratorol (orodaterol hydrochloride), carmoterol (carmoterol hydrochloride), turobterol (turobterol hydrochloride) and viranterol (viranterol triphenylacetate). Short-acting β 2 stimulants (SABAs) include, for example, albuterol (albuterol sulfate).
典型的に、短時間作用性気管支拡張剤は、急性気管支収縮からの迅速な救援を提供する(しばしば、「救急薬」または「リリーバー薬」と呼ばれる)一方、長時間作用性気管支拡張剤は、長時間にわたる症状のコントロールおよび予防を支援する。
しかしながら、ホルモテロール(フマル酸ホルモテロール)のような発現が早く、長時間作用性気管支拡張剤のいくつかは、救急薬として使用され得る。すなわち、救急薬は急性気管支収縮からの救援を提供する。救急薬は必要に応じて服用される。救急薬は、また、例えば、ICS-ホルモテロール(フマル酸ホルモテロール)、典型的にはブデソニド・ホルモテロールフマル酸塩水和物吸入剤のようなコンビネーション製品の形態をとり得る。こうして、救急薬は、好ましくは、SABAまたは発現が速いLABA、より好ましくは、アルブテロール(硫酸アルブテロール)またはホルモテロール(フマル酸ホルモテロール)、さらに好ましくは、アルブテロール(硫酸アルブテロール)からなっている。
Typically, short-acting bronchodilators provide rapid relief from acute bronchoconstriction (often referred to as "emergency medications" or "relievers"), while long-acting bronchodilators. Supports long-term symptom control and prevention.
However, some fast-acting, long-acting bronchodilators, such as formoterol (formoterol fumarate), can be used as first aid agents. That is, first aid provides relief from acute bronchoconstriction. First aid is taken as needed. The first aid may also take the form of a combination product such as, for example, ICS-formoterol (formoterol fumarate), typically budesonide formoterol fumarate hydrate inhaler. Thus, the emergency drug preferably consists of SABA or fast-expressing LABA, more preferably albuterol (albuterol sulfate) or formoterol (formoterol fumarate), and even more preferably albuterol (albuterol sulfate).
アルブテロール(サルブタモールとしても知られる)は、典型的に硫酸塩として投与され、本発明における好ましい救急薬である。 Albuterol (also known as salbutamol) is typically administered as a sulfate and is the preferred first aid agent in the present invention.
抗コリン作用薬(抗ムスカリン薬)は、神経伝達物質アセチルコリンを、神経細胞内のその受容体を選択的にブロックすることでブロックする。局所適用に際し、抗コリン作用薬は、主に、気道内に位置するM3ムスカリン授与体に作用し、円滑な筋肉弛緩を生じさせ、気管支拡張を生じさせる。
長時間作用性ムスカリン拮抗薬(LAMA)は、例えば、チオトロピウム(チオトロピウム臭化物)、オキシトロピウム(オキシトロピウム臭化物)、アクリジニウム(アクリジニウム臭化物)、イプラトピウム(イプラトピウム臭化物)、グリコピロニウム(臭化グリコピロニウム)、オキシブチニン(オキシブチニン塩酸塩またはオキシブチニン臭化水素酸塩)、トルテロジン(トルテロジン酒石酸塩)、トロスピウム(トロスピウム塩化物)、ソリフェナシン(ソリフェナシンコハク酸塩)、フェソテロジン(フェソテロジンフマル酸塩)およびダリフェナシン(ダリフェナシン臭化水素酸塩)を含んでいる。
Anticholinergic agents (antimuscarinic agents) block the neurotransmitter acetylcholine by selectively blocking its receptors in nerve cells. Upon topical application, anticholinergic agents act primarily on M3 muscarinic donors located in the airways , resulting in smooth muscle relaxation and bronchodilation.
Long-acting muscarinic antagonists (LAMA) include, for example, thiotropium (thiotropium bromide), oxytropium (oxytropium bromide), acridinium (acridinium bromide), ipratopium (ipratopium bromide), glycopyrronium (glycopyrro bromide). Nium), oxybutinine (oxybutinine hydrochloride or oxybutinine bromide hydrochloride), tortellodin (torterodin tartrate), trospium (trospium chloride), solifenasin (soliphenacin succinate), fesoterodin (fesoterodin fumarate) and dalifenasin. Contains (dalifenacin hydrobromide).
これまで、ドライパウダー吸入器(DPI)、圧力式定量吸入器(pMDI)およびネブライザー等を用いた吸入による投与のためにそれらの薬剤を準備し、処方する際に多数のアプローチがなされてきている。 To date, numerous approaches have been taken in preparing and prescribing these agents for administration by inhalation using a dry powder inhaler (DPI), pressure metered inhaler (pMDI), nebulizer, etc. ..
GINA(Global Initiative for Asthma:喘息管理に関する国際指針)のガイドラインによれば、段階的アプローチが喘息の治療のためにとられる。
軽症型の喘息を表す第1段階では、患者は硫酸アルブテロール等の必要に応じたSABAを与えられる。患者は、また、SABAが処方されるときはいつも、必要に応じた低用量のICS-ホルモテロールまたは低用量のICSを与えられるかもしれない。第2段階では、通常の低用量のICSがSABAまたは必要に応じた低用量のICS-ホルモテロールと一緒に与えられる。第3段階では、LABAが加えられる。第4段階では、各薬剤の用量が増やされ、第5段階では、さらに、抗コリン作用薬または低用量の経口コルチコステロイド等の追加の治療が含まれる。つまり、各段階は治療計画とみなすことができ、治療はそれぞれ、呼吸器疾患の急性重症度の程度に応じて構成される。
According to the GINA (Global Initiative for Asthma) guidelines, a step-by-step approach is taken for the treatment of asthma.
In the first stage, which represents mild asthma, the patient is given SABA as needed, such as albuterol sulfate. Patients may also be given low doses of ICS-formoterol or low doses of ICS as needed whenever SABA is prescribed. In the second step, the usual low dose ICS is given with SABA or optionally low dose ICS-formoterol. In the third stage, LABA is added. In the fourth stage, the dose of each drug is increased, and in the fifth stage, additional treatment such as an anticholinergic agent or a low dose of oral corticosteroid is included. That is, each stage can be regarded as a treatment plan, and each treatment is structured according to the degree of acute severity of respiratory disease.
COPDは世界中の主要な死因である。COPDは、慢性気管支炎や肺気腫、さらには狭気道を含む異質の長期間にわたる病気である。COPDを患った患者における病変は、主に、気道、肺実質および肺血管系に限定される。それらの病変は、肺のガスを吸い込み、吐き出す健全な能力を低下させる。 COPD is the leading cause of death worldwide. COPD is a heterogeneous, long-term illness that includes chronic bronchitis, emphysema, and even the narrow airways. Lesions in patients with COPD are primarily confined to the airways, pulmonary parenchyma and pulmonary vasculature. These lesions reduce the healthy ability of the lungs to inhale and exhale gas.
気管支炎は長期間にわたる気管の炎症によって特徴づけられる。一般的な症状は、喘鳴、呼吸困難、咳および喀痰の喀出を含み、これらの症状はすべて患者の生活の質にとって厄介かつ有害である。気腫はまた長期間にわたる気管支炎症に関係し、この場合、炎症に対する反応によって、肺組織の破壊および進行性の気道狭窄が生じる。やがて、肺組織はその自然な弾力性を失い、拡張する。そうなると、ガス交換機能が低下し、呼吸されたガスがしばしば肺に閉じ込められる。これは、局所化された低酸素症を引き起こし、1回の吸気当たりに患者の血流中に供給される酸素量を減少させる。そして、患者は呼吸困難を経験する。 Bronchitis is characterized by long-term inflammation of the trachea. Common symptoms include wheezing, dyspnea, coughing and sputum production, all of which are bothersome and detrimental to the patient's quality of life. Emphysema is also associated with long-term bronchial inflammation, in which case the response to inflammation results in destruction of lung tissue and progressive airway narrowing. Over time, lung tissue loses its natural elasticity and expands. When this happens, the gas exchange function is impaired and the breathed gas is often trapped in the lungs. This causes localized hypoxia and reduces the amount of oxygen delivered to the patient's bloodstream per inspiration. And the patient experiences dyspnea.
COPDとともに生活する患者は、日々、それらの様々の症状を、一部かもしれないが経験する。病気の重症度は種々の要因によって決定されるが、最も一般的には、病気の進行度と相関がある。それらの症状は、病気の重症度とは無関係に、安定したCOPDを表し、この病状が維持され、種々の薬剤の投与を通じてコントロールされる。治療法は変更され得るが、しばしば、吸入気管支拡張剤、抗コリン作用薬、長時間作用性および短時間作用性β2刺激薬および吸入コルチコステロイドを含んでいる。薬剤はしばしば単一治療としてまたは併用治療として投与される。 Patients living with COPD experience these various symptoms on a daily basis, although some may be part of them. Disease severity is determined by a variety of factors, but most commonly correlates with disease progression. Their symptoms represent stable COPD, regardless of the severity of the disease, and this condition is maintained and controlled through the administration of various agents. Treatment may vary, but often includes inhaled bronchodilators, anticholinergic agents, long-acting and short-acting β 2 stimulants and inhaled corticosteroids. The drug is often given as a single treatment or as a combination treatment.
患者は、GOLD(Global Initiative for Chronic Obstructive Lung Disease, Inc.:慢性閉塞性肺疾患のためのグローバルイニシアティブ)ガイドラインに定められたカテゴリーを用いて、患者のCOPDの重症度によって分類される。カテゴリーはA~Dからなり、治療法の推奨される最初の選択肢はカテゴリー毎に変わる。患者グループAは、必要に応じて、短時間作用性ムスカリン拮抗薬(SAMA)または短時間作用性β2刺激薬(SABA)を処方される。患者グループBは、長時間作用性ムスカリン拮抗薬(LAMA)または長時間作用性β2刺激薬(LABA)を処方される。患者グループCは、吸入コルチコステロイド(ICS)+LABA、またはLAMAを処方される。患者グループDは、ICS+LABA、および/またはLAMAを処方される。 Patients are categorized by the severity of their COPD using the categories defined in the GOLD (Global Initiative for Chronic Obstructive Lung Disease, Inc .) guidelines. The categories consist of A to D, and the first recommended treatment options vary from category to category. Patient group A is prescribed a short-acting muscarinic antagonist (SAMA) or a short-acting β 2 stimulant (SABA) as needed. Patient group B is prescribed a long-acting muscarinic antagonist (LAMA) or a long-acting β 2 stimulant (LABA). Patient group C is prescribed inhaled corticosteroid (ICS) + LABA, or LAMA. Patient group D is prescribed ICS + LABA and / or LAMA.
喘息またはCOPD等の呼吸器疾患を患った患者は、日々の基本的な病状の変化の範囲を超えた周期的な増悪に苦しむ。増悪は、追加の治療、つまり維持管理的治療の範囲を超えてなされる治療を必要とする急性の病状悪化である。 Patients with respiratory illnesses such as asthma or COPD suffer from periodic exacerbations that go beyond the scope of daily basic changes in the condition. Exacerbations are acute exacerbations that require additional treatment, that is, treatment that goes beyond maintenance treatment.
喘息については、中程度の増悪に対する追加の治療は、SABAおよび経口コルチコステロイドの反復投与および/またはコントロールされた酸素吸入(後者は入院を必要とする)からなる。重大な増悪に対しては、抗コリン作用薬(典型的にイプラトピウム臭化物)、噴霧SABAまたは硫酸マグネシウムが追加される。 For asthma, additional treatment for moderate exacerbations consists of repeated doses of SABA and oral corticosteroids and / or controlled oxygen inhalation (the latter requiring hospitalization). For significant exacerbations, anticholinergic agents (typically iplatopium bromide), nebulized SABA or magnesium sulphate are added.
COPDについては、中程度の増悪に対する追加の治療は、SABA、経口コルチコステロイドおよび/または抗生物質の反復投与からなる。重大な増悪に対しては、コントロールされた酸素吸入および/または呼吸サポート(いずれも入院を必要とする)が加えられる。 For COPD, additional treatment for moderate exacerbations consists of repeated doses of SABA, oral corticosteroids and / or antibiotics. Controlled oxygen inhalation and / or respiratory support (both requiring hospitalization) are added for significant exacerbations.
本明細書中では、用語「増悪」は中程度の増悪と重大な増悪の両方を含んでいる。 As used herein, the term "exacerbation" includes both moderate and severe exacerbations.
本発明は、呼吸器疾患の増悪を予測することによって、患者に対する治療に早期に介入し、それによって患者の転帰を改善することができる治療アプローチに係るものである。 The present invention relates to a therapeutic approach that can intervene early in the treatment of a patient by predicting the exacerbation of respiratory disease, thereby improving the outcome of the patient.
本発明によれば、対象者における喘息の増悪の確率を計算するシステムが提供される。システムは、対象者に救急薬を投与するための第1の吸入器を備えている。救急薬は例えば薬の吸入時に気管支および細気管支を迅速に拡張させることによって呼吸器症状の悪化を治療するのに適している。第1の吸入器は対象者が第1の吸入器を使用することで実行される救急吸入を計測するように構成された使用検出システムを有している。システムは、選択的に、定期吸入の間に前記対象者に維持管理薬を投与するための第2の吸入器を有している。センサーシステムは、第2の吸入器がシステムにおいて使用される場合に、第2の吸入器を使用した救急吸入および/または定期吸入の間の気流に関するパラメータを測定するように構成されている。 INDUSTRIAL APPLICABILITY According to the present invention, a system for calculating the probability of exacerbation of asthma in a subject is provided. The system is equipped with a first inhaler for administering the first aid to the subject. First aid is suitable for treating exacerbations of respiratory symptoms, for example by rapidly dilating the bronchi and bronchioles when inhaling the drug. The first inhaler has a use detection system configured to measure the emergency inhalation performed by the subject using the first inhaler. The system optionally has a second inhaler for administering the maintenance agent to the subject during regular inhalation. The sensor system is configured to measure parameters with respect to airflow during emergency inhalation and / or periodic inhalation using the second inhaler when the second inhaler is used in the system.
救急薬は、上述したようなものであり、典型的には、SABA、またはホルモテロール(フマル酸ホルモテロール)等の発現が速いLABAからなっている。救急薬は、また、例えば、ICS-ホルモテロール(フマル酸ホルモテロール)、典型的にはブデソニド・ホルモテロール(ブデソニド・ホルモテロールフタル酸塩)等のコンビネーション製品の形態を有している。
このようなアプローチは「MART」(maintenance and rescue therapy:維持療法および救済療法)と呼ばれる。しかしながら、救急薬が存在することは、本明細書中ではそれが第1の吸入器であることを表している。なぜなら、救急薬の存在は重みづけされたモデルにおいて決定的だからである。したがって、それは、救急薬、および救急薬と維持管理薬の組み合わせの両方をカバーする。これに対し、第2の吸入器は、使用された場合、治療の維持管理的な面において使用されるだけであり、救急目的では使用されない。重要な違いは、第1の吸入器が必要に応じて使用されるのに対し、第2の吸入器は、定期的に、所定の時間に使用される点にある。
The first aid is as described above and typically consists of SABA, or LABA with rapid expression such as formoterol (formoterol fumarate). The first aid also has the form of a combination product such as, for example, ICS-formoterol (formoterol fumarate), typically budesonide formoterol (budesonide formoterol phthalate).
Such an approach is called "MART" (maintenance and rescue therapy). However, the presence of an emergency drug indicates that it is the first inhaler herein. Because the presence of first aid is decisive in the weighted model. Therefore, it covers both emergency medicines and combinations of emergency medicines and maintenance medicines. In contrast, the second inhaler, when used, is only used in terms of maintenance and management of treatment, not for emergency purposes. An important difference is that the first inhaler is used as needed, while the second inhaler is used on a regular basis at a given time.
システムは、さらに、第1の期間内の救急吸入の回数を測定し、少なくとも数回の救急および/または定期吸入の間のパラメータの測定値を受け取るように構成されたプロセッサーを備えている。プロセッサーは、重みづけされたモデルを用いて、救急吸入の回数およびパラメータの測定値に基づき喘息の増悪の確率を計算する。モデルは、救急吸入の回数が確率の計算においてパラメータの測定値よりも有意となるように重みづけされている。
本発明によれば、さらに、対象者における喘息の増悪の確率を計算する方法が提供される。方法は、重みづけされたモデルを使用する。本発明のシステムに関して述べられた好ましい実施例はいずれもこの方法に適用され得るし、またその逆も成り立つ。
The system further comprises a processor configured to measure the number of emergency inhalations during the first period and receive parameter measurements during at least several emergency and / or regular inhalations. The processor uses a weighted model to calculate the probability of exacerbation of asthma based on the number of emergency inhalations and parameter measurements. The model is weighted so that the number of emergency inhalations is more significant than the parameter measurements in the probability calculation.
The present invention further provides a method of calculating the probability of exacerbation of asthma in a subject. The method uses a weighted model. Any of the preferred embodiments described with respect to the system of the invention can be applied to this method and vice versa.
喘息またはCOPDの増悪等の切迫した呼吸器疾患の憎悪のリスクを、種々の対象者に関係する要因および環境要因をモニタリングすることによって評価する試みがこれまでになされてきている。どの要因が考慮に入れられ、どの要因が無視されるべきかに関するチャレンジがこれまでになされてきている。リスクの評価にわずかなまたは無視し得る影響しか及ぼさない要因を無視することにより、例えば、より少量の処理リソース、バッテリー電力およびメモリ容量等々の計算のためのリソースを用いて、より効率的にリスク計算をすることが可能になる。より重要なことは、切迫した呼吸器疾患の増悪の確率の計算精度を上げることである。より正確なリスク評価によって、より効果的なアラームシステムを実現することができ、その結果、対象者により適切に医療介入することができるようになる。すなわち、増悪のリスクのより正確な評価は、緊急のリスク時に、対象者への介入をガイドする可能性を有している。 Attempts have been made to assess the risk of exacerbations of imminent respiratory illness, such as asthma or exacerbation of COPD, by monitoring factors and environmental factors associated with a variety of subjects. Challenges have been made on which factors should be taken into account and which should be ignored. By ignoring factors that have a negligible or negligible impact on risk assessment, risk is more efficient, for example, with less processing resources, resources for calculations such as battery power and memory capacity, etc. It becomes possible to calculate. More importantly, it is necessary to improve the accuracy of calculating the probability of exacerbation of imminent respiratory illness. A more accurate risk assessment can result in a more effective alarm system, resulting in better medical intervention for the subject. That is, a more accurate assessment of the risk of exacerbations has the potential to guide intervention in the subject in the event of an urgent risk.
増悪の確率が高い場合、治療計画の段階的な変更は、例えば、緊急のリスク時に対象者に対して構成されていた治療法に対して正当化され得る。あるいは、長期にわたって増悪の確率が低い場合には、より高い精度の確率計算は、目下の治療法のダウングレードを、あるいは撤回をも正当化するための指針として用いることができる。これは、例えば、対象者が、もはや自己の呼吸器疾患の病状と釣り合っていない高用量の薬剤を摂取するように要求されることがないことを意味する。 If the probability of exacerbation is high, a gradual change in treatment plan may be justified, for example, for a treatment that was configured for the subject at the time of urgent risk. Alternatively, if the probability of exacerbations is low over the long term, more accurate probability calculations can be used as a guide to justify the downgrade or even withdrawal of the current treatment. This means, for example, that subjects are no longer required to take high doses of medication that are no longer commensurate with the pathology of their respiratory illness.
本発明者は、広範な臨床研究を行い、以下で詳細に説明するように、喘息疾患の増悪の確率計算を、一定期間(第1の期間)内に対象者によって実行される救急薬の救急吸入の回数と、救急および/または維持管理薬の吸入の間の気流に関するパラメータ(の測定値)との両方に基礎づける重みづけされたモデルを用いることによって、喘息の増悪の確率の計算の精度を上げることができることを見出した。 The present inventor has conducted extensive clinical studies and, as described in detail below, a first-aid drug emergency calculation performed by a subject within a period of time (first period) to calculate the probability of exacerbation of asthma disease. Accuracy in calculating the probability of exacerbation of asthma by using a weighted model that is based on both the number of inhalations and the parameters (measurements) of airflow during the inhalation of emergency and / or maintenance medications. I found that I could raise it.
第1の期間は、救急吸入の回数が計測されるサンプリング期間に対応する。第1の期間は、例えば1~15日である。このサンプリング期間は、当該期間が救急吸入の回数のデータ収集に適切な長さとなるように選択される。サンプリング期間が短すぎると、増悪の信頼できる予測のために必要な量のデータを収集することができず、サンプリング期間が長すぎると、診断または予測にとって意味のある短期的な傾向との区別をつきにくくする平均化効果が生じてしまう。 The first period corresponds to a sampling period in which the number of emergency inhalations is measured. The first period is, for example, 1 to 15 days. This sampling period is selected so that the period is of appropriate length for data collection of the number of emergency inhalations. If the sampling period is too short, we will not be able to collect the amount of data needed for a reliable prediction of exacerbations, and if the sampling period is too long, we will distinguish it from short-term trends that are meaningful for diagnosis or prediction. An averaging effect that makes it difficult to attach will occur.
救急吸入の回数およびパラメータ(値)の両方を用いることで、例えば、これらの因子のいずれか一方を無視するモデルよりも高い精度での予測を可能にするモデルを形成することができる。さらに、臨床研究から、救急吸入の回数および救急吸入器の使用に関する傾向は、喘息の増悪の確率計算において、吸入の間の気流に関するパラメータよりも有意であることが見出された。パラメータは依然として喘息の増悪の確率の計算において有意な因子であるが、救急吸入の回数と比べると、確率に及ぼす影響を小さい。
したがって、モデルを、救急吸入の回数が確率計算においてパラメータよりも有意となるように重みづけすることによって、確率計算の精度がより高められる。
By using both the number of emergency inhalations and the parameters (values), it is possible to form a model that allows for more accurate predictions than, for example, a model that ignores one of these factors. In addition, clinical studies have found that trends in the number of emergency inhalations and the use of emergency inhalers are more significant in calculating the probability of exacerbation of asthma than parameters for airflow during inhalation. The parameters are still a significant factor in calculating the probability of exacerbation of asthma, but have a small effect on the probability when compared to the number of emergency inhalations.
Therefore, by weighting the model so that the number of emergency inhalations is more significant than the parameter in the probability calculation, the accuracy of the probability calculation is further improved.
モデルは、例えば、救急吸入の回数に関係づけられた第1の重みづけ係数と、パラメータに関係づけられた第2の重みづけ係数とを有している。救急吸入の回数(または救急薬使用に係る傾向)およびパラメータを定量化するために使用された異なるユニットを評価すべく標準化されたとき、第1の重みづけ係数は第2の重みづけ係数よりも大きくなり、それによって、救急吸入の回数が確率計算においてパラメータよりも有意となることが保証される。 The model has, for example, a first weighting factor associated with the number of emergency inhalations and a second weighting factor associated with the parameter. The first weighting factor is greater than the second weighting factor when standardized to evaluate the different units used to quantify the number of first-aid inhalations (or trends associated with first-aid drug use) and parameters. It increases, which ensures that the number of emergency inhalations is more significant than the parameter in the probability calculation.
確率計算は、部分的に救急吸入の回数に基づいている。確率計算の基礎を救急吸入の回数におくことは、モデルが、第1の期間内の救急吸入の絶対数および/または救急吸入の回数に基づく1または2以上の傾向を使用することを意味する。このような傾向は、救急吸入の回数それ自体ではなく、救急吸入の回数の変動からなる Probability calculations are based in part on the number of emergency inhalations. Placing the basis of the probability calculation on the number of emergency inhalations means that the model uses one or more trends based on the absolute number of emergency inhalations and / or the number of emergency inhalations during the first period. .. This tendency consists of fluctuations in the number of emergency inhalations, not the number of emergency inhalations themselves.
救急吸入の回数に基づく傾向は、例えば、1日のうちの特定の時間内に行われた吸引の回数を含んでいる。したがって、例えば夜間の吸入の回数が、1つの因子として、吸入の回数に含まれる。プロセッサーは、例えば、1日のうちのそのような時間内の救急薬の使用を記録すべく適当なクロック機能を備えている。 Trends based on the number of emergency inhalations include, for example, the number of inhalations made during a particular time of the day. Therefore, for example, the number of inhalations at night is included in the number of inhalations as one factor. The processor, for example, has a suitable clock function to record the use of emergency medicine during such time of the day.
第1の重みづけ係数は、救急吸入の絶対数および/または救急吸入の回数に基づく1または2以上の傾向を重みづけする。 The first weighting factor weights a tendency of 1 or 2 or more based on the absolute number of emergency inhalations and / or the number of emergency inhalations.
より一般的には、救急吸入の回数(例えば任意の関係する傾向を含む)は、モデルにおいて、(他の因子に対して)40%~95%、好ましくは55%~95%、より好ましくは60%~85%、最も好ましくは60%~80%、例えば約60%の有意性/重要性(重み)を有している。 More generally, the number of emergency inhalations (including, for example, any relevant trends) is 40% to 95%, preferably 55% to 95%, more preferably (relative to other factors) in the model. It has a significance / importance (weight) of 60% to 85%, most preferably 60% to 80%, for example about 60%.
確率計算は、また、第2の吸入器が備えられた場合に、第2の吸入器を用いた救急吸入の間および/または定期吸入の間の気流に関するパラメータに基づいている。パラメータは、吸入の間の気流に関する単一の因子に対応し、あるいはこのような因子を複数含んでいる。例えば、パラメータは、最大吸入流量、吸入量、吸入継続時間および吸入速度のうちの少なくとも1つである。時間対最大吸入流量は、例えば、吸入速度の尺度をもたらす。 The probabilistic calculation is also based on parameters for airflow during emergency inhalation and / or regular inhalation using the second inhaler when provided with a second inhaler. The parameters correspond to a single factor for airflow during inhalation, or include multiple such factors. For example, the parameter is at least one of maximum inhalation flow rate, inhalation volume, inhalation duration and inhalation rate. The time vs. maximum inhalation flow rate provides, for example, a measure of inhalation rate.
確率計算の基礎をパラメータにおくことは、モデルが、吸入の間の気流に関する1または2以上の因子および/または各因子に関係する1または2以上の傾向を使用することを意味する。このような傾向は各因子の変動に対応する。 Putting the basis of the probability calculation on the parameters means that the model uses one or more factors with respect to the airflow during inhalation and / or one or more tendencies associated with each factor. Such a tendency corresponds to the fluctuation of each factor.
第2の重みづけ係数は、吸入の間の気流に関する1または2以上の因子および/または各因子に関係する1または2以上の傾向を重みづけする。 The second weighting factor weights one or more factors with respect to airflow during inhalation and / or one or more tendencies associated with each factor.
より一般的には、吸入パラメータ(例えば任意の関係する傾向を含む)は、モデルにおいて、2%~49%または2%~30%、好ましくは2%~45%、より好ましくは5%~40パーセント、最も好ましくは10%~35%、例えば約10%または約35%の有意性/重要性(例えば重み)を有している。 More generally, the inhalation parameters (including, for example, any relevant tendencies) are 2% to 49% or 2% to 30%, preferably 2% to 45%, more preferably 5% to 40% in the model. It has a percentage, most preferably 10% to 35%, eg, about 10% or about 35% significance / significance (eg, weight).
喘息の増悪の確率は、第1の期間に続く増悪期間内に発生する切迫した喘息の増悪の確率である。こうして、モデルは、吸入データ、すなわち救急吸入の回数と、パラメータデータが収集される第1の期間に続く「増悪期間」と呼ばれる予め決定された期間内に発生する喘息の増悪の確率を計算可能にする。増悪期間は、例えば1~10日、例えば5日である。増悪期間は、モデルが当該期間内に増悪を予測する能力に基づいて選択され、予め決定された期間が、必要ならば、適切な治療のステップをとるのに十分に長くなることを保証する。 The probability of asthma exacerbation is the probability of an imminent asthma exacerbation that occurs during the exacerbation period following the first period. In this way, the model can calculate inhalation data, the number of emergency inhalations, and the probability of exacerbation of asthma occurring within a predetermined period called the "exacerbation period" following the first period in which parameter data is collected. To. The exacerbation period is, for example, 1 to 10 days, for example, 5 days. The exacerbation period is selected based on the ability of the model to predict exacerbations within that period, ensuring that the predetermined period is long enough to take appropriate treatment steps, if necessary.
いくつかの実施例において、生体に関するパラメータが、重みづけされたモデルの精度を上げるために当該モデルに含まれる。このような実施例では、プロセッサーが、例えば、生体に関するパラメータ(パラメータ値)を受け取るように構成される。データ入力ユニットが、例えば、システムに含まれ、対象者および/または医療従事者が生体に関するパラメータを入力できるようになっている。 In some embodiments, biological parameters are included in the model to improve the accuracy of the weighted model. In such an embodiment, the processor is configured to receive, for example, parameters (parameter values) relating to the living body. A data entry unit is included, for example, in the system to allow subjects and / or healthcare professionals to enter parameters related to the living body.
モデルは、例えば、生体に関するパラメータが、確率計算において、救急吸入の回数よりも低い有意性を有するように重みづけされている。言い換えれば、第3の重みづけ係数が生体に関するパラメータに関係づけられ、第3の重みづけ係数は救急吸入の回数に関係づけられた第1の重みづけ係数よりも小さくなるように設定される。第3の重みづけ係数は気流に関するパラメータに関係づけられた第2の重みづけ係数よりも大きくまたは小さくなるように設定される。 The model is, for example, weighted so that parameters relating to the living body have a lower significance than the number of emergency inhalations in the probability calculation. In other words, the third weighting factor is set to be related to the parameters relating to the living body, and the third weighting factor is set to be smaller than the first weighting factor related to the number of emergency inhalations. The third weighting factor is set to be greater or lesser than the second weighting factor associated with the airflow parameter.
好ましくは、第3の重みづけ係数は第2の重みづけ係数よりも小さい。予測力の順に、救急薬の使用が最も大きな影響力を及ぼし、次に吸入パラメータが続き、その次に生体に関するパラメータが続く。 Preferably, the third weighting factor is smaller than the second weighting factor. In order of predictive power, the use of first aid drugs has the greatest impact, followed by inhalation parameters, followed by biological parameters.
生体に関するパラメータは、例えば、体重、身長、ボディマス指数、収縮期および/または拡張期の血圧を含む血圧、性別、人種、年齢、喫煙歴、睡眠/活動パターン、増悪履歴、対象者に対し施された別の治療または投与された別の薬剤等々のうちから選択された1または2以上のパラメータである。1実施例では、生体に関するパラメータは、年齢、ボディマス指数および増悪履歴を含んでいる。別の実施例では、生体に関するパラメータは、増悪履歴および病歴、ボディマス指数および血圧、例えば、収縮期および/または拡張期血圧を含んでいる。 Biological parameters include, for example, body weight, height, body mass index, blood pressure including systolic and / or diastolic blood pressure, gender, race, age, smoking history, sleep / activity pattern, exacerbation history, and subject. One or more parameters selected from another treatment given, another drug administered, and so on. In one embodiment, the biological parameters include age, body mass index and exacerbation history. In another embodiment, biological parameters include exacerbation history and medical history, body mass index and blood pressure, such as systolic and / or diastolic blood pressure.
より一般的には、生体に関するパラメータは、モデルにおいて、1%~15%、好ましくは1%~12%、より好ましくは3%~10%、最も好ましくは4%~10%、例えば約5%または約8%の有意性/重要性(例えば重み)を有している。 More generally, the biological parameters are 1% -15%, preferably 1% -12%, more preferably 3% -10%, most preferably 4% -10%, eg about 5%, in the model. Or have about 8% significance / significance (eg weight).
非限定的な例において、救急吸入の回数(例えば、関係する傾向を含む)は、モデルにおいて40%~95%、好ましくは55%~90%、より好ましくは60%~85%、最も好ましくは60%~80%、例えば約60%または約80%の有意性/重要性(例えば重み)を有し、吸入パラメータ(例えば、関係する傾向を含む)は、モデルにおいて2%~49%、好ましくは2%~45%、より好ましくは5%~40%、最も好ましくは10%~35%、例えば約10%または約35%の有意性/重要性(例えば重み)を有し、生体に関するパラメータは、モデルにおいて1%~15%、好ましくは1%~12%、より好ましくは3%~10%、最も好ましくは4%~10%、例えば約5%または約8%の有意性/重要性(例えば重み)を有している。 In a non-limiting example, the number of emergency inhalations (eg, including relevant tendencies) is 40% to 95%, preferably 55% to 90%, more preferably 60% to 85%, most preferably in the model. It has a significance / significance (eg, weight) of 60% to 80%, such as about 60% or about 80%, and inhalation parameters (eg, including relevant tendencies) are preferably 2% to 49% in the model. Has a significance / significance (eg, weight) of 2% to 45%, more preferably 5% to 40%, most preferably 10% to 35%, such as about 10% or about 35%, and parameters relating to the living body. Is 1% to 15%, preferably 1% to 12%, more preferably 3% to 10%, most preferably 4% to 10%, eg, about 5% or about 8% significance / significance in the model. Has (eg weight).
より一般的には、天候または汚染のレベルに関する環境データ等の追加のデータソースがモデルに加えられ得る。このような追加のデータは、確率計算に関し、救急吸入の回数のデータよりも低い有意性を有するよう、そして選択的に、吸入パラメータのデータよりも低い有意性を有するように重みづけされる。 More generally, additional data sources such as environmental data regarding the level of weather or pollution may be added to the model. Such additional data is weighted to have a lower significance than the data on the number of emergency inhalations and, optionally, less than the data on the inhalation parameters, with respect to the probability calculation.
維持管理/定期吸入の回数は、選択的または付加的に、増悪の予測に対する有益な情報をもたらす。なぜなら、より少ない回数の維持管理/定期吸入(維持管理薬の投薬の順守が不十分なことを示している)は増悪のリスクを増大させるからである。 The number of maintenance / regular inhalations, selectively or additionally, provides useful information for predicting exacerbations. This is because a smaller number of maintenance / regular inhalations (indicating poor adherence to maintenance medications) increases the risk of exacerbations.
比較的単純な例では、(問題となる対象者に関する基準期間に対する)第1の吸入器を用いた救急吸入の回数の増加および/または第2の吸入器を用いた定期吸入の回数の減少(治療計画の順守が低いことを示している)は、吸入パラメータとともに、肺疾患の増悪の確率を高める肺機能の悪化を表す。 In a relatively simple example, an increase in the number of emergency inhalations using the first inhaler (relative to the reference period for the subject in question) and / or a decrease in the number of regular inhalations using the second inhaler (relative to the reference period for the subject in question). Poor adherence to the treatment regimen), along with inhalation parameters, represents a deterioration in lung function that increases the probability of exacerbation of lung disease.
具体例では、維持管理薬の投薬の順守が80%から55%に低下して、救急吸入器の使用が67.5%増加し、最大吸入流量が34%低下し、吸入量が23%低下し(それらはすべて患者の基準値からの変化率である)、前年に2回の増悪が発生し、BMIが28を超えていると、ROC-AUCを用いて(以下の図8および図17に関する説明参照)、次の5日間の喘息の増悪の確率が0.87となる。 In a specific example, adherence to maintenance medications decreased from 80% to 55%, emergency inhaler use increased by 67.5%, maximum inhalation flow decreased by 34%, and inhalation volume decreased by 23%. (They are all rates of change from the patient's reference value), and when two exacerbations occurred the previous year and the BMI exceeded 28, using ROC-AUC (FIGS. 8 and 17 below). The probability of exacerbation of asthma over the next 5 days is 0.87.
より一般的には、救急吸入の回数(例えば救急吸入の回数に関する傾向を含む)は確率計算において最も有意性のある因子である。 More generally, the number of emergency inhalations (including, for example, trends with respect to the number of emergency inhalations) is the most significant factor in the probability calculation.
モデルは線形または非線形のモデルである。モデルは、例えば、機械学習モデルからなっている。例えば、教師あり機械学習モデル等の教師ありモデルが使用される。使用されるモデルの具体的な形式に関係なく、既に説明したように、モデルは吸入パラメータよりも救急吸入の回数に対してより敏感である、すなわち反応するように構成されている。この敏感さは、重みづけされたモデルの「重みづけ」に対応している。 The model is a linear or non-linear model. The model consists of, for example, a machine learning model. For example, a supervised model such as a supervised machine learning model is used. Regardless of the specific form of the model used, as already described, the model is configured to be more sensitive, i.e., responsive to the number of emergency inhalations than the inhalation parameters. This sensitivity corresponds to the "weighting" of the weighted model.
非限定的的な例において、モデルは決定木を用いるように構成されている。ニューラルネットワークまたはディープラーニングモデル等の別の適当な技術がまた当業者によって検討され得る。 In a non-limiting example, the model is configured to use a decision tree. Other suitable techniques such as neural networks or deep learning models may also be considered by those of skill in the art.
呼吸器疾患の増悪を予測することとは関係なく、システムのプロセッサーは、吸入の回数、吸入パラメータ、および対象者が患っている呼吸器疾患の病状に関する指標に基づいて増悪の確率を計算する。指標を予測に含めることによって、予測精度が上がる。その理由は、ユーザー入力された指標が、例えば当該ユーザー入力された指標を用いずに吸入の回数および吸入パラメータを考慮に入れて導出された確率評価の予測値の正当性を立証し、より確かなものにすることを助けるからである。 Regardless of predicting the exacerbation of respiratory illness, the system's processors calculate the probability of exacerbation based on the number of inhalations, inhalation parameters, and indicators of the condition of the respiratory illness suffering by the subject. By including the index in the prediction, the prediction accuracy is improved. The reason is that the user-entered metric proves the validity of the predicted value of the probability assessment derived by taking into account the number of inhalations and the inhalation parameters, for example, without using the user-entered metric, and is more certain. Because it helps to make things.
1実施例において、プロセッサーは呼吸器疾患の増悪の初期確率を、記録された吸入の回数および受け取った吸入パラメータ(値)に基づくが、指標には基づくことなく計算する。初期確率は、例えば、上述のような重みづけされたモデルを用いて計算される。そして、確率、すなわち全体的な確率が吸入回数、吸入パラメータ、および受け取った、対象者が患った呼吸器疾患の症状に関する指標に基づいて計算される。例えば、全体的な確率は初期確率および受け取られた指標に基づいて計算される。 In one embodiment, the processor calculates the initial probability of exacerbation of respiratory disease based on the number of inhalations recorded and the inhalation parameters (values) received, but not on the index. The initial probabilities are calculated using, for example, a weighted model as described above. Probability, or overall probability, is then calculated based on the number of inhalations, inhalation parameters, and the received index of the symptoms of the respiratory illness suffered by the subject. For example, the overall probability is calculated based on the initial probability and the received index.
初期確率は、例えば、後の10日間の増悪のリスクを決定する。対象者が患った呼吸器疾患の病状の指標を考慮に入れた全体的な確率は、例えば、後の5日間の増悪のリスクを決定する。すなわち、確率計算に指標を含めることで、より短期間におけるより正確な予測が可能となる。 The initial probability determines, for example, the risk of exacerbations for the next 10 days. The overall probability of taking into account the indicators of the condition of the respiratory illness suffered by the subject determines, for example, the risk of exacerbations over the next 5 days. That is, by including the index in the probability calculation, more accurate prediction in a shorter period becomes possible.
確率計算にユーザー入力された指標を含めることによって、陽性および陰性の予測値、予測の感度、すなわち対象者がリスクにさらされているとシステム/方法が正しく判定する能力(真陽性率)、および予測の特異性、すなわち対象者がリスクにさらされていないとシステム/方法が正しく判定する能力(真陰性率)のうちの1または2以上が強化される。 By including user-entered indicators in the probability calculation, positive and negative predictions, prediction sensitivity, that is, the ability of the system / method to correctly determine that the subject is at risk (true positive rate), and Prediction specificity, i.e. one or more of the system / method's ability to correctly determine that a subject is not at risk (true negative rate), is enhanced.
吸入の回数および吸入パラメータのデータは、例えば、増悪に先立つ10日間の対象者の基準値からの偏差を表している。ユーザー入力された指標をその後の予測に含めることによって、陽性および陰性の予測値、および予測システム/方法の感度および特異性が改善される。 Data on the number of inhalations and inhalation parameters represent, for example, deviations from the subject's reference values for 10 days prior to exacerbations. Including user-entered indicators in subsequent predictions improves positive and negative predictions, as well as the sensitivity and specificity of the prediction system / method.
プロセッサーは、例えば、ユーザーにプロンプトを出力し、ユーザーから指標の入力を受けるユーザーインターフェイスを制御するように構成されている。プロンプトは、吸入の回数および吸入パラメータに基づいて、しかし指標には基づかずに計算された初期確率に基づいて出力される。プロンプトは、例えば、予め決定された閾値に達したまたはこれを超えた初期確率に基づいて出力される。こうして、ユーザーは、切迫した増悪の発生の可能性を示す初期確率に基づき、システムによって指標を入力するように促される。ユーザーが指標を入力することによって、指標を考慮に入れた(全体的な)確率が初期確率を裏付け、正当化することを助ける。 The processor is configured, for example, to output a prompt to the user and control the user interface to receive input from the user. Prompts are output based on the number of inhalations and inhalation parameters, but not on the basis of indicators, but on the calculated initial probabilities. The prompt is output, for example, based on the initial probability of reaching or exceeding a predetermined threshold. In this way, the user is prompted by the system to enter an indicator based on the initial probability of an imminent exacerbation. By inputting the metric, the (overall) probability that takes the metric into account helps to support and justify the initial probability.
これは、例えば、指標の「分析主導の使用」とみなされる。吸入の回数および吸入パラメータのデータが起こり得る対象者の呼吸器疾患の悪化を示すときに、ユーザー入力が要求される。 This is considered, for example, the "analysis-driven use" of the indicator. User input is required when data on the number of inhalations and inhalation parameters indicate a possible exacerbation of the subject's respiratory illness.
ユーザーインターフェイスは、例えば、ユーザーまたは対象者に、ポップアップ通知を通じて短い質問票を完成させることで指標を入力するように促される。いつポップアップ通知を出すかを決定するロジックは、救急および/または維持管理吸入の回数および/または時間、および吸入パラメータの変化等の主要な変数のずれによって発動される。 The user interface is prompted, for example, to enter the metric by completing a short questionnaire through a pop-up notification to the user or target audience. The logic that determines when to issue a pop-up notification is triggered by a shift in key variables such as the number and / or duration of emergency and / or maintenance inhalations, and changes in inhalation parameters.
選択的にまたは付加的に、システムは、ユーザーがユーザーインターフェイスを通じて指標を入力することを選択したとき、その指標を受け取るように構成される。例えば、医療従事者が指標が初期確率の計算を確かなものにするのに有用であると決定したとき。これは、例えば、指標の「要求に応じた」使用とみなされる。この要求は、例えば医療のプロによる評価に先立ってまたは評価の間に、患者または患者を担当する医師によってなされる。 Optionally or additionally, the system is configured to receive the metric when the user chooses to enter the metric through the user interface. For example, when a healthcare professional determines that an indicator is useful in ensuring the calculation of initial probabilities. This is considered, for example, the "on demand" use of the indicator. This request is made, for example, by the patient or the physician in charge of the patient prior to or during the evaluation by a medical professional.
こうして、ユーザーは、これがシステムおよび/または医療従事者によって必要であるとみなされたとき、指標を入力するように促されるにすぎない。これは、対象者の負担を有利に低減し、対象者が、入力を求められまたは促されたとき、つまり、このような入力が対象者の呼吸器疾患のモニタリングに関して望ましいときに指標を入力することを可能にする。これらの実施例で指標を入力することは、対象者が日常的に指標の入力を促される場合よりも実現可能性がある。 Thus, the user is only prompted to enter an indicator when this is deemed necessary by the system and / or healthcare professional. This advantageously reduces the burden on the subject and inputs indicators when the subject is prompted or prompted for input, i.e., when such input is desirable for monitoring the subject's respiratory illness. Make it possible. Entering the indicators in these examples is more feasible than when the subject is routinely prompted to enter the indicators.
1実施例において、ユーザーインターフェイスは、複数のユーザーが選択可能な呼吸器疾患の病状の選択肢を提供するように構成される。この場合、指標は少なくとも1つの病状の選択肢のユーザーによる選択によって決定される。 In one embodiment, the user interface is configured to provide multiple user selectable respiratory disease pathologies. In this case, the index is determined by the user's choice of at least one medical condition option.
例えば、ユーザーインターフェイスは、それぞれの回答が指標に対応する複数の質問からなる質問票を表示する。ユーザー、例えば対象者または対象者を担当する医療従事者がユーザーインターフェイスを使用して質問に対する回答を入力する。 For example, the user interface displays a questionnaire consisting of multiple questions, each answer corresponding to an indicator. A user, such as the subject or the healthcare professional responsible for the subject, uses the user interface to enter the answer to the question.
質問票は、対象者の負担を最小にすべく、比較的短く、つまり比較的少数の質問から構成される。それにもかかわらず、質問の数および内容は、指標によって増悪の確率の計算が、指標が全く入力されない場合よりも確かなものになるように設定される。 The questionnaire is relatively short, that is, it consists of a relatively small number of questions in order to minimize the burden on the subject. Nevertheless, the number and content of questions are set by the indicator to ensure that the calculation of the probability of exacerbation is more reliable than if no indicator was entered.
より一般的には、質問票の目的は、比較的素早く回答される少数の時機得た質問によって、対象者の(呼吸器疾患に関する)生活状態を即座に理解するために、目下のまたは比較的最近の(例えば直近の24時間以内の)指標を確認することにある。質問票は対象者の地方の言語に翻訳される。 More generally, the purpose of the questionnaire is to provide an immediate or relatively quick understanding of the subject's living conditions (related to respiratory illness) with a small number of timely questions answered relatively quickly. The purpose is to identify recent indicators (eg, within the last 24 hours). The questionnaire will be translated into the subject's local language.
一般的なコントロール質問票、特に喘息に関するACQ/T(Asthma Control Questionnaire/Test:喘息コントロール質問票/テスト)、あるいはCOPDに関するCAT(COPD Assessment Test:COPDアセスメントテスト)は、患者の過去の病状の想起に焦点が当てられがちであり、現在ではなく過去に焦点を当てると、予測的分析の目的の価値に悪影響を及ぼすおそれがある。 General control questionnaires, especially ACQ / T (Asthma Control Questionnaire / Test) for asthma, or CAT (COPD Assessment Test) for COPD, recall the patient's past medical conditions. Focusing on the past rather than the present can adversely affect the value of the purpose of predictive analysis.
次に、このような質問票の非限定的な例を説明する。対象者は、各質問に対して、状況を示す選択肢、いつも(5)、たいてい(4)、ときどき(3)、まれ(2)およびなし(1)のうちから1つを選ぶ。
1.あなたは呼吸困難をどれくらい頻繁に経験しますか、あるいはあなたの呼吸困難が発症する割合は?
2.あなたは咳をどれくらい頻繁に経験しますか、あるいはあなたの咳の発症する割合は?
3.あなたは喘鳴をどれくらい頻繁に経験しますか、あついはあなたの喘鳴の発症する割合は?
4.あなたはどれくらい頻繁に胸部圧迫を経験しますか、あるいはあなたの胸部圧迫の発症する割合は?
5.あなたはどれくらい頻繁に夜間の発症/睡眠への影響を経験しますか、あるいはあなたの夜間の発症/睡眠への影響の割合は?
6.あなたはどれくらい頻繁に職場、学校または家庭での制限を経験しますか、あるいはあなたの職場、学校または家庭での制限の割合は?
Next, a non-limiting example of such a questionnaire will be described. For each question, the subject chooses one of the situational options, always (5), usually (4), sometimes (3), rare (2), and none (1).
1. 1. How often do you experience dyspnea, or how often do you develop dyspnea?
2. 2. How often do you experience a cough, or how often do you develop a cough?
3. 3. How often do you experience wheezing, and what is the rate of wheezing?
4. How often do you experience chest compressions, or how often do you develop chest compressions?
5. How often do you experience nighttime onset / sleep effects, or what percentage of your nighttime onset / sleep effects?
6. How often do you experience work, school or home restrictions, or what percentage of your work, school or home limits?
質問票の別の例は、次のようなものである。
1.あなたは普段よりも多くの呼吸器症状を経験していますか(はい/いいえ)?
「はい」と答えた場合:
2.より多くの胸部圧迫または呼吸困難を経験していますか(はい/いいえ)?
3.より多くの咳を経験していますか(はい/いいえ)?
4.より多くの喘鳴を経験していますか(はい/いいえ)?
5.それはあなたの睡眠に影響していますか(はい/いいえ)?
6.それはあなたの家庭/職場/学校での活動を制限していますか(はい/いいえ)?
Another example of a questionnaire looks like this:
1. 1. Do you experience more respiratory symptoms than usual (yes / no)?
If you answered "yes":
2. 2. Are you experiencing more chest compressions or dyspnea (yes / no)?
3. 3. Are you experiencing more coughs (yes / no)?
4. Are you experiencing more wheezing (yes / no)?
5. Does it affect your sleep (yes / no)?
6. Does it limit your home / work / school activities (yes / no)?
これらの質問に対する回答は、例えば、スコアを計算するために使用され、スコアは、対象者が患った呼吸器疾患の病状の指標に含まれ、または対応する。 Answers to these questions are used, for example, to calculate scores, which are included in or correspond to indicators of the pathology of the respiratory illness suffered by the subject.
1実施例において、ユーザーインターフェイスは、選択可能なアイコン、例えば絵文字型のアイコンおよび/またはチェックボックスおよび/またはスライダーおよび/またはダイアルの形態の、状況を示す選択肢を提供するように構成される。こうして、ユーザーインターフェイスは、患者が患った呼吸器疾患の病状に関する指標を入力するための直接的かつ直感的な方法を提供する。このような直感的な入力法は、対象者自身が自己に関する指標を入力する際に特に有利である。なぜなら、比較的に容易に行えるユーザー入力は、対象者の呼吸器疾患の悪化によってもほとんど妨げられないからである。 In one embodiment, the user interface is configured to provide contextual choices in the form of selectable icons, such as pictogram icons and / or checkboxes and / or sliders and / or dials. Thus, the user interface provides a direct and intuitive way to enter indicators of the pathology of the respiratory illness suffered by the patient. Such an intuitive input method is particularly advantageous when the subject himself / herself inputs an index related to himself / herself. This is because the relatively easy user input is hardly hindered by the worsening of the subject's respiratory illness.
適当なユーザインターフェイスは、対象者が患った呼吸器疾患の病状の指標のユーザー入力を可能にする目的のために使用される。例えば、ユーザーインターフェイスはユーザー所有の装置の(第1の)ユーザーインターフェイスを備え、またはそれからなっている。ユーザー所有の装置は、例えば、パソコン、タブレットコンピュータおよび/またはスマートフォンである。ユーザー所有の装置がスマートフォンであるとき、(第1の)ユーザーインターフェイスは、例えば、当該スマートフォンのタッチスクリーンに対応する。 Appropriate user interfaces are used for the purpose of allowing user input of indicators of the pathology of the respiratory illness suffered by the subject. For example, the user interface comprises or consists of a (first) user interface for a user-owned device. User-owned devices are, for example, personal computers, tablet computers and / or smartphones. When the user-owned device is a smartphone, the (first) user interface corresponds, for example, to the touch screen of the smartphone.
1実施例において、システムのプロセッサー少なくとも部分的にユーザー所有の装置内の(第1の)プロセッサーを含んでいる。選択的にまたは付加的に、第1の吸入器および/または第2の吸入器は、例えば、(第2の)プロセッサーを有し、システムのプロセッサーは少なくとも部分的に吸入器に含まれた(第2のプロセッサー)を含んでいる。 In one embodiment, the processor of the system includes at least a (first) processor in a user-owned device. Optionally or additionally, the first inhaler and / or the second inhaler has, for example, a (second) processor, the processor of the system is at least partially included in the inhaler ( A second processor) is included.
本発明の方法は、対象者における喘息の増悪の確率を計算するために提供される。方法は、第1の期間内に対象者によって実行された、対象者の切迫した呼吸器疾患の治療に適した救急薬の救急吸入の回数を計測し、少なくとも数回の救急吸入の間および/または対象者によって実行された維持管理薬の定期吸入の間の気流に関するパラメータを測定し、重みづけされたモデルを用いて、救急吸入の回数およびパラメータの測定値に基づき喘息の増悪の確率を計算することを有し、モデルは、救急吸入の回数が確率の計算においてパラメータの測定値よりも有意となるように重みづけされていることを特徴とする。 The method of the present invention is provided to calculate the probability of exacerbation of asthma in a subject. The method measures the number of emergency inhalations of an emergency drug suitable for the treatment of the subject's imminent respiratory disease performed by the subject during the first period, during and / or at least several emergency inhalations. Alternatively, measure parameters for airflow during routine inhalation of maintenance medications performed by the subject, and use a weighted model to calculate the number of emergency inhalations and the probability of exacerbation of asthma based on the measured values of the parameters. The model is characterized in that the number of emergency inhalations is weighted to be more significant than the measured value of the parameter in the calculation of probability.
さらに、本発明によれば、対象者の喘息の増悪を治療する方法であって、上述した喘息の増悪の確率を計算する方法を実施し、確率が予め決定された上限に達するかまたは上限を超えるかどうかを判定し、あるいは、確率が予め決定された下限に達するかまたは下限よりも低いかどうかを判定し、上限に達したまたは上限を超えた確率に基づいて、または下限に達したまたは下限よりも低くなった確率に基づいて喘息を治療することを特徴とする方法が提供される。 Further, according to the present invention, a method for treating an exacerbation of asthma in a subject, wherein the method for calculating the probability of exacerbation of asthma described above is carried out, and the probability reaches a predetermined upper limit or is set to an upper limit. Determine if it exceeds, or determine if the probability reaches or is below a predetermined lower limit, and based on the probability of reaching or exceeding the upper limit, or reaching the lower limit A method comprising treating asthma based on the probability of being below the lower limit is provided.
治療は、確率が予め決定された上限に達しまたはこれを超えたとき、対象者に救急薬を投与すべく吸入器を使用することを含んでいる。 Treatment involves using an inhaler to administer an emergency drug to the subject when the probability reaches or exceeds a predetermined upper limit.
この治療法は、現存する喘息の治療法を変更する。現存する治療法は第1の治療計画を有しており、現存する治療法の変更は、第1の治療計画から、予め決定された閾値に達したまたはこれを超えた確率に基づく第2の治療計画に変更することからなり、第2の治療計画は第1の治療計画よりも高いリスクを有する喘息の増悪に対して作成される。 This treatment modifies existing treatments for asthma. The existing treatment has a first treatment plan, and the modification of the existing treatment is based on the probability that a predetermined threshold has been reached or exceeded from the first treatment plan. Composed of changing to a treatment plan, a second treatment plan is created for exacerbations of asthma that are at higher risk than the first treatment plan.
重みづけされたモデルを用いるより正確なリスク計算は、より効果的な警告システムの実現を容易にし、その結果、対象者に対する適切な医療介入がもたらされる。すなわち、増悪のリスクのより正確な評価によって、重大なリスク時の対象者への介入をガイドすることが可能になる。特に、介入は、第2の治療計画を実行することを含んでいる。これは、例えば、対象者をGINAまたはGOLDガイドラインに規定されたより高い段階に進めることを含んでいる。このような先手を取る介入は、正当化されるべき第2の治療計画に進むために、対象者が増悪に苦しめられ続ける必要がないこと、あるいは関係するリスクにさらされ続ける必要がないことを意味する。 More accurate risk calculations using weighted models facilitate the realization of more effective warning systems, resulting in appropriate medical intervention for the subject. That is, a more accurate assessment of the risk of exacerbations can guide intervention in the subject at critical risk. In particular, the intervention involves carrying out a second treatment plan. This includes, for example, advancing the subject to a higher stage as specified in the GINA or GOLD guidelines. Such preemptive interventions do not require the subject to continue to suffer from exacerbations or to continue to be exposed to the risks involved in order to proceed to a second treatment plan that should be justified. means.
1実施例において、第2の治療計画は、対象者にバイオ医薬品を投与することからなっている。比較的高額のバイオ医薬品は、対象者の治療をバイオ医薬品の投与を含めるべくステップアップすることが、注意深い考察および正当化を要求しがちであることを意味する。
本発明によるシステムおよび方法は、対象者が増悪を被るリスクに関しての信頼し得る予測を提供することで、バイオ医薬品の投与を正当化することができる。例えば、計算された確率が、予め決定された最小回数、高リスクの増悪を表す上限に達しまたはそれを超えたとき、バイオ医薬品の投与が定量的に正当化され、それに応じてバイオ医薬品が投与される。
In one example, the second treatment plan consists of administering a biopharmacy to the subject. Relatively expensive biopharmacy means that stepping up a subject's treatment to include biopharmacy administration tends to require careful consideration and justification.
The systems and methods according to the invention can justify the administration of biopharmacy by providing a reliable prediction of the subject's risk of suffering exacerbations. For example, when the calculated probability reaches or exceeds a predetermined minimum number of times, an upper limit representing a high-risk exacerbation, the administration of the biopharmacy is quantitatively justified and the biopharmacy is administered accordingly. Will be done.
より一般的には、バイオ医薬品は、オマリズマブ、メポリズマブ、レスリズマブ、ベンラリズマブおよびデュピルマブのうちのいずれか1つまたはそれらの2以上の組み合わせからなっている。 More generally, biopharmacy consists of any one of omalizumab, mepolizumab, reslizumab, benralizumab and dupilumab, or a combination of two or more thereof.
現存する喘息の治療法を変更することは、予め決定された下限に達するまたはこれより低い確率に基づき、第1の治療計画から、第1の治療計画よりも低リスクの喘息の増悪に対して作成された第3の治療計画に変更することからなる。 Changing existing treatments for asthma is based on the probability that a predetermined lower limit will be reached or lower, from the first treatment plan to a lower risk exacerbation of asthma than the first treatment plan. It consists of changing to the created third treatment plan.
例えば、増悪の確率が比較的長期間にわたって低い場合、確かな精度の確率計算は現存する治療計画のグレードダウンあるいは除外さえも正当化するためのアドバイスとして用いられる。特に、対象者は第1の治療計画から、第1の治療計画よりも低リスクの呼吸器疾患の増悪に対して作成された第3の治療計画に移行される。これは、例えば、対象者をGINAまたはGOLDガイドラインに規定されたより低い段階に進めることを含んでいる。 For example, if the probability of exacerbations is low over a relatively long period of time, reliable accurate probability calculations can be used as advice to justify downgrading or even excluding existing treatment regimens. In particular, subjects are transitioned from a first treatment plan to a third treatment plan created for exacerbations of lower-risk respiratory illness than the first treatment plan. This includes, for example, advancing the subject to a lower stage as specified in the GINA or GOLD guidelines.
また、本発明によれば、喘息の増悪を診断する方法であって、上述した対象者における喘息の増悪の確率を計算する方法を実施し、確率が、喘息の増悪を表す予め決定された上限に達するかまたは上限を超えるかどうかを判定し、上限に達したまたは上限を超えた確率に基づいて、喘息の増悪を診断することを特徴とする方法が提供される。 Further, according to the present invention, a method for diagnosing an exacerbation of asthma, wherein the method for calculating the probability of exacerbation of asthma in the above-mentioned subject is carried out, and the probability is a predetermined upper limit representing the exacerbation of asthma. Provided is a method comprising determining whether to reach or exceed the upper limit and diagnosing an exacerbation of asthma based on the probability of reaching or exceeding the upper limit.
さらに、本発明によれば、対象者における喘息の重症度を診断する方法であって、上述した対象者における喘息の増悪の確率を計算する方法を実施し、確率が、喘息がより重症であることを表す予め決定された上限に達したかまたは上限を超えたかどうかを判定し、あるいは、確率が、喘息がより軽症であることを表す下限に達したかまたは下限よりも低くなったかどうかを判定し、上限に達したまたは上限を超えた確率に基づいて喘息がより重症化したと診断し、または下限に達したまたは下限より低くなった確率に基づいて喘息がより軽症化したと診断することを特徴とする方法が提供される。 Further, according to the present invention, a method for diagnosing the severity of asthma in a subject and calculating the probability of exacerbation of asthma in the subject described above is carried out, and the probability is that asthma is more severe. Determine if a predetermined upper limit has been reached or exceeded, or if the probability has reached or is lower than the lower limit, which indicates that asthma is milder. Determine and diagnose asthma as more severe based on the probability of reaching or exceeding the upper limit, or more mild asthma based on the probability of reaching or lowering the lower limit A method characterized by that is provided.
さらに、本発明によれば、対象者の亜集団の境界を定めるための方法であって、対象者の母集団に属するそれぞれの対象者に対して上述した方法を実施し、それによって、母集団に属するそれぞれ対象者に対する喘息の増悪の確率を計算し、亜集団に対して計算した確率を母集団の残りに対して計算した確率から区別する確率の閾値または確率の範囲を設定し、確率の閾値または確率の範囲を用いて亜集団を母集団の残りから画定することを特徴とする方法が提供される。 Further, according to the present invention, there is a method for defining the boundaries of the subpopulations of the subjects, and the above-mentioned method is carried out for each subject belonging to the population of the subjects, thereby performing the population. Calculate the probability of exacerbation of asthma for each subject belonging to, set the threshold or range of probabilities to distinguish the calculated probabilities for the subpopulation from the calculated probabilities for the rest of the population, and set the probabilistic A method is provided characterized in that a subpopulation is defined from the rest of the population using a range of thresholds or probabilities.
図1は、本発明の1実施例によるシステム10のブロック図である。システム10は第1の吸入器100およびプロセッサー14を備えている。第1の吸入器100は、対象者にSABA等の救急薬を投与するために使用される。SABAは、例えばアルブテロールを含んでいる。第1の吸入器100は、センサーシステム12Aおよび/または使用検出システム12Bを有している。
FIG. 1 is a block diagram of a
システム10は、例えば選択的に「吸入器アッセンブリー」と呼ばれる。
The
第1の吸入器は、例えば選択的に「救急吸入器」と呼ばれる。 The first inhaler is selectively referred to, for example, as an "emergency inhaler".
第2の吸入器は、例えば選択的に「維持吸入器」または「管理吸入器」と呼ばれる。 The second inhaler is selectively referred to, for example, as a "maintenance inhaler" or a "managed inhaler".
救急吸入の回数が、第1の吸入器100に含まれた使用検出システム12Bによって計測される。
The number of emergency inhalations is measured by the
センサーシステム12Aはパラメータを測定するように構成される。センサーシステム12Aは、例えば、1または2以上の圧力センサーおよび/または温度センサーおよび/または湿度センサーおよび/または方向センサーおよび/または音響センサーおよび/または光学センサー等の1または2以上のセンサーを有している。圧力センサーは、気圧センサー(例えば、大気圧センサー)、差圧センサーおよび絶対圧センサー等々を含んでいる。センサーは、微小電気機械システム(MEMS)および/またはナノ電気機械システム(NEMS)の技術を使用する。
The
圧力センサーは特にパラメータの測定に適している。なぜなら、対象者による吸入の間の気流に関係する圧力変化を測定することによってモニタリングされるからである。以下で図18~図22を参照しつつより詳細に説明されるように、圧力センサーは、例えば、空気および薬剤がそれを通じて吸入の間に対象者によって吸入される流路内に、またはこの流路に連通して配置される。フローセンサーを使用する等のパラメータの別の測定法がまた当業者には明らかであろう。 Pressure sensors are particularly suitable for measuring parameters. This is because it is monitored by measuring the pressure changes associated with the airflow during inhalation by the subject. As described in more detail below with reference to FIGS. 18-22, the pressure sensor may be, for example, in a flow path through which air and agents are inhaled by the subject during inhalation, or this flow. It is placed in communication with the road. Other methods of measuring parameters, such as using a flow sensor, will also be apparent to those of skill in the art.
選択的または付加的に、センサーシステム12Aは、差圧センサーを備えている。差圧センサーは、例えば対象者がそれを通じて吸入する空気流路の一部を横切る圧力差を測定するためのデュアルポート型センサーからなっている。あるいは、シングルポートゲージ型センサーが使用される。後者は吸入の間と気流が存在しないときとの空気流路内の圧力差を測定する。測定値の差は吸入に関係する圧力の低下に対応する。
Optionally or additionally, the
図1には示されないが、システム10はさらに定期吸入の間に対象者に維持管理薬を投与するための第2の吸入器を備えている。第2の吸入器は、第1の吸入器100のセンサーシステム12Aおよび/または使用検出システム12Bとは異なるセンサーシステム12Aおよび/または使用検出システム12Bを有している。第2の吸入器のセンサーシステム12Aは、定期吸入の間のパラメータを測定するように構成される。例えば、センサーシステム12Aは、維持管理薬の吸入の間にパラメータを測定するための別の微小電気機械システム圧力センサーまたは別のナノ電気機械システム圧力センサー等の別の圧力センサーを有している。
Although not shown in FIG. 1, the
こうして、救急薬および維持管理薬の一方または両方の吸入が、対象者の肺機能および/または肺の健康に関する情報を収集するために用いられる。第1および第2の吸入器が使用されるとき、切迫した増悪の予測精度が、定期吸入および救急吸入の両方をモニタリングすることで供給された追加の吸入データによって改善される。 Thus, inhalation of one or both emergency and maintenance medications is used to collect information on the subject's lung function and / or lung health. When the first and second inhalers are used, the predictive accuracy of imminent exacerbations is improved by additional inhalation data provided by monitoring both regular and emergency inhalations.
定期吸入および救急吸入はそれぞれ、吸入が行われないときと比較して、空気流路内の圧力を低下させる。圧力がその最低となる点は、最大吸入流量に対応する。センサーシステム12Aは吸入時にこの点を検出する。最大吸入流量は吸入毎に異なり、対象者の病状に依存する。より低い最大吸入流量は、例えば、対象者が増悪に近づいているときに記録される。ここで使用される用語「最小の最大吸入流量」は、一定の(第2の)期間内に第1および/または第2の吸入器を用いて実行された吸入に関して記録された最大吸入流量のうちの最小のものを意味する。
Regular inhalation and emergency inhalation each reduce the pressure in the air flow path compared to when inhalation is not performed. The point where the pressure is at its lowest corresponds to the maximum suction flow rate. The
各吸入に関係する圧力変化は、選択的にまたは付加的に吸入量を測定するために用いられる。これは、例えば、吸入の間にセンサーシステム12Aによって測定された圧力変化を用いて、吸入の間にわたる流量を測定し、それから総吸入量を導出することによって達成される。より少ない吸入量は、例えば、対象者が増悪に近づいているときに記録される。なぜなら、対象者の吸入する能力が低下するからである。ここで使用される用語「最小吸入量」は、一定の(第3の)期間内に第1および/または第2の吸入器を用いて実行された吸入に関して記録された最小の吸入量を意味する。
The pressure changes associated with each inhalation are used to selectively or additionally measure the inhalation volume. This is achieved, for example, by using the pressure change measured by the
各吸入に関係する圧力変化は、選択的にまたは付加的に吸入継続時間を測定するために用いられる。例えば、吸入の開始に一致する、圧力センサー12Aによって測定された最初の圧力低下から、吸入が行われていないときの圧力に戻るまでの時間が記録される。より短い吸入継続時間が、例えば対象者が増悪に近づいているときに記録される。なぜなら、対象者の長時間吸入する能力が低下するからである。ここで使用される用語「最小吸入継続時間」は、一定の(第4の)期間内に第1および/または第2の吸入器を用いて実行された吸入に関して記録された最短の吸入継続時間を意味する。
The pressure changes associated with each inhalation are used to selectively or additionally measure inhalation duration. For example, the time from the initial pressure drop measured by the
1実施例において、パラメータは、例えば、最大吸入流量および/または吸入量および/または吸入継続時間の代わりとしてまたはそれに加えて、時間対最大吸入流量を含んでいる。この時間対最大吸入流量は、例えば、吸入の開始に一致する、センサーシステム12Aによって測定された最初の圧力低下から、圧力が最大流量に対応する最小値に達するまでに記録される。増悪のより大きなリスクにさらされた対象者は、長時間かけて最大吸入流量を達成する。
In one embodiment, the parameters include, for example, as a substitute for or in addition to the maximum inhalation flow rate and / or inhalation volume and / or inhalation duration, time vs. maximum inhalation flow rate. This time vs. maximum inhalation flow rate is recorded, for example, from the first pressure drop measured by the
非限定的な例において、第1および/または第2の吸入器は、通常吸入について、それぞれの薬剤が吸入の開始に続く約0.5秒間に投与されるように構成される。約1.5秒後等の、当該0.5秒が経過した後に最大吸入流量に達する対象者の吸入は、部分的に切迫した増悪を表している。 In a non-limiting example, the first and / or second inhaler is normally configured for inhalation such that each agent is administered for about 0.5 seconds following the onset of inhalation. The subject's inhalation, which reaches the maximum inhalation flow rate after the lapse of 0.5 seconds, such as after about 1.5 seconds, represents a partially imminent exacerbation.
使用検出システム12Bは、対象者による吸入(例えば、吸入器が救急吸入器であるときの対象者による各救急吸入、または吸入器が維持吸入器であるときの対象者による各維持管理吸入)を記録するように構成される。
非現定的な例において、第1の吸入器100は、薬剤タンク(図1では示されない)と、薬剤タンクから1回分の薬剤を計量するように構成された計量アッセンブリー(図1では示されない)とを備えている。使用検出システム12Bは、計量アッセンブリーによる1回分の薬剤の計量を記録するように構成され、各計量は対象者が第1の吸入器100を用いて行った救急吸入を表す。したがって、吸入器100は薬剤の救急吸入の回数をモニタリングするように構成される。なぜなら、1回分の薬剤は対象者によって吸入される前に計量アッセンブリーによって計量されねばならないからである。計量のための構成の1つの非限定的な例が、図18~図22を参照してより詳細に説明されるだろう。
The
In a non-constant example, the
選択的にまたは付加的に、使用検出システム12Bは、種々の方法でおよび/または当業者には明らかな付加的または選択的なフィードバックに基づいて各吸入を登録する。例えば、使用検出システム12Bは、センサーシステム12Aからのフィードバックが、対象者による吸入が発生していることを示すとき(例えば、圧力測定値または流量が成功した吸入に関係する予め決定された閾値を超えているとき)、対象者による吸入を登録するように構成される。さらに、いくつかの例において、使用検出システム12Bは、吸入器の切り替えまたは外部装置のユーザー入力(例えば、スマートフォンのタッチスクリーン)が、吸入前または吸入の間または吸入後に対象者によって手動的に行われたときに吸入を登録するように構成される。
Optionally or additionally, the
センサー(例えば圧力センサー)は、例えば、各吸入を登録するために使用検出システム12Bに含まれる。かかる例において、使用検出システム12Bおよびセンサーシステム12Aは、それぞれのセンサー(例えば圧力センサー)、または使用の検出および吸入パラメータの検出の両方の機能を実行できるように構成された共通のセンサー(例えば共通の圧力センサー)を使用する。
Sensors (eg, pressure sensors) are included in the
センサーが使用検出システム12Bに含まれるとき、センサーは、例えば、図18~図22を参照してより詳細に説明されるように、計量アッセンブリーによって計量された1回分の薬剤が対象者によって吸入されたことを確認し、あるいは当該吸入の程度を評価するために使用される。
When the sensor is included in the
1実施例において、センサーシステム12Aおよび/または使用検出システム12Bは音響センサーを有している。この実施例においける音響センサーは、対象者がそれぞれの吸入器を用いて吸入を行うときに発生するノイズを検出するように構成される。音響センサーは、例えばマイクロフォンからなっている。
In one embodiment, the
非限定的な例において、それぞれの吸入器は、対象者が装置を用いて吸入するときに回転するように配置されたカプセルを有している。カプセルの回転は音響センサによって検出可能なノイズを発生する。すなわち、カプセルの回転は、例えばカタカタ音等の使用および/または吸入パラメータのデータに導くための適当に解釈可能なノイズを提供する。 In a non-limiting example, each inhaler has a capsule that is arranged to rotate when the subject inhales with the device. The rotation of the capsule produces noise that can be detected by the acoustic sensor. That is, the rotation of the capsule provides a reasonably interpretable noise to guide the use and / or inhalation parameter data, such as rattling.
アルゴリズムが、例えば、音響データを解釈して使用のデータを測定するために(音響センサーが使用検出システム12Bに含まれるとき)および/または吸入の間の気流に関するパラメータを測定するために(音響センサーがセンサーシステム12Aに含まれるとき)使用される。
The algorithm, for example, to interpret acoustic data and measure data for use (when an acoustic sensor is included in the
例えば、Colthorpe(コルソープ)他、「Adding Electronics to the Breezhler; Satisfying the Needs of Patients(ブリーズヘラー(登録商標)への電子機器の追加;患者の要求を満足させること)」、Respiratory Drug Delivery(呼吸器ドラッグデリバリー)、2018年、71~79頁に記載されたようなアルゴリズムが使用される。一旦発生した音が検出されると、アルゴリズムは生の音響データを処理し、使用および/または吸入パラメータのデータを生成する。 For example, Colthorpe et al., "Adding Electronics to the Breezhler; Satisfying the Needs of Patients", Respiratory Drug Delivery, Respiratory Drug Delivery. Drug Delivery), 2018, an algorithm as described on pages 71-79 is used. Once the generated sound is detected, the algorithm processes the raw acoustic data to generate data for use and / or inhalation parameters.
システム10に含まれたプロセッサー14は、第1の期間内に救急および/または吸入吸入の回数を計測し、救急および/または定期吸入のそれぞれに関して測定されたパラメータを受け取る。図1において、センサーシステム12Aおよびプロセッサー14間、および使用検出システム12Bおよびプロセッサー14間の矢印によって示されるように、プロセッサーは、使用検出システム12Bおよびセンサーシステム12Aからそれぞれ吸入およびパラメータのデータを受け取る。プロセッサー14は、さらに、図3~図17を産所してより詳細に説明されるように、重みづけされたモデルを用いて、救急吸入の回数およびパラメータに基づき呼吸器疾患の増悪の確率を計算するように構成される。
The
非限定的な例において、プロセッサー14はそれぞれの第1および/または第2の吸入器から独立して配置される。この場合、プロセッサー14は、第1および/または第2の吸入器のセンサーシステム12Aおよび使用検出システム12Bから送信された救急吸入の回数およびパラメータのデータを受け取る。外部装置の処理ユニット等の外部処理ユニットにおいてデータを処理することによって、吸入器のバッテリーの寿命が有利に維持される。
In a non-limiting example, the
別の非限定的な例において、プロセッサー14は第1および/または第2の吸入器の不可欠の部分であり、例えば、第1および/または第2の吸入器の(図1には示されない)メインハウジング内または上部キャップ内に収容される。かかる例において、外部装置への接続に頼る必要はない。なぜなら、呼吸器疾患の増悪の確率の計算は第1および/または第2の吸入器の内部だけで行われるからである。第1および/または第2の吸入器は、例えば、光源、スクリーン、ラウドスピーカー等の、確率計算の結果を対象者に知らせるためのユーザーインターフェイスを含んでいる。確率を数字で知らせるよりむしろ、いくつかの例では、確率の計算値に応じて異なる色の光源を使用する等の、リスクを対象者に知らせるより直感的な手段が使用される。すなわち、第1および/または第2の吸入器は、例えば、対象者が救急薬を1または2回以上吸入する等の先手を取ったステップをとり、増悪のリスクを低減しあるいは除去するように促す。
In another non-limiting example, the
プロセッサー14の機能のいくつかが第1および/または第2の吸入器に含まれた内部処理ユニットによって実行され、確率計算それ自体のようなプロセッサーの他の機能が外部処理ユニットによって実行されるようにすることも可能である。
Some of the functions of the
より一般的には、システム10は、例えば、計算された確率を対象者および/または医師等の医療従事者に知らせるように構成された(図1には示されない)通信モジュールを有している。そして、対象者および/または医師は、呼吸器疾患の増悪の計算された確率に基づいて適切なステップをとる。例えばスマートフォン処理ユニットがプロセッサーに含まれるとき、SMS、Eメール、ブルートゥース(登録商標)等の、スマートフォンの通信機能が計算された確率を医療従事者に知らせるために使用される。
More generally, the
図2は、対象者における呼吸器疾患の増悪の確率を計算するシステム10の非限定的な例を示している。選択的に呼吸器疾患増悪リスク予測モデルと呼ばれる、重みづけされたモデルが、確率を計算するために使用され、そして、計算結果が対象者および/または介護者および/または医療従事者に提供される。
FIG. 2 shows a non-limiting example of a
システム10は、第1の吸入器100、外部装置15(例えばモバイル機器)、公共のおよび/または専用のネットワーク16(例えばインターネット、クラウドネットワーク等)およびパーソナルデータ記憶装置17を有している。外部装置15は、例えば、スマートフォン、パソコン、ラップトップパソコン、ワイヤレスメディア装置、メディアストリーミング装置、タブレット装置、ウェアラブル装置、Wi-Fiまたはワイヤレス通信可能なテレビ、または他の適当なインターネットプロトコルで接続可能な装置を含んでいる。例えば、外部装置15は、Wi-Fi通信リンク、Wi-MAX通信リンク、ブルートゥース(登録商標)またはブルートゥーススマート通信リンク、近距離無線通信(NFC)リンク、携帯電話通信リンク、またはテレビ用ホワイトスペース(TVWS)通信リンクまたはそれらの2以上の組み合わせを通じてRF信号を送信および/または受信するように構成される。外部装置15はデータを公共および/または専用ネットワーク16を通じてパーソナルデータ記憶装置17に送信する。
The
第1の吸入器100は、外部装置15にデータを送信するための、ブルートゥースラジオ等の通信回路を有している。データは上述した吸入の回数およびパラメータのデータを含んでいる。
The
第1の吸入器100は、また、例えば外部装置15から、例えばプログラム命令、オペレーティングシステムの変更、1回分の投薬量に関する情報、警告または通知、承認等のデータを受信する。
The
外部装置15は、プロセッサー14の少なくとも一部を含み、それによって、吸入の回数およびパラメータのデータを処理し、分析する。例えば、外部装置15は、ブロック18Aによって表されるように、呼吸器疾患の増悪の確率を計算するためのデータ等のデータを処理して、かかる情報を自動的な記憶のためのパーソナルデータ記憶装置17に提供する。
The
いくつかの非限定的な例において、外部装置15は、また、ブロック18Bによって表されるように、データを処理することによって、無吸入事象および/または低吸入事象および/または良好吸入事象および/または過吸入事象および/または呼気事象を特定する。外部装置15は、また、ブロック18Cによって表されるように、データを処理することによって、不十分な使用、過度の使用および最適の使用を特定する。外部装置15は、データを処理することによって、例えば、与えられたおよび/または残された1回分の投薬の回数を見積もり、対象者が計量アッセンブリーによって計量された1回分の投薬量の吸入を怠ったことを表すタイムスタンプエラーフラグに関係するエラー状態等のエラー状態を特定する。外部装置15は、ディスプレイ、およびディスプレイ上にGUIを通じて使用パラメータを視覚的に表示するためのソフトウェアを有している。使用パラメータは、リアルタイムデータに基づき増悪の将来的リスクを予測するために記憶されるパーソナライズされたデータとして記憶される。
In some non-limiting examples, the
いくつかの実施例では、パーソナルデータ記憶装置17に記憶されるものとして説明されたが、ブロック18Aによって示されたような呼吸器疾患の増悪の確率、ブロック18Bによって示されたような無吸入事象、低吸入事象、良好吸入事象、過剰吸入事象および/または呼気事象、および/またはブロック18Cによって示されたような不十分使用事象、過度使用事象および最適使用事象は、外部装置15にも記憶され得る。
In some examples, it was described as being stored in the personal
図3Aは、本発明の1実施例による方法20のフロー図である。方法20は、図1および/または図2に示されたシステム10のようなシステムによって実行される。例えば、第1および/または第2の吸入器および/または外部装置15および/またはパーソナルデータ記憶装置17のうちの1または2以上が、方法20の全部または一部を実行するように構成される。すなわち、ステップ22、24および26の任意の組み合わせが、第1の吸入器および/または第2の吸入器および/または外部装置15および/またはパーソナルデータ記憶装置17の任意の組み合わせによって実行される。さらに、ステップ22および24は任意の時間的順序で実行されることが理解されるべきである。
FIG. 3A is a flow chart of a
方法20は、第1の期間内に対象者によって行われる救急薬の救急吸入の回数を計測するステップ22を有している。ステップ24において、少なくとも数回、例えばそれぞれの救急および/または定期吸入の間の気流に関するパラメータが測定される。ステップ26において、重みづけされたモデルが喘息の増悪の確率を救急吸入の回数およびパラメータに基づいて計算するために使用される。モデルは、救急吸入の回数が、確率計算においてパラメータよりも有意となるように重みづけされる。
方法20において説明されないが、システム10は、喘息の増悪の確率が閾値を超える、またはそれより低くなるときユーザーに知らせるように構成される。例えば、システム10は、確率が予め決定された上限に達するかまたは上限を超えるかどうか、および/または、確率が予め決定された下限に達するかまたは下限よりも低いかどうかを判定するように構成される。それに応じて、システム10は、例えば、患者の治療計画を、当初の治療計画よりも喘息の増悪のリスクがより高い(より低い)場合に対し作成された治療計画に切り替えることによって(例えば、患者を担当する医療従事者へのメッセージを通じて)、患者を治療するように構成される。
Although not described in
システム10は、ユーザーに対し、喘息の増悪の確率を1または2以上の技術を通じて知らせる。例えば、システム10は、外部装置15のディスプレイ上にメッセージを表示し、ユーザーに関係する医療従事者または第三者にメッセージを送信し、吸入器100の指示器(例えばライトまたはスピーカー)を起動させてユーザーに知らせるように構成される。
図13Aに示された非限定的な例において、方法は、さらに、対象者が患った呼吸器疾患の病状に関する指標の入力を受けるステップ23を有している。この入力は、既に説明したように、増悪の予測の精度を上げるために使用される。
In the non-limiting example shown in FIG. 13A, the method further comprises
1実施例において、方法20は、ユーザーに対しプロンプトを出力し、ユーザーの入力を促すステップを有している。プロンプトは吸入の回数および吸入パラメータに基づいて、しかし指標には基づかずに出力される。例えば、プロンプトは、予め決定された閾値に達したまたはそれを超えた初期確率に基づいて出力される。こうして、ユーザーは、システムによって、切迫した増悪が起こり得ることを示す初期確率に基づき、指標を入力するように促される。そして、ユーザーが指標を入力することによって、指標を考慮に入れた(全体的な)確率が初期確率を確認または正当化するための助けとなる。
In one embodiment, the
図3Bは、本発明の別の実施例による方法に関するフロー図およびタイムラインである。タイムラインは、予測された増悪の発生の日(「[0]日」)、増悪に先立つ5日前(「[-5]日」)および増悪に先立つ10日前(「[-10]日」)を示している。 FIG. 3B is a flow chart and a timeline relating to the method according to another embodiment of the present invention. The timeline is the date of the predicted exacerbation (“[0] days”), 5 days prior to the exacerbation (“[-5] days”) and 10 days prior to the exacerbation (“[-10] days”). Is shown.
図3Bにおいて、ブロック222は、救急薬および/または維持管理薬の使用に関する通知とみなされる吸入器使用通知を表す。ブロック224は、吸入の間の気流に関するパラメータに対応する流量の通知を表す。ブロック225は、吸入器の使用および吸入パラメータに基づく組み合わされた通知とみなされる「使用」および「流量」の通知を表す。
In FIG. 3B, block 222 represents an inhaler use notice that is considered a notice regarding the use of emergency and / or maintenance medications.
ブロック226は予測の通知を表す。この予測の通知は、上で説明された初期確率の計算に基づく。図3Bは、[-10]日にブロック223における質問票の提示がなされたことを示している。質問票の提示は、ユーザーに対して質問票を通じて指標を入力することを促すプロンプトを出力することを含んでいる。ブロック227は、質問票の結果がユーザー入力後も増悪のリスクが残っていることを示すことを表す。これは、ブロック230において、質問票の提示が継続され、あるいはユーザーは再び指標を入力するように求められ、あるいは自己の呼吸器疾患の病状に関するさらなる入力を求められることを意味する。ブロック231は、増悪のリスクが、例えば上で説明された全体的な確率の計算の後も残っていることを表し、ブロック233において、増悪の予測の通知が継続するというシナリオを表す。
ブロック228は、ブロック223の質問票の提示の後、計算された増悪のリスクが、ユーザー入力された指標に基づいて、ベースラインまで戻るシナリオを表す。それに対応して、リスクの通知はブロック229において終了する。
同様に、ブロック232は、ブロック230の継続したまたはさらなる質問票の提示が終了した後、増悪のリスクがベースラインまで戻るシナリオを表す。(説明を簡単にするため)図3Bには示されないが、リスクの通知はブロック232において増悪のリスクがベースラインまで戻った後に終了する。
Similarly, block 232 represents a scenario in which the risk of exacerbation returns to baseline after the continuous or additional questionnaire presentation of
より一般的には、方法20はさらに対象者に救急薬を投与するための第1の吸入器を準備するステップを有している。第1の吸入器は対象者によって第1の吸入器を用いて行われた吸入を検出するように構成された使用検出システムを有している。
More generally, the
救急吸入の回数およびパラメータがそれぞれ救急薬を投与するための第1の吸入器に含まれた使用検出システムおよびセンサーシステムによって計測される。センサーシステムは、選択的または付加的に、既に説明されたように、第2の吸入器を使用した維持管理薬の定期吸入の間の気流に関するパラメータを測定する。 The number and parameters of emergency inhalation are measured by the use detection system and sensor system included in the first inhaler for administering the emergency drug, respectively. The sensor system selectively or additionally measures parameters for airflow during regular inhalation of maintenance medication using a second inhaler, as previously described.
ここで本発明の1実施例による方法を支える重みづけされたモデルは臨床試験の結果であった。これは次に説明されるだろう。以下の実施例は、説明のための非限定的な例であるとみなされるべきである。 Here, the weighted model supporting the method according to one embodiment of the present invention was the result of a clinical trial. This will be explained next. The following examples should be considered as non-limiting examples for illustration purposes.
研究の結果は別の形式の装置を用いて投与された別の救急薬にも一般に適用可能であるにもかかわらず、テバ・ファーマシューティカルズ・インダストリー(Teva Pharmaceutical Industries)によって市販されているプロエアー・ディジハラー(ProAir Digihalaer)(登録商標)を用いて投与されたアルブテロールが、12週間の多施設での非盲検試験において使用された。 Proair marketed by Teva Pharmaceutical Industries, although the results of the study are generally applicable to other first-aid drugs administered using another type of device. Albuterol administered using ProAir Digihalaer® was used in a 12-week multicenter open-label study.
悪化しやすい喘息を患った患者(18歳以上)が試験に採用された。患者は、必要に応じてプロエアー・ディジハラーを使用した(乳糖担体を含む硫酸塩としての90mcgのアルブテロールを、4時間毎に1~2回吸入した)。 Patients (aged 18+) with asthma, which is prone to exacerbation, were included in the study. Patients used Proair Digihaler as needed (90 mcg of albuterol as a sulfate containing lactose carrier was inhaled 1-2 times every 4 hours).
ディジハラーの電子モジュールは、各使用、すなわち各吸入および各吸入の間の気流に関するパラメータ、すなわち最大吸入流量、吸入量、時間対最大吸入流量および吸入継続時間を記録した。データが、吸入器から、臨床データとともにダウンロードされ、切迫した増悪を予測するためのモデルを開発するための機械学習アルゴリズムに適用された。 The Digihaller's electronic module recorded parameters for each use, ie airflow between each inhalation and each inhalation, namely maximum inhalation flow rate, inhalation volume, time vs. maximum inhalation flow rate and inhalation duration. The data were downloaded from the inhaler along with clinical data and applied to machine learning algorithms to develop models for predicting imminent exacerbations.
この実施例における臨床喘息増悪(CAE)の診断は、American Thoracic Society/European Respiratory Society statement(アメリカ胸部医学会/ヨーロッパ呼吸器学会公式ステートメント) (H.K. Reddel et al.(H.K.ラッデル他), Am J Respir Crit Care Med. 2009年、第180(1)巻、59~99頁)に基づくものであった。それは、「重大なCAE」および「並みのCAE」の両方を含んでいる。 The diagnosis of clinical asthma exacerbation (CAE) in this example is made by the American Thoracic Society / European Respiratory Society statement (HK Reddel et al.), Am J Respir Crit Care Med. 2009, Vol. 180 (1), pp. 59-99). It includes both "significant CAE" and "medium CAE".
重大なCAEは、経口ステロイド(プレドニゾンまたはその等価物)の少なくとも3日間の投与および入院を必要とする悪化した喘息を含むCAEとして規定される。
並みのCAEは、経口ステロイド(プレドニゾンまたはその等価物)の少なくとも3日間の投薬または入院を必要とする。
Significant CAE is defined as CAE containing exacerbated asthma requiring administration and hospitalization of oral steroids (prednisone or its equivalents) for at least 3 days.
Normal CAE requires at least 3 days of dosing or hospitalization of oral steroids (prednisone or its equivalents).
一般化されたモデルが、以下で図8を参照してより詳細に説明されるように、受信者動作特性(ROC)曲線解析によって評価された。 The generalized model was evaluated by receiver operating characteristic (ROC) curve analysis, as described in more detail below with reference to FIG.
試験の目的およびプライマリーエンドポイントは、ディジハラーによって捕捉された、CAEに先行するアルブテロールの使用パターンおよび使用量を単独で、またはCAEに先行する吸入の間の気流、身体活動および睡眠等々に関するパラメータのような他の試験データとの組み合わせにおいて調べることであった。この試験は、統合センサーを備え、吸入パラメータを測定可能な救急薬吸入装置の使用から導出される、CAEの予測のためのモデルを開発するための最初に成功した試みを提供する。 The purpose and primary endpoint of the study are parameters such as airflow, physical activity and sleep during CAE-preceding albuterol usage pattern and usage alone or during CAE-preceding inhalation captured by the Digihaller. It was to investigate in combination with other test data. This test provides the first successful attempt to develop a model for the prediction of CAE, which is derived from the use of an emergency drug inhaler equipped with an integrated sensor and capable of measuring inhalation parameters.
図4は、3人の異なる患者に対し彼らのそれぞれのディジハラーによって記録された異なる吸入パターンを示す3つのタイムラインを示している。最上位のタイムラインは、問題の患者が1度に1回の吸入を行うことを示している。最下位のタイムラインは、問題の患者が1セッションに2回または3回以上の連続した吸入を行うことを示している。ここで、用語「セッション」は、連続する吸入が60秒以内の時間間隔でなされる一連の吸入として規定される。中間に位置するタイムラインは、問題の患者が様々のパターンで吸入を行うことを示している。すなわち、ディジハラーは、救急吸入の回数を記録するだけでなく、使用のパターンも記録するように構成される。 FIG. 4 shows three timelines showing different inhalation patterns recorded by their respective digital hallers for three different patients. The top timeline shows that the patient in question makes one inhalation at a time. The lowest timeline shows that the patient in question makes two or more consecutive inhalations per session. Here, the term "session" is defined as a series of inhalations in which successive inhalations are made at time intervals of up to 60 seconds. An intermediate timeline shows that the patient in question performs inhalation in different patterns. That is, the Digihaller is configured to not only record the number of emergency inhalations, but also the pattern of use.
360人の患者が、ディジハラーから1以上の有効な吸入を行ったことがわかった。これら360人の患者が分析に含まれた。これらの患者のうち、64人の患者が総数73例のCAEを経験した。
図5は、救急吸入の平均回数対喘息の増悪からの日数のグラフ30である。図5は、増悪の発生日の前後14日のリスク期間のデータを示している。直線32は、リスク期間内の1日の救急吸入の平均回数に対応している。直線32は、直線34によって表された、基準となるリスク期間外の1日の救急吸入の平均回数よりもY軸上の高い位置にある。これは、増悪のリスクが高まるにつれて1日の救急吸入の平均回数が増加することを表している。参考までに、図5には、さらに、直線36によって表された、基準となる増悪を経験しなかった患者に関する1日の救急吸入の平均回数が示されている。
It was found that 360 patients received one or more effective inhalations from the Digihaller. These 360 patients were included in the analysis. Of these patients, 64 experienced a total of 73 CAEs.
FIG. 5 is a
図6は、救急吸入の平均回数対喘息の増悪からの日数の別のグラフ30である。図6は、増悪の発生日の前後50日の期間内のデータを示している。図6は、直線34によって表された、基準となるリスク期間外の1日の救急吸入の平均回数と比較して、増悪の発生する日が近づくにつれて、救急吸入器の使用回数が顕著に増加することを示している。
FIG. 6 is another
図7は、救急吸入の回数および気流に関する種々のパラメータのそれぞれの基準値に対する変化率対喘息の増悪からの日数の4つのグラフである。 FIG. 7 is a four graph of the rate of change vs. the number of days since exacerbation of asthma with respect to each reference value for the number of emergency inhalations and various parameters for airflow.
グラフ40は、救急吸入の回数の(リスク期間外の)基準値に対する変化率対喘息の増悪からの日数をプロットしたものである。救急吸入の回数は、増悪の直前に、基準値に対して90%増加することがわかった。
グラフ42は、1日の最小の最大吸入流量の基準値に対する変化率対喘息の増悪からの日数をプロットしたものである。グラフ42は、1日の最小の最大吸入流量が増悪に至るまでの日々において一般的に減少することを示している。1日の最小の最大吸入流量は、増悪の直前に、基準値に対して12%減少することがわかった。
グラフ44は、1日の最小吸入量の基準値に対する変化率対増悪からの日数をプロットしたものである。グラフ44は、1日の最小吸入量が増悪に至るまでの日々において一般的に減少することを示している。1日の最小吸入量は、増悪の直前に、基準値に対して20%減少することがわかった。
グラフ46は、1日の最小吸入継続時間の基準値に対する変化率対増悪からの日数をプロットしたものである。グラフ46は、1日の最小吸入継続時間が増悪に至るまでの日々において一般的に減少することを示している。1日の最小吸入継続時間は、増悪の直前に、基準値に対して15%~20%減少することがわかった。
第1の重みづけされた予測モデルを構成する際に、特にCAEに先立つ5日の期間内に、喘息の増悪に関する最も強い予測因子が、1日当たりの救急吸入の平均回数であることがわかった。気流に関するパラメーター、すなわち、最大吸入流量および/または吸入量および/または吸入継続時間がまた有意な予測値を有していることがわかった。 In constructing the first weighted predictive model, it was found that the strongest predictor of asthma exacerbation was the average number of emergency inhalations per day, especially within the 5-day period prior to CAE. .. It was found that the parameters related to airflow, namely the maximum inspiratory flow rate and / or the inspiratory volume and / or the inspiratory duration, also had significant predictors.
第1の重みづけされたモデルにおいて、喘息の増悪の確率の計算において最も有意な特性は、救急吸入の回数が61%、吸入傾向が16%、最大吸入流量が13%、吸入量が8%、夜間のアルブテロールの使用が2%であることがわかった。このような吸入特性がディジハラーによって収集され、最大吸入流量、時間対最大吸入流量、吸入量、吸入継続時間、夜間の使用およびそれらのパラメータの時間経過に伴う傾向が記録された。 In the first weighted model, the most significant characteristics in calculating the probability of exacerbation of asthma are 61% for emergency inhalation, 16% for inhalation tendency, 13% for maximum inhalation flow rate, and 8% for inhalation volume. , It was found that the use of albuterol at night was 2%. Such inhalation characteristics were collected by the Digihaller and recorded trends over time for maximum inhalation flow rate, time vs. maximum inhalation flow rate, inhalation volume, inhalation duration, nocturnal use and their parameters over time.
吸入傾向は、直近3日間と比較した今日の吸入量の変化率のような、人工的に作られたまたは設計されたパラメータである。別の例は、直近3日間と比較した今日の救急吸入の回数の変化率である。これらの例において、それぞれの傾向は、吸入量および救急吸入の回数それ自体ではなく、吸入量および救急吸入の回数のそれぞれの変化である。 Inhalation tendency is an artificially created or designed parameter, such as the rate of change in inhalation volume today compared to the last 3 days. Another example is the rate of change in the number of emergency inhalations today compared to the last 3 days. In these examples, each trend is a variation in the inhalation volume and the number of emergency inhalations, rather than the inhalation volume and the number of emergency inhalations themselves.
上の結果に基づき、第1の重みづけされた予測モデルが、喘息の増悪の確率を計算するために開発された。教師あり機械学習技術および勾配ブースティングが、分類問題(今後x日間で増悪が発生するか否か(増悪期間))を解決するために使用された。 Based on the above results, a first weighted predictive model was developed to calculate the probability of exacerbation of asthma. Supervised machine learning techniques and gradient boosting were used to solve the classification problem (whether exacerbations will occur in the next x days (exacerbation period)).
勾配ブースティング技術は、従来技術においてよく知られている。J.H. Friedman(J.H.フリードマン), Computational Statistics & Data Analysis(計算統計学およびデータ分析), 2002年、第38(4)巻、367~378頁、およびJ.H. Friedman et al.(J.H.フリードマン他), The Annals of Statistics(統計学年報)、2000年、第28(2)巻、337~407頁を参照されたい。それは、決定木(樹形モデルおよびその可能な帰結)からなる基本予測モデルのアンサンブル(複数の学習アルゴリズム)の形態の予測モデルを生み出す。それは、いくつかの適当な損失関数(データの例に対する推定値と真の値との差の関数)を最小化するための最適化アルゴリズムを用いることによって反復的なやり方で単一の強力な学習者モデルを形成する。最適化アルゴリズムは、応答変数の既知の値(今後x日間で増悪が発生するか否か)およびそれらの対応する予測値(特性および設計された特性のリスト)のトレーニングセットを用いて、損失関数の期待値を計算する。学習プロセスは、連続して新たなモデルに適合し、応答変数のより正確な予測値を提供する。 Gradient boosting techniques are well known in the prior art. J.H. Friedman, Computational Statistics & Data Analysis, 2002, Vol. 38 (4), pp. 376-378, and J.H. Friedman et al. (JH). Friedman et al.), The Annals of Statistics, 2000, Vol. 28 (2), pp. 337-407. It produces a predictive model in the form of an ensemble (multiple learning algorithms) of basic predictive models consisting of decision trees (tree-shaped models and their possible consequences). It is a single powerful learning in an iterative way by using an optimization algorithm to minimize some suitable loss function (the function of the difference between the estimated value and the true value for an example of the data). Form a person model. The optimization algorithm uses a training set of known values of the response variables (whether exacerbations will occur in the next x days) and their corresponding predicted values (list of characteristics and designed characteristics) to the loss function. Calculate the expected value of. The learning process continuously fits into the new model and provides more accurate predictions of the response variables.
表1は、第1の重みづけされた予測モデルに含まれた因子を、それらの相互の相対的な重みづけとともに例示列挙したものである。 Table 1 exemplifies the factors included in the first weighted predictive model, along with their relative weighting to each other.

切迫した喘息の増悪の確率を計算するための予測モデルにおける重要な因子は、救急吸入の回数および救急吸入の回数に関する傾向であるにもかかわらず、予測モデルは、これに吸入の間の気流に関するパラメータを補うことによってより確かなものとなった。
図8は、真陽性率を偽陽性率に対してプロットすることによってモデルの質を評価する、モデルの受信者動作特性(ROC)曲線解析を示す図である。この第1の重みづけされた予測モデルは、上述の関係する特性を用いて、0.75のAUC値を伴った後の5日間にわたる切迫した増悪を予測した。救急吸入の回数のみに基づく特性を用いたとき、AUC値は0.69となる。
Although an important factor in the predictive model for calculating the probability of exacerbation of imminent asthma is the tendency for the number of emergency inhalations and the number of emergency inhalations, the predictive model is associated with this regarding the airflow between inhalations. It became more reliable by supplementing the parameters.
FIG. 8 shows a receiver operating characteristic (ROC) curve analysis of a model that evaluates the quality of the model by plotting the true positive rate against the false positive rate. This first weighted predictive model used the relevant characteristics described above to predict an imminent exacerbation over the next 5 days with an AUC value of 0.75. When using the characteristic based only on the number of emergency inhalations, the AUC value is 0.69.
したがって、確率に及ぼす影響は救急吸入の回数よりも小さいにもかかわらず、吸入の間の気流に関するパラメータは、救急吸入の回数以外の他の因子と同様に、喘息の増悪の確率の計算精度を上げる有意な因子であることを示している。 Therefore, although the effect on probability is less than the number of emergency inhalations, the parameters for airflow during inhalation, like other factors other than the number of emergency inhalations, determine the accuracy of calculating the probability of exacerbation of asthma. It shows that it is a significant factor to raise.
第2の重みづけされた予測モデルが、第1の重みづけされた予測モデルを改善すべく、同じデータを用いて開発された。生体に関するパラメータがモデルに含められた。特に、病歴、モディマス指標(BMI)および血圧等の症例報告書(CRF)データが、ディジハラーのデータと組み合わせられて機械学習アルゴリズムに適用され、予測モデルが改良された。 A second weighted predictive model was developed using the same data to improve the first weighted predictive model. Biological parameters were included in the model. In particular, case report (CRF) data such as medical history, Modimas index (BMI) and blood pressure were combined with Digihaller data and applied to machine learning algorithms to improve predictive models.
アルゴリズムは、直近12カ月間の年齢、BMI、血圧および増悪の回数および入院回数に関してのみならず、ディジハラーによって収集された患者固有の吸入に関する情報に関してもトレーニングされた。基準特性および予測前の特性の間の比較、およびそれらの特性の変化の傾向が教師あり機械学習アルゴリズムに適用された。4分割交差検証技術が性能測定基準を比較するために使用され、勾配ブースティングが最適アルゴリズムとして選択された。前のように、一般化されたモデルが、受信者動作特性曲線(ROC)および同曲線下の面積(AUC)の解析によって評価された。 The algorithm was trained not only on age, BMI, blood pressure and number of exacerbations and hospitalizations over the last 12 months, but also on patient-specific inhalation information collected by Digihaller. Comparisons between reference and unpredicted characteristics, and trends in changes in those characteristics, were applied to supervised machine learning algorithms. Four-fold cross-validation techniques were used to compare performance metrics, and gradient boosting was selected as the optimal algorithm. As before, the generalized model was evaluated by analysis of the receiver operating characteristic curve (ROC) and the area under the curve (AUC).
表2は、第2の重みづけされた予測モデルに含まれた因子を、それらの相互の相対的な重みづけとともに例示列挙したものである。 Table 2 exemplifies the factors included in the second weighted predictive model, along with their relative weighting to each other.
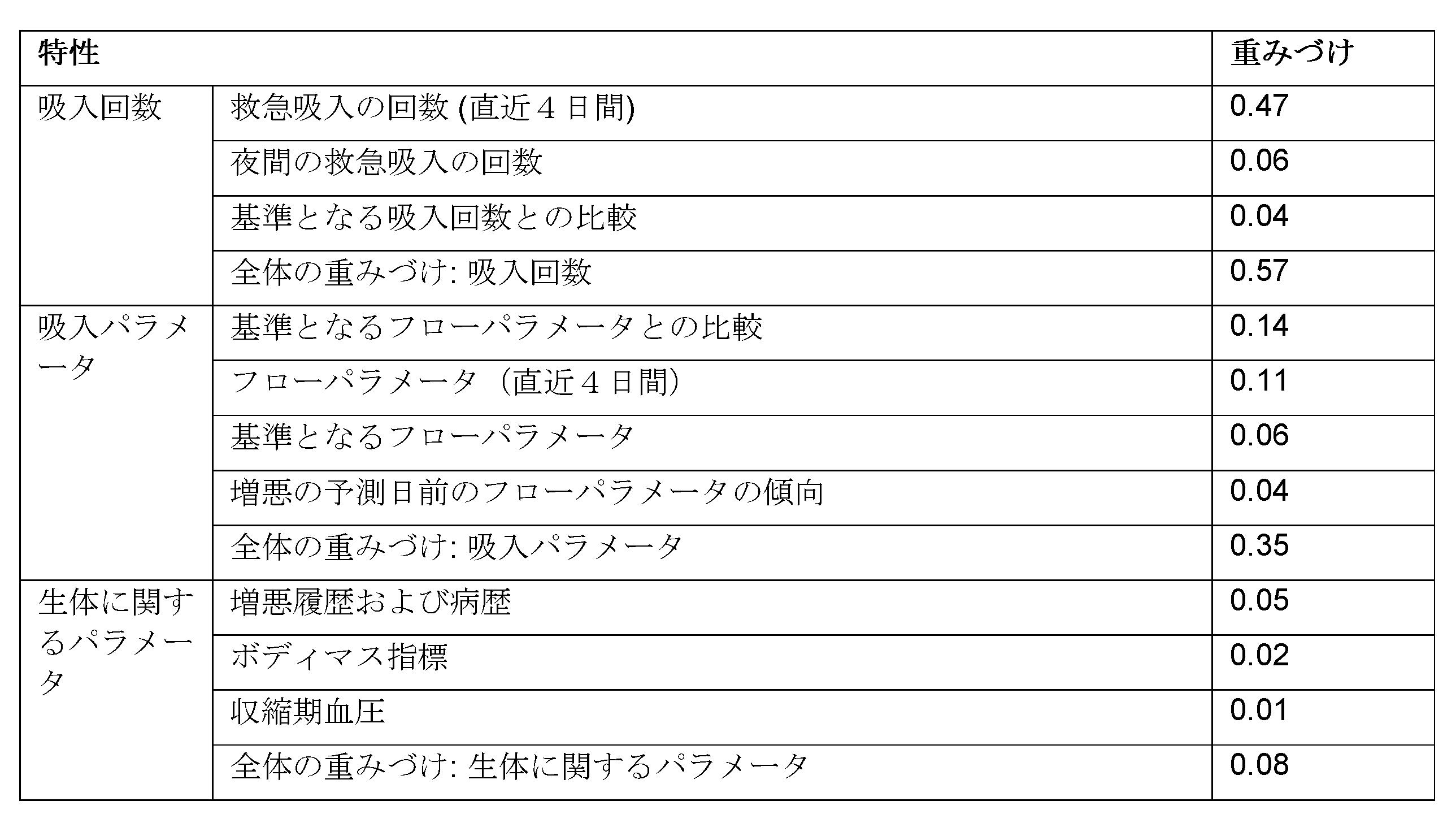
第2の重みづけされた予測モデルは、0.83のAUC値を伴ったその後の5日間の切迫した増悪を予測した。第2の重みづけされた予測モデルは、68.8%の感度および89.1%の特異度を有している。こうして、第2の重みづけされた予測モデルは、上で説明された、0.75のAUC値を伴った第1の重みづけされた予測モデルよりも改善された喘息増悪予測モデルであることが示された。第2の重みづけされた予測モデルの追加の改良は、少なくとも部分的に生体に関するパラメータの導入に帰する。 A second weighted predictive model predicted an imminent exacerbation for the next 5 days with an AUC value of 0.83. The second weighted predictive model has a sensitivity of 68.8% and a specificity of 89.1%. Thus, the second weighted predictive model may be an improved asthma exacerbation predictive model over the first weighted predictive model with an AUC value of 0.75 described above. Shown. The additional refinement of the second weighted predictive model is at least partially attributed to the introduction of biological parameters.
より一般的には、救急吸入の回数が計測されるべき第1の期間は、1~15日、好ましくは3~8日である。第1の期間にわたって救急吸入の回数をモニタリングすることは、喘息の増悪の確率の計算において特に有効である。 More generally, the first period in which the number of emergency inhalations should be measured is 1 to 15 days, preferably 3 to 8 days. Monitoring the number of emergency inhalations over the first period is particularly useful in calculating the probability of exacerbation of asthma.
吸入パラメータが最大吸入流量を含むとき、方法20は、さらに、最小または平均最大吸入流量のような最大吸入流量を、第2の期間内に行われた吸入に関して測定された最大吸入流量から計算するステップを有している。第2の期間に関する用語「第2の」は、最大吸入流量のサンプリングの期間を、救急吸入の回数がサンプリングされる第1の期間と区別することを意図している。第2の期間は少なくとも部分的に第1の期間と重なり得るし、あるいは第1および第2の期間が一致していてもよい。
When the inhalation parameter includes a maximum inspiratory flow rate,
こうして、喘息の増悪の確率を計算するステップ26は、部分的に最小または平均最大吸入流量に基づいている。第2の期間は、例えば、1日等の、1~5日である。第2の期間は、上で第1の期間に関して説明された考察と同様のやり方で、適当な値の最大吸入流量のデータを収集するのに要する時間に従って選択される。 Thus, step 26 of calculating the probability of exacerbation of asthma is based in part on the minimum or average maximum inhalation flow rate. The second period is 1 to 5 days, for example, 1 day. The second period is selected according to the time required to collect data for the maximum inhalation flow of appropriate values, in a manner similar to the discussion described for the first period above.
喘息の増悪の確率の計算は、例えば、図7のグラフ42のように、部分的に最小または平均最大吸入流量の基準となる最大吸入流量に対する変化に基づいている。
The calculation of the probability of exacerbation of asthma is based, for example, on the change with respect to the maximum inspiratory flow rate, which is the basis for the partially or average maximum inspiratory flow rate, as shown in
増悪の予測の改善された精度に対し、最小または平均最大吸入流量の基準となる最大吸入流量に対する変化は、例えば、10%またはそれ以上(50%またそれ以上または90%またはそれ以上等)である。基準値は、増悪が発生しなかった期間、例えば1~20日間、好ましくは10日間にわたって測定された1日の最小の最大吸入流量を用いて計算される。選択的または付加的に、最小または平均最大吸入流量は、絶対値に対して評価される。 For the improved accuracy of exacerbation prediction, the change to the maximum inspiratory flow rate, which is the basis for the minimum or average maximum inspiratory flow rate, is, for example, 10% or more (50% or more or 90% or more, etc.). be. Reference values are calculated using the minimum daily maximum inhalation flow measured over a period of no exacerbations, eg, 1-20 days, preferably 10 days. Selectively or additionally, the minimum or average maximum inspiratory flow rate is evaluated relative to the absolute value.
方法20は、さらに、第3の期間内に行われた吸入に関して測定された吸入量から、最小または平均吸入量のような吸入量を計算するステップを有している。第3の期間に関する用語「第3の」は、吸入量をサンプリングする期間を、救急吸入の回数がサンプリングされる第1の期間、および最大吸入流量データがサンプリングされる第2の期間から区別することを意図している。第3の期間は、少なくとも部分的に第1の期間および/または第2の期間と重なり得るし、あるいは、第3の期間が第1の期間および第2の期間のうちの少なくとも一方と一致していてもよい。
こうして、喘息の増悪の確率を計算するステップ26は、部分的に最小または平均吸入量に基づいている。第3の期間は、例えば、1~5日である。第3の期間は、上で第1の期間に関し説明された考察に類似したやり方で、適当な値の最小吸入量データを収集するのに要する時間に従って選択される。 Thus, step 26 of calculating the probability of exacerbation of asthma is based in part on the minimum or average inhalation dose. The third period is, for example, 1 to 5 days. The third period is selected according to the time required to collect the minimum inhalation amount data of appropriate values in a manner similar to the discussion described for the first period above.
喘息の増悪の確率の計算は、例えば、図7のグラフ44のように、部分的に最小または平均吸入量の基準となる吸入量に対する変化に基づいている。
The calculation of the probability of exacerbation of asthma is based in part on changes to the reference inhalation volume of the minimum or average inhalation dose, as shown in
増悪の予測の改善された精度に対し、最小または平均吸入量の基準となる吸入量に対する変化は、例えば、10%またはそれ以上(50%またそれ以上または90%またはそれ以上等)である。基準値は、増悪が発生しなかった期間、例えば1~10日間にわたって測定された1日の最小吸入量を用いて計算される。選択的または付加的に、最小または平均最大吸入流量は、絶対値に対して評価される。 For the improved accuracy of exacerbation prediction, the change in the minimum or average inhalation volume relative to the reference inhalation volume is, for example, 10% or more (50% or more or 90% or more, etc.). Reference values are calculated using the minimum daily inhalation dose measured over a period of no exacerbations, eg 1-10 days. Selectively or additionally, the minimum or average maximum inspiratory flow rate is evaluated relative to the absolute value.
方法20は、さらに、第4の期間にわたる吸入に関して測定された吸入継続時間から最小または平均吸入継続時間を計算するステップを有している。第4の期間に関する用語「第4の」は、最小吸入継続時間をサンプリングする期間を、救急吸入の回数がサンプリングされる第1の期間、および最大吸入流量データがサンプリングされる第2の期間、吸入量データがサンプリングされる第3の期間から区別することを意図している。第4の期間は、少なくとも部分的に第1の期間および/または第2の期間および/または第3の期間と重なり得るし、あるいは、第4の期間が第1の期間および第2の期間および第3の期間のうちの少なくとも1つと一致していてもよい。
こうして、喘息の増悪の確率を計算するステップ26は、部分的に最小または平均吸入継続時間に基づいている。第4の期間は、例えば、1日等の、1~5日である。第4の期間は、上で第1の期間に関し説明された考察に類似したやり方で、適当な目安値の最小吸入継続時間データを収集するのに必要な時間に従って選択される。 Thus, step 26 of calculating the probability of exacerbation of asthma is based in part on the minimum or average inhalation duration. The fourth period is 1 to 5 days, for example, 1 day. The fourth period is selected according to the time required to collect the minimum inhalation duration data of appropriate reference values in a manner similar to the discussion described for the first period above.
喘息の増悪の確率の計算は、例えば、図7のグラフ46のように、部分的に最小または平均吸入継続時間の基準となる吸入継続時間に対する変化に基づいている。
The calculation of the probability of exacerbation of asthma is based, for example, on a change with respect to the inhalation duration, which is partly the basis for the minimum or average inhalation duration, as in
増悪の予測の改善された精度に対し、最小または平均吸入継続時間の基準となる吸入継続時間に対する変化は、例えば、10%またはそれ以上(50%またそれ以上または90%またはそれ以上等)である。基準値は、増悪が発生しなかった期間、例えば1~20日間にわたって測定された1日の最小吸入継続時間を用いて計算される。選択的または付加的に、最小または平均最大吸入継続時間は、絶対値に対して評価される。 For the improved accuracy of exacerbation prediction, the change in inhalation duration as the basis for the minimum or average inhalation duration is, for example, 10% or more (50% or more or 90% or more, etc.). be. Reference values are calculated using a minimum daily inhalation duration measured over a period of no exacerbations, eg, 1-20 days. Selectively or additionally, the minimum or average maximum inhalation duration is evaluated relative to the absolute value.
COPDの増悪の予測に影響を及ぼす因子をより良く理解するため、別の臨床試験が行われた。以下に説明する実施例は、1つの説明のための、非限定的な例とみなされるべきである。 Another clinical trial was conducted to better understand the factors that influence the prediction of exacerbations of COPD. The embodiments described below should be regarded as a non-limiting example for one explanation.
試験の結果は別の形式の装置を用いて投与された別の救急薬にも一般に適用可能であるにもかかわらず、テバ・ファーマシューティカルズ・インダストリー(Teva Pharmaceutical Industries)によって市販されているプロエアー・ディジハラー(ProAir Digihaler)(登録商標)を用いて投与されたアルブテロールが、12週間の多施設での非盲検試験において使用された。 Proair marketed by Teva Pharmaceutical Industries, although the results of the study are generally applicable to other first aid drugs administered using another type of device. Albuterol administered using ProAir Digihaler® was used in a 12-week multicenter open-label study.
ディジハラーは、吸入の総数、最大吸入流量、時間対最大吸入流量、吸入量および吸入継続時間を記録可能な状態であった。データが、試験の最後に、ディジハラーの電子モジュールからダウンロードされた。 The digital haller was in a state where it was possible to record the total number of inhalations, the maximum inhalation flow rate, the time vs. the maximum inhalation flow rate, the inhalation amount and the inhalation duration. The data was downloaded from Digihaller's electronic module at the end of the test.
切迫したCOPDの増悪(AECOPD)がこの試験の主要な結果の評価基準であった。この試験において、AECOPDは「重大なAECOPD」または「並みのAECOPD」のいずれかの発症からなる。この試験では、「軽度のAECOPD」はAECOPDの評価基準として使用されなかった。 Imminent exacerbation of COPD (AECOPD) was the primary criterion for the outcome of this study. In this study, AECOPD consists of the onset of either "serious AECOPD" or "ordinary AECOPD". In this study, "mild AECOPD" was not used as a criterion for AECOPD.
重大なAECOPDは、少なくとも2日連続して全身性コルチコステロイド(SCS、基準値より上の少なくとも10mgのプレドニゾン等価物)および/または全身性抗生物質を使用した治療と、AECOPDの治療のための入院を必要とする呼吸器疾患の悪化を含む事象として規定される。 Critical AECOPD is for treatment with systemic corticosteroids (SCS, at least 10 mg prednisone equivalent above baseline) and / or systemic antibiotics for at least 2 consecutive days and for the treatment of AECOPD. It is defined as an event that involves exacerbation of respiratory illness that requires hospitalization.
並みのAECOPDは、少なくとも2日連続してSCS(基準値より上の少なくとも10mgのプレドニゾン等価物)および/または全身性抗生物質を使用した治療と、(電話通話、病院訪問、緊急治療訪問または救急治療訪問等の)AECOPDの治療のための予定外の接触を必要とするが、入院は必要としない呼吸器疾患の悪化を含む事象として規定される。 Normal AECOPD is treated with SCS (at least 10 mg of prednisone equivalent above baseline) and / or systemic antibiotics for at least two consecutive days and (telephone call, hospital visit, emergency treatment visit or emergency). It is defined as an event involving exacerbation of respiratory illness that requires unscheduled contact for treatment of AECOPD (such as a treatment visit) but does not require hospitalization.
COPDを患った患者(40歳以上)が試験のために採用された。患者は、必要に応じてプロエアー・ディジハラーを使用した(乳糖担体を含む硫酸塩としての90mcgのアルブテロールを、4時間毎に1~2回吸入した)。 Patients with COPD (40+) were recruited for the study. Patients used Proair Digihaler as needed (90 mcg of albuterol as a sulfate containing lactose carrier was inhaled 1-2 times every 4 hours).
次のような選択基準が要求された。すなわち、患者はスクリーニングの前の直近12カ月にわたって並みのまたは重大なAECOPDのうちの少なくと1つを発症し、SABAに加えて、LABA、ICS/LABA、LAMAまたはLABA/LAMAのうちの少なくとも1つの投与を受けており、ディジハラーからアルブテロールを適切に使用したことを実証することができ、試験の期間中、他のすべての救急または維持管理SABAまたは短時間作用性抗ムスカリン剤の使用を中断し、それらを試験のために提供されるディジハラーに切り替えることができること。 The following selection criteria were requested. That is, the patient develops at least one of moderate or significant AECOPD over the last 12 months prior to screening, and in addition to SABA, at least one of LABA, ICS / LABA, LAMA or LABA / LAMA. Having received one dose, it was possible to demonstrate proper use of albuterol from Digihaller and discontinue use of all other emergency or maintenance SABA or short-acting antimuscarinic agents during the study. , Being able to switch them to the digital hallers provided for testing.
患者は、調査員の意見で、試験への参加を妨げる(治療中のまたは未治療の)臨床的に重要な症状がある場合、例えば、COPD以外の他の混乱を生じさせる根本的な肺障害を有している場合、投薬中断後の5半減期以内または1カ月の訪問2回のうちのどちらか長い方の期間内に治験薬を使用していた場合、うっ血性心不全を発症していた場合、妊娠していた場合または授乳期の場合、または試験中に妊娠する可能性がある場合には、試験から排除された。 In the investigator's opinion, the patient has an underlying pulmonary disorder that causes confusion other than COPD, for example, if there are clinically significant symptoms (under treatment or untreated) that prevent participation in the trial. If the study drug was used within the 5 half-life after discontinuation of medication or within the longer of the two visits per month, congestive heart failure had developed. If you were pregnant or during the lactation period, or if you were likely to become pregnant during the trial, you were excluded from the trial.
約100人の患者から構成された2つのサブ集団が、加速度計を、身体活動(一日の総歩数(Total Daily Steps;TDS))を測定するために足首に、あるいは睡眠障害(睡眠障害指数(Sleep Disturbance Index;SDI))を測定するために手首に装着するよう要求された。 Two subpopulations, consisting of about 100 patients, have accelerometers on their ankles to measure physical activity (Total Daily Steps (TDS)) or sleep disorders (sleep disorder index). (Sleep Disturbance Index; SDI)) was requested to be worn on the wrist to measure.
救急薬に関する興味ある一般的因子は、
(1)AECOPDの最大に先行する、1日の吸入総回数
(2)AECOPDの最大に先行するアルブテロールの使用回数が増加したときの日数
(3)AECOPDに先行する24時間のアルブテロールの使用回数
であった。
A common factor of interest for first aid is
(1) Total number of inhalations per day preceding the maximum of AECOPD (2) Number of days when the number of times of use of albuterol preceding the maximum of AECOPD increases (3) Number of times of use of albuterol for 24 hours preceding AECOPD there were.
約400人の患者が登録された。これにより、試験を終えた366人の価値ある患者がもたらされた。336例のディジハラーによる有効な吸入が記録された。この点に関するさらなる詳細が表3に示されている。 About 400 patients were enrolled. This resulted in 366 valuable patients who completed the study. Effective inhalation by 336 Digihallers was recorded. Further details in this regard are shown in Table 3.
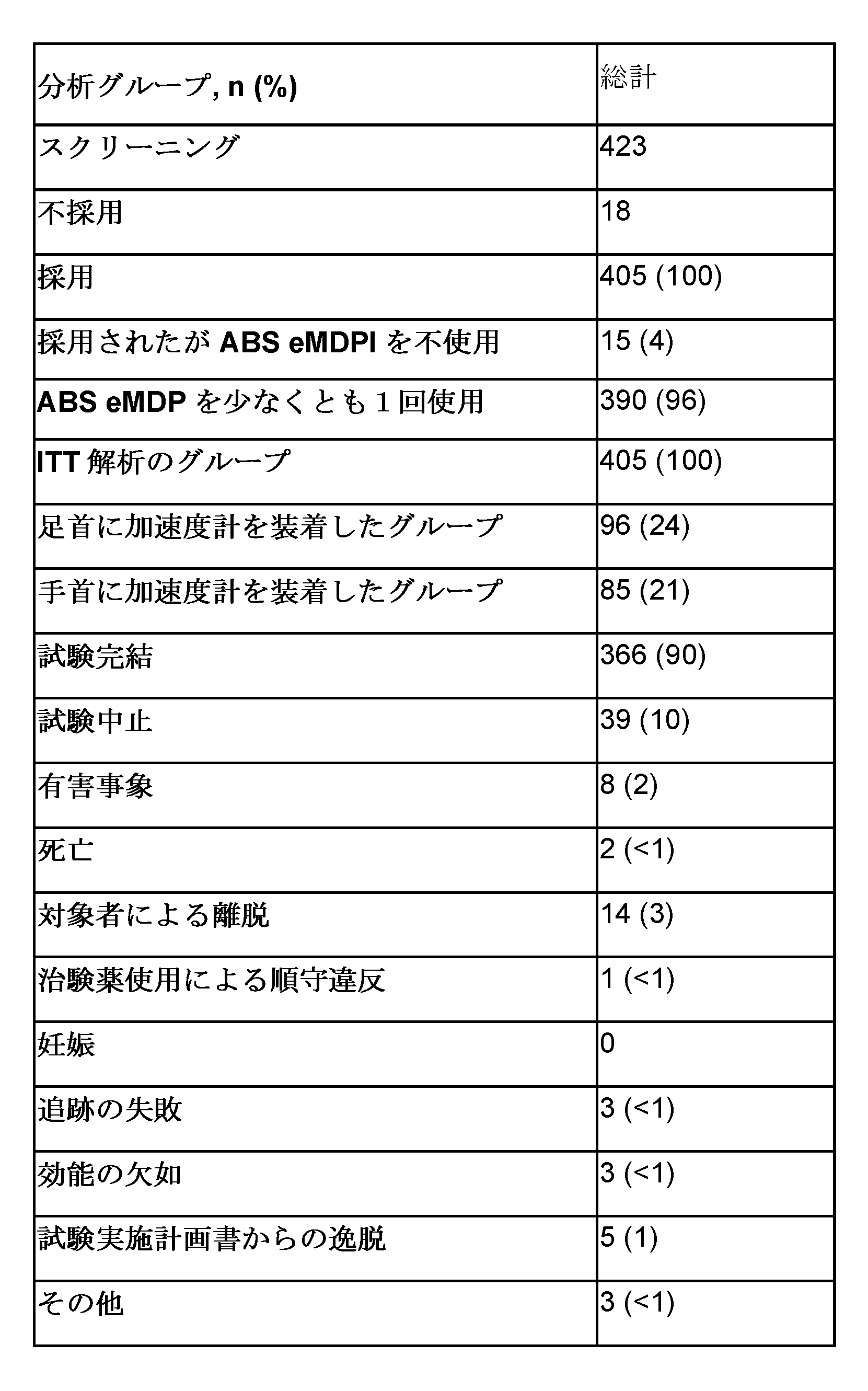
試験を終えた98人の患者がAECOPDの事象を経験し、ディジハラーを使用した。総数で121例の並みの/重大なAECOPDの事象が記録された。さらなる詳細が表4に示されている。 Ninety-eight patients who completed the study experienced an event of AECOPD and used a digital haller. A total of 121 average / significant AECOPD events were recorded. Further details are shown in Table 4.
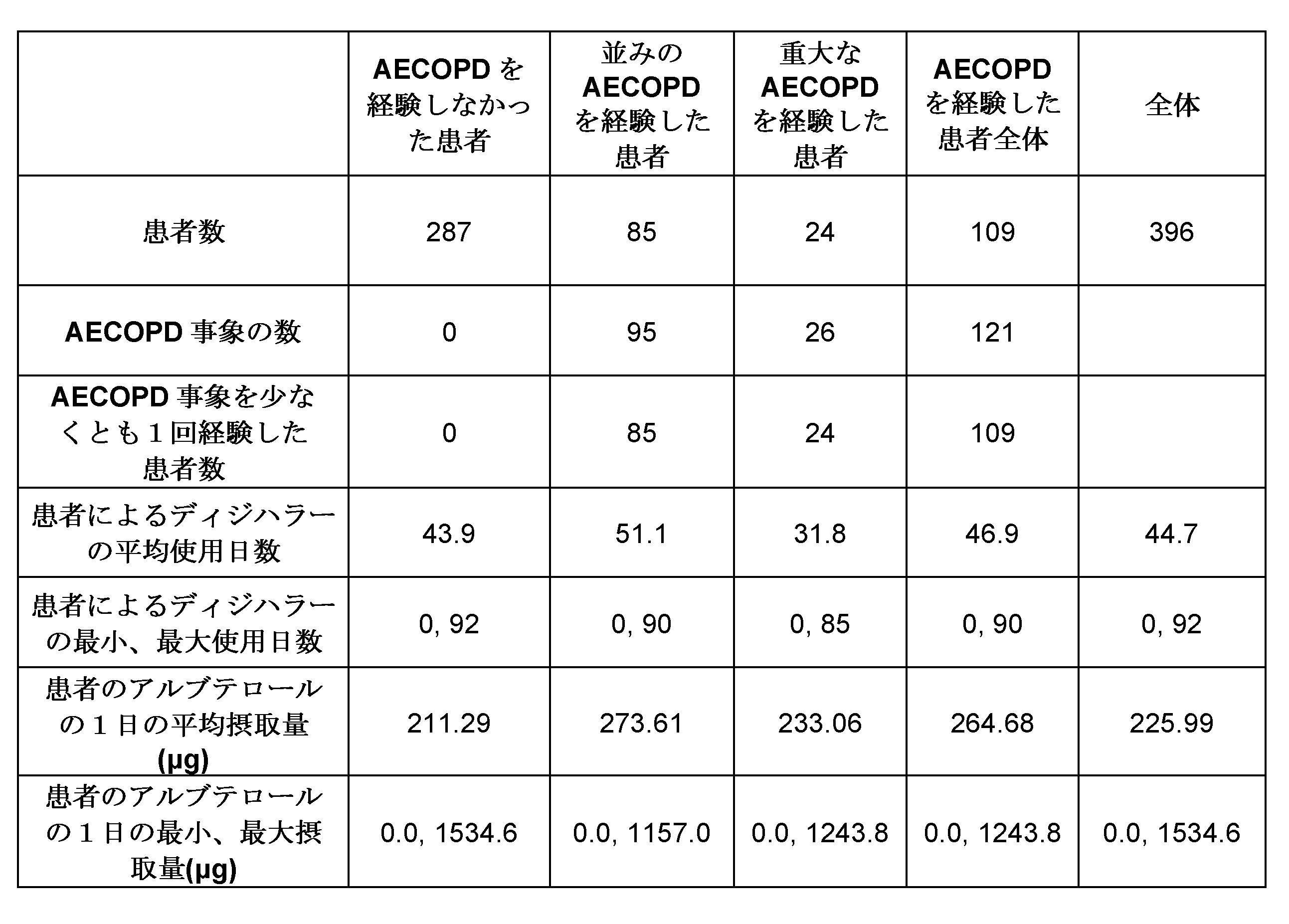
試験を終えた366人の患者について、30人(8%)の患者は吸入器を全く使用せず、268人(73%)の患者は1日平均5回まで吸入を行い、11人(3%)の患者は1日平均10回以上吸入を行った。 Of the 366 patients who completed the study, 30 (8%) did not use the inhaler at all, and 268 (73%) inhaled up to an average of 5 times a day, 11 (3). %) Patients inhaled 10 times or more a day on average.
図9は、対象者1人当たりの救急吸入の平均回数対COPDの増悪からの日数のグラフ30bである。図9は、増悪が発生した日の前後14日間のリスク期間内のデータを示している。直線32bはリスク期間内の救急吸入の1日の平均回数に対応する。直線32bは、直線34bによって表された、基準となるリスク期間外の救急吸入の1日の平均回数よりもY軸上のより高い位置にある。これは、増悪のリスクが高まるにつれて救急吸入の1日の平均回数が増加することを表している。参照のために、図9には、さらに、直線36bによって表された、基準となる増悪を経験しなかった患者の救急吸入の1日の平均回数が示されている。
FIG. 9 is a
図10は、対象者1人当たりの救急吸入の平均回数対COPDの増悪からの日数の別のグラフ30bである。図10は、増悪が発生した日の前後30日間のリスク期間内のデータを示している。図10は、直線34bによって表された、基準となるリスク期間外の救急吸入の1日の平均回数と比較して、増悪の発生の日が近づくにつれて、救急吸入器の使用回数が顕著に増加することを示している。
FIG. 10 is another
データは、増悪の発生に先立つ約2週間の間に救急薬の吸入の回数が増加することを示している。増悪の発生に先立つ約1週間の間は増加率は小さい。表5は、増加した救急薬の使用回数とAECOPDとの関連性に関するさらなる詳細を示している。 The data show that the number of emergency drug inhalations increases during the approximately two weeks prior to the onset of exacerbations. The rate of increase is small for about a week prior to the onset of exacerbations. Table 5 shows further details regarding the association between increased number of first aid use and AECOPD.

[1]AECOPD事象を経験した患者について、アルブテロールの使用が、事象の症状の最大に達する前になされる。複数回の事象を経験した患者について、第1回目の事象のみが分析に含まれている。基準となるアルブテロールの使用は試験の最初の7日間の吸入の平均回数として規定されている。この最初の7日間に吸入が行われなかった場合、当該7日後の最初の利用可能な吸入が用いられる。試験期間中に全く吸入が行われなかった場合、基準値はゼロとなる。
[2]推測統計学のすべて、オッズ比、p値、および適合度に対するC統計量が、ロジスティック回帰モデルから増加するアルブテロール使用回数および基準となるアルブテロールの使用回数を用いて、試験変数として計算される。1よりも大きいオッズ比は、日常的なアルブテロールの使用が基準値を20%も超えている患者は、日常的なアルブテロールの使用が基準値を20%も超えない患者よりもAECOPDの事象を経験する可能性が高いことを示す。試験の1日目~7日目の間にAECOPDを経験した患者は分析から除外されている。
[1] For patients who have experienced an AECOPD event, the use of albuterol is made before the maximum symptom of the event is reached. For patients who have experienced multiple events, only the first event is included in the analysis. The standard use of albuterol is defined as the average number of inhalations during the first 7 days of the study. If no inhalation is made during this first 7 days, the first available inhalation after the 7 days is used. If no inhalation is performed during the test period, the reference value will be zero.
[2] All of the inference statistics, odds ratios, p-values, and C-statistics for goodness of fit are calculated as test variables using the increasing number of albuterol usages and reference albuterol usages from the logistic regression model. To. Odds ratios greater than 1 are such that patients with routine albuterol use exceeding the reference value by as much as 20% experience AECOPD events more than patients with routine albuterol use not exceeding the reference value by 20%. Indicates that there is a high possibility of doing so. Patients who experienced AECOPD between days 1-7 of the study were excluded from the analysis.
図11は、対象者1人当たりの平均最大吸入流量対COPDの増悪からの日数のグラフ40bである。図11は、増悪の発生日の前後14日間のリスク期間のデータを示している。直線42bは、直線44bによって表された、基準となるリスク期間外の平均最大吸入流量よりもY軸上においてわずかに高い位置にあるが、この差はあまり重要ではないと思われる。図11には、さらに、直線46bによって表された、基準となる増悪を経験しなかった患者に関する平均最大吸入流量が示されている。
FIG. 11 is a
図12は、対象者1人当たりの平均最大吸入流量対COPDの増悪からの日数の別のグラフ60bである。図12は、増悪の発生日の前後30日間のデータを示している。図12は、増悪の発生前の、比較的安定した、低い平均最大吸入流量を示している。
FIG. 12 is another
図13は、対象者1人当たりの平均吸入量対COPDの増悪からの日数のグラフ60bである。図13は、増悪の発生日の前後14日のリスク期間内のデータを示している。直線62bは、リスク期間内の平均吸入量に対応している。直線62bは、直線64bによって表された、基準となるリスク期間内の平均吸入量よりもY軸上のより低い位置にある。図13には、さらに、直線66bによって表された、基準となる増悪を経験しなかった対象者に関する平均吸入量が示されている。
FIG. 13 is a
図14は、対象者1人当たりの平均吸入量対COPDの増悪からの日数の別のグラフ60bである。図14は、増悪の発生日の前後30日の期間のデータを示している。
FIG. 14 is another
図15は、対象者1人当たりの平均吸入継続時間対COPDの増悪からの日数のグラフ70bである。図15は、増悪の発生日の前後14日のリスク期間内のデータを示している。直線72bはリスク期間内の平均吸入継続時間に対応している。直線72bは、直線74bによって表された、基準となるリスク期間外の平均吸入継続時間よりもY軸上の低い位置にある。図15には、さらに、直線76bによって表された、基準となる増悪を経験しなかった対象者に関する平均吸入継続時間が示されている。
FIG. 15 is a
図16は、対象者1人当たりの平均吸入継続時間対COPDの増悪からの日数の別のグラフ70bである。図16は、増悪の発生日の前後30日の期間内のデータを示している。
FIG. 16 is another
図13~図16は、AECOPDの前の吸入量および吸入継続時間の比較的長期間の(約30日間にわたって実証された)直線的な減少を明らかにしている。 13-16 show a relatively long-term (demonstrated over about 30 days) linear reduction in inhalation volume and duration of inhalation prior to AECOPD.
表6は、±14日間のAECOPDの窓の内外における患者に関して記録された吸入パラメータおよび救急薬の吸入回数と、AECOPDを経験しなかった患者に関して記録された吸入パラメータおよび救急薬の吸入回数を比較したものである。 Table 6 compares the inhalation parameters and the number of inhalations of the first aid recorded for patients inside and outside the window of ACECOPD for ± 14 days with the inhalation parameters and the number of inhalations of the first aid recorded for patients who did not experience AECOPD. It was done.
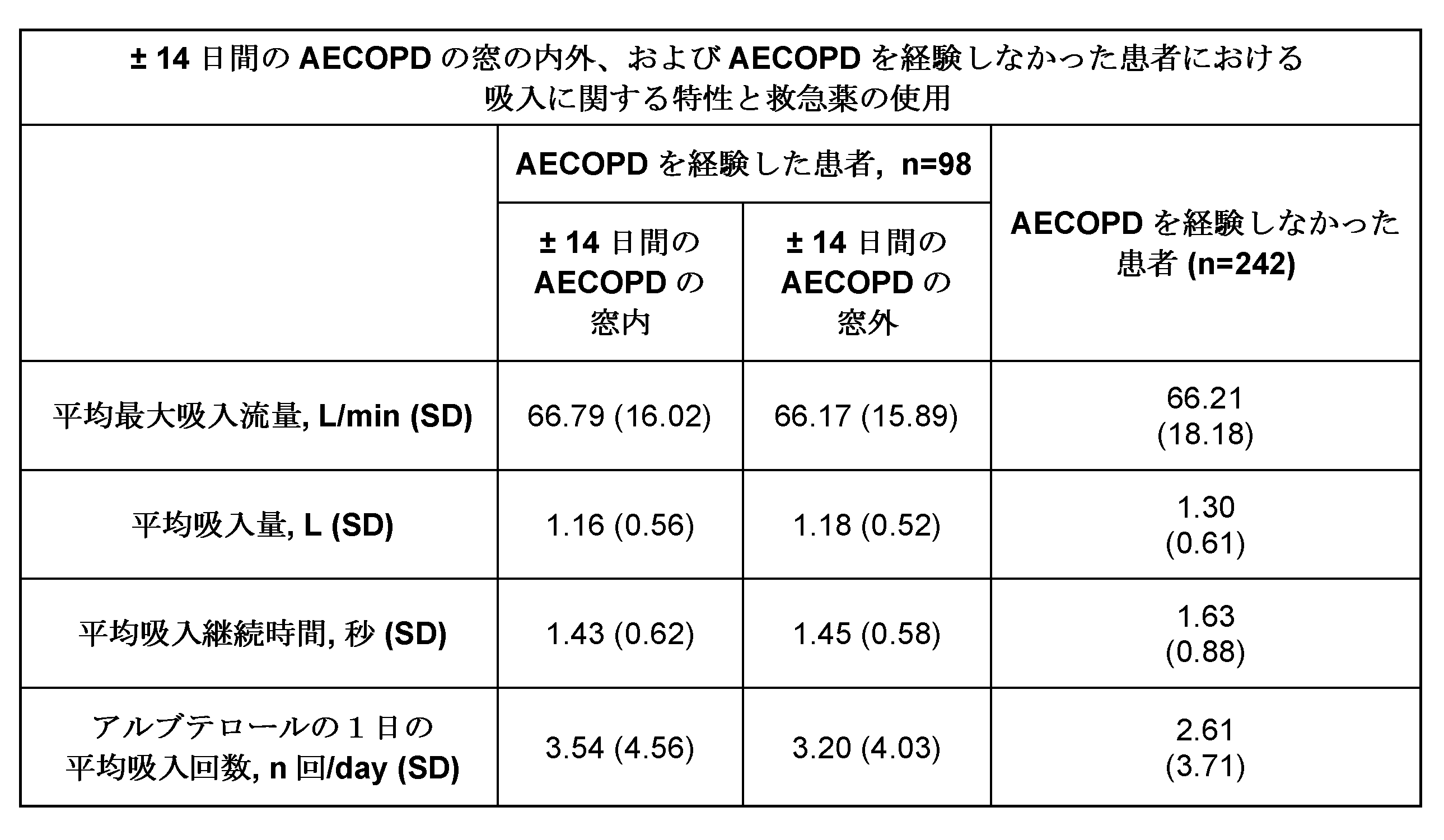
増悪を経験した患者に関する基準となる1日のアルブテロール平均吸入回数は、増悪を経験しなかった患者の場合に比べてわずかに高くなり、増悪を経験した患者に関する基準となる平均吸入量および吸入継続時間は、増悪を経験しなかった患者の場合に比べてわずかに低くなった。±14日間のAECOPDの窓内において、患者は、基準値(±14日間のAECOPDの窓の外)よりも、またAECOPDを経験しなかった患者と比べても、1日のアルブテロール平均吸入回数が多くなった。 The standard daily average number of inhalations of albuterol for patients who experienced exacerbations was slightly higher than for patients who did not experience exacerbations, and the standard average inhalation volume and continued inhalation for patients who experienced exacerbations. The time was slightly lower than in patients who did not experience exacerbations. Within the ± 14-day AECOPD window, patients had an average number of albuterol inhalations per day above reference values (outside the ± 14-day AECOPD window) and even compared to patients who did not experience AECOPD. It became more.
上で説明された喘息の増悪に対する予測モデルとは対照的に、COPDの増悪の最も強い予測因子は、気流に関するパラメータ、例えば、最大吸入流量および/または吸入量および/または吸入継続時間であることがわかった。また、救急吸入の回数は有意な予測値を含んでいることがわかった。 In contrast to the predictive model for asthma exacerbations described above, the strongest predictors of COPD exacerbations are airflow parameters such as maximum inhalation flow rate and / or inhalation volume and / or inhalation duration. I understand. It was also found that the number of emergency inhalations included a significant predicted value.
上の結果に基づき、重みづけされたモデルが、COPDの増悪の確率を計算するために発展せしめられた。教師あり機械学習技術、勾配ブースティング(Gradient Boosting Trees)が分類問題(今後x日間でCOPDの増悪が発生するか否か(増悪期間))を解決するために使用された。 Based on the above results, a weighted model was developed to calculate the probability of exacerbation of COPD. A supervised machine learning technique, Gradient Boosting Trees, was used to solve the classification problem (whether COPD exacerbations will occur in the next x days (exacerbation period)).
表7は、重みづけされたモデルに含まれる因子の例示的なリストを、それらの相互の相対的な重みづけとともに示している。 Table 7 shows an exemplary list of factors contained in the weighted model, along with their relative weighting to each other.
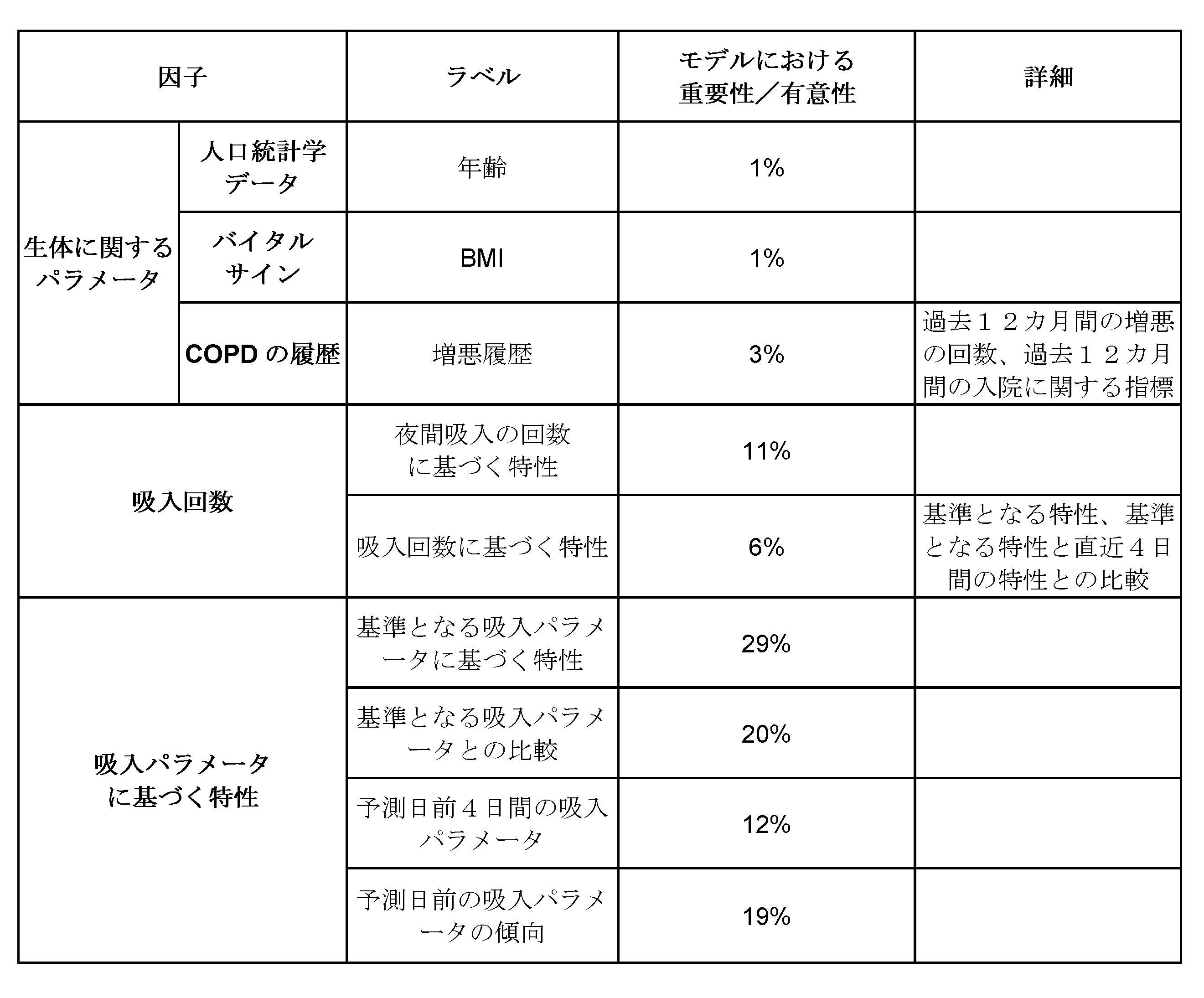
一般化されたモデルは、受信者動作特性(ROC)曲線解析によって評価された。切迫したCOPDの増悪の確率を計算するための予測モデルにおける最も有意な因子は、吸入パラメータであるが、予測モデルは、これに救急吸入の回数に関するデータを補うことによってより確かなものとなった。
図17は、モデルの受信者動作特性(ROC)曲線解析を示しており、偽陽性率に対する真陽性率をプロットすることによってモデルの質を評価している。このモデルは、ROC曲線下の面積(AUC)の値0.77を伴うその後の5日間の切迫した増悪を予測した。
The generalized model was evaluated by receiver operating characteristic (ROC) curve analysis. The most significant factor in the predictive model for calculating the probability of an imminent exacerbation of COPD is the inhalation parameter, which was further confirmed by supplementing this with data on the number of emergency inhalations. ..
FIG. 17 shows a receiver operating characteristic (ROC) curve analysis of the model, assessing the quality of the model by plotting the true positive rate against the false positive rate. This model predicted an imminent exacerbation for the next 5 days with an area under the ROC curve (AUC) value of 0.77.
COPDの増悪を予測する場合、救急吸入の回数は、吸入パラメータよりも確率の全体に及ぼす影響が小さいにもかかわらず、増悪の確率計算の精度を上げる際の有意な因子である。 When predicting exacerbations of COPD, the number of emergency inhalations is a significant factor in improving the accuracy of the probability calculation of exacerbations, even though it has a smaller effect on overall probability than inhalation parameters.
図18~図22はシステム10に含まれた吸入器の非限定的な例を示している。
18-22 show non-limiting examples of inhalers included in
図18は、非限定的な例に係る第1の吸入器100の斜視図である。吸入器100は、例えば自己吸入式吸入器である。吸入器100は、上部キャップ102、メインハウジング104および/またはマウスピース106および/またはマウスピースカバー108および/または電子モジュール120および/または換気口126を有している。マウスピースカバー108は蝶番によってメインハウジング104に結合され、マウスピースカバーの開閉によってマウスピース106が露出しまたは収納されるようになっている。この例では蝶番による結合が用いられるが、マウスピースカバー108は別の形式の結合によっても吸入器100に結合され得る。さらに、この例では、電子モジュール120がメインハウジング104の上部において上部キャップ102内に収容されているが、電子モジュール120は、吸入器100のメインハウジング104と一体化されおよび/またはメインハウジング104の内部に収容されてもよい。
FIG. 18 is a perspective view of the
図19は、図18に示した吸入器100の縦断面図である。吸入器100は、メインハウジング104の内側に、薬剤タンク110(例えば、ホッパー)、ベローズ112、ベローズスプリング114、ヨーク(図示されない)、投薬カップ116、投薬チャンバ117、解砕器121および流路119を有している。薬剤タンク110は、対象者に投与するための、ドライパウダー薬剤等の薬剤を有している。マウスピースカバー108が閉位置から開位置まで動かされたとき、ベローズ112が薬剤タンクから1回分の薬剤を投薬カップ116に供給する。その後、対象者は、マウスピース106を通じて吸入を行い、1回分の薬剤を吸引する。
FIG. 19 is a vertical sectional view of the
対象者の吸入によって生じた気流によって、解砕器121は、投薬カップ116内の薬剤の凝集体を粉砕することによって1回部の薬剤をエアロゾル化する。解砕器121は、流路119を通る気流が特定の速度に達しまたはこれを超えたとき、または特定の範囲内の速度を有するとき、薬剤をエアロゾル化するように構成されている。エアロゾル化されたとき、1回分の薬剤は投薬カップ116から流路119を通って投薬チャンバ117内に流入し、その後、マウスピース106から対象者に供給される。流路119を通る気流が特定の速度に達しないかまたはそれを超えず、あるいは速度が特定の範囲内にないとき、薬剤は投薬カップ116内に残ったままとなる。投薬カップ116内の薬剤が解砕器121によってエアロゾル化されなかった場合、マウスピースカバー108がその後に開放されたときに薬剤の次の1回分は薬剤タンク110から供給されない。すなわち、1回分の薬剤が解砕器121によってエアロゾル化されるまで当該1回分の薬剤は投薬カップ内に残ったままとなる。1回分の薬剤が投与されたとき、投薬が行われたことの確認が吸入器100において、投薬確認情報としてメモリに記憶される。
The airflow generated by the subject's inhalation causes the
対象者がマウスピース106を通じて吸入しているとき、空気が換気口から進入し、薬剤を対象者に供給するための気流が発生する。流路119は投薬チャンバ117からマウスピース106の端までのび、投薬チャンバ117およびマウスピース106の内側部分を含んでいる。投薬カップ116は、投薬チャンバ117の内部にありまたはこれに隣接している。さらに、吸入器100は、最初、薬剤タンク110内の薬剤の総投薬回数がセットされ、マウスピースカバー108が閉位置から開位置まで動かされるたびに当該総投薬回数から1回ずつ減じられるように構成された投薬回数カウンタ111を有している。
When the subject is inhaling through the
上部キャップ102はメインハウジング104に取り付けられている。上部キャップ102は、例えば、メインハウジング104の凹部に係合し得る1または2以上のクリップを用いてメインハウジング104に取り付けられている。上部キャップ102は、結合されたとき、メインハウジング104の一部と重なり合い、例えば、上部キャップ102とメインハウジング104の間に実質的な気密シールが生じるようになっている。
The
図20は、図18に示した吸入器100の分解斜視図であり、上部キャップ102が取り外されて電子モジュール120が露出した状態を示した図である。図20に示されるように、メインハウジング104の上面は1または2以上(例えば2つ)のオリフィス146を有している。1つのオリフィス146はスライダ140を受け入れ可能に構成されている。例えば、上部キャップ102がメインハウジング104に取り付けられたとき、スライダ140が1つのオリフィス146を通ってメインハウジング104の上面から突出する。
FIG. 20 is an exploded perspective view of the
図21は、図18に示した吸入器100の上部キャップ102および電子モジュールの分解斜視図である。図21に示されるように、スライダ140は、腕142、ストッパ144および遠位端145を形成している。遠位端145はスライダ140の底部を形成している。スライダ140の遠位端145は、(例えば、マウスピースカバー108が閉位置または部分的に開位置にあるとき)メインハウジング104の内部にあるヨークに当接するように構成されている。遠位端145は、ヨークが半径方向のいずれかにあるとき、ヨークの上面にに当接するように構成されている。例えば、ヨークの上面は複数のアパーチャ(図示されない)を有し、スライダ140の遠位端145は、例えば、1つのアパーチャがスライダ140と1列に並ぶかどうかにかかわらず、ヨークの上面に当接するように構成されている。
FIG. 21 is an exploded perspective view of the
上部キャップ102は、スライダースプリング146およびスライダー140を受けるように構成されたスライダガイド148を有している。スライダスプリング146はスライダガイド内部に位置している。スライダスプリング146は、上部キャップ102の内面に係合し、スライダ140の上部(例えば、近位端)に係合する。スライダ140がスライダガイド148の内部に配置されるとき、スライダスプリング146はスライダ140の上部と上部キャップ102の内面との間において部分的に圧縮される。例えば、スライダスプリング146は、マウスピースカバー108が閉じられているとき、スライダ140の遠位端145がヨークに接触しているように構成されている。スライダ145の遠位端145は、また、マウスピースカバー108が開かれまたは閉じられている間、ヨークに接触しているように構成される。スライダ140のストッパー144は、スライダガイド148に対し、例えば、スライダ140がマウスピースカバー108の開閉またはその逆を通してスライダガイド148内に保持されるように係合している。ストッパー144およびスライダガイド148は、スライダ140の上下方向(例えば軸方向)の運動を制限するように構成されている。この制限された運動距離は、ヨークの上下方向の運動の制限距離よりも短い。すなわち、マウスピースカバー108が完全に開いた位置まで動かされるとき、ヨークは上下方向にマウスピース106に向けて動き続けるが、ストッパー144がスライダ140の上下方向の運動を制止し、それによって、スライダ140の遠位端145はもはやヨークに接触しなくなる。
The
より一般的には、ヨークはマウスピースカバー108に機械的に結合されていて、マウスピースカバー108が閉位置から開かれるときにベローズスプリングを圧縮し、その後、マウスピースカバー108が開位置に達したときに当該圧縮されたベローズスプリング114を開放し、それによって、ベローズ112に1回分の薬剤を薬剤タンク110から投薬カップ116に供給させるように構成されている。ヨークは、マウスピースカバー108が閉位置にあるとき、スライダ140に接触している。スライダ140は、マウスピースカバー108が閉位置から開かれるとき、ヨークによって動かされ、マウスピースカバー108が完全に開いた位置をとるとき、ヨークから離されるように設けられている。この構成は、上で既に説明された計量アッセンブリーの非限定的な例とみなされる。なぜなら、マウスピースカバー108が開かれることによって、薬剤の1回分の計量がなされるからである。
More generally, the yoke is mechanically coupled to the
薬剤の計量の間のスライダ140の運動によって、スライダ140はスイッチ130に係合してスイッチ130を作動させる。スイッチ130は、電子モジュール120を起動し、薬剤の計量を記録させる。スライダ140およびスイッチ130は、電子モジュール120とともに、上で説明された使用検出システム12Bの非限定的な例に対応している。この例において、スライダ140は、それによって使用検出システム12Bが計量アッセンブリーによる1回分の薬剤の計量を記録するように構成される手段とみなされ、それによる各計量は対象者が吸入器100を用いて行った吸入を表す。
The movement of the
スライダ140によるスイッチ130の作動によって、例えば、電子モジュール120が第1の電力状態から第2の電力状態に遷移し、対象者によるマウスピース108からの吸入を検出する。
By operating the
電子モジュール120は、プリント回路基板(PCB)アッセンブリー122および/またはスイッチ130および/または電源(例えば、電池126)および/または電池ホルダー124を有している。PCBアッセンブリー122は、センサーシステム128および/または無線通信回路129および/またはスイッチ130および/または、1または2以上の発光ダイオード(LED)のような(図示されない)インディケータ等の表面実装部品を有している。電子モジュール120は、コントローラ(例えば、プロセッサー)および/またはメモリを有している。コントローラおよび/またはメモリは、PCB122の部品とは物理的に異なる。あるいは、コントローラおよびメモリは、PCB122に実装された別のチップセットの一部からなり、例えば、無線通信回路129は電子モジュール120に対するコントローラおよび/またはメモリを含んでいる。電子モジュール120のコントローラは、マイクロコントローラ、プログラマブルロジックデバイス(PLD)、マイクロプロセッサー、アプリケーションスペシフィックインテグレイティッドサーキット(ASIC)、フィールドプログラマブルゲートアレイ(FPGA)または任意の適当な処理装置またはコントロール回路を含んでいる。
The
コントローラは、メモリからデータを読み出し、メモリにデータを記録する。メモリは、取り外し不可能なメモリおよび/または取り外し可能なメモリのような、任意の形式の適当なメモリを含んでいる。取り外し不可能なメモリは、ランダムアクセスメモリ(RAM)、読み出し専用メモリ(ROM)、ハードディスク、またはその他の任意の形式の記憶装置を含んでいる。取り外し可能なメモリは、加入者IDモジュール(SIM)カード、メモリスティック、セキュアディジタル(CD)メモリカードおよびそれらに類するものを含んでいる。メモリは、コントローラの内部に配置される。コントローラは、また、サーバまたはスマートフォン上等の、電子モジュール120の内部には物理的に配置されないメモリからデータを読み出し、それにデータを記録する。
The controller reads the data from the memory and records the data in the memory. Memory includes any form of suitable memory, such as non-removable memory and / or removable memory. Non-removable memory includes random access memory (RAM), read-only memory (ROM), hard disk, or any other form of storage. Removable memory includes subscriber ID module (SIM) cards, memory sticks, secure digital (CD) memory cards and the like. The memory is located inside the controller. The controller also reads data from a memory that is not physically located inside the
センサーシステム128は、1または2以上のセンサーを有している。センサーシステム128はセンサーシステム12Aの1例である。センサーシステム128は、例えば、1または2以上の圧力センサーおよび/または温度センサーおよび/または湿度センサーおよび/または方向センサーおよび/または音響センサーおよび/または光学センサー等の1または2以上の異なる形式のセンサーを有している。1または2以上の圧力センサーは、気圧センサー(例えば、大気圧センサー)および/または差圧センサーおよび/または絶対圧センサーおよび/またはそれらに類するものを含んでいる。センサーは、微小電気機械システム(MEMS)および/またはナノ電気機械システム(NEMS)の技術を使用する。センサーシステム128は、電子モジュール120のコントローラに対し、瞬間的な測定値(例えば、圧力測定値)および/または一定時間にわたって集計された測定値(例えば、圧力測定値)を与えるように構成されている。図19および図20に示されるように、センサーシステム128は、吸入器100の流路119の外部に配置されるが、流路と空気圧的に結合されている。
The
電子モジュール120のコントローラは、センサーシステム128から測定値に対応する信号を受信する。コントローラは、センサーシステム128から受信した信号を用いて気流に関するメトリックスを計算し、または決定する。気流に関するメトリックスは、吸入器100の流路119を通る気流のプロファイルを表す。例えば、センサーシステム128が0.3キロパスカル(kPa)の気圧変化を記録したとき、電子モジュール120は、その気圧変化が流路119を通じた約45リットル/分(Lpm)の空気流量に対応していると計算する。
The controller of the
図22は、空気流量対圧力のグラフである。図22に示された空気流量およびプロファイルは単なる例示であり、計算された速度は、吸入器100およびその部品のサイズ、形状およびデザインに依存する。
FIG. 22 is a graph of air flow rate vs. pressure. The air flow rate and profile shown in FIG. 22 are merely exemplary, and the calculated speed depends on the size, shape and design of the
電子モジュール120のコントローラは、センサーシステム128から受信した信号および/または計算された気流に関するメトリックスを1または2以上の閾値または数値範囲と比較することによって、リアルタイムでのパーソナライズされたデータを、吸入器100がどのように使用されたのか、および/またはその使用が結果として薬剤の完全な投与を生じる可能性があるかどうかに関する評価の一部として生成する。例えば、計算された気流に関するメトリックスが特定の閾値より低い空気流量を伴った吸入に対応するとき、電子モジュール120は、吸入器100のマウスピース106からの吸入が全くないか、または当該マウスピース106からの吸入が不十分であると判定する。また、計算された気流に関するメトリックスが特定の閾値を超える空気流量を伴った吸入に対応するとき、電子モジュール120は、吸入器100のマウスピース106からの吸入が過剰であると判定する。また、計算された気流に関するメトリックスが特定の範囲内にある空気流量を伴った吸入に対応するとき、電子モジュール120は、吸入が良好であると、あるいは、結果的に完全な投薬が生じた可能性があると判定する。
The controller of the
圧力測定値および/または計算された気流に関するメトリックスは、吸入器100からの吸入の質または強さを表す。例えば、特定の閾値または数値範囲と比較されたとき、測定値および/またはメトリックスは、関係する吸入を、良好吸入事象、低吸入事象、無吸入事象または過剰吸入事象等の一定の事象タイプに分類するために使用される。吸入の分類は、対象者のパーソナライズされたデータとして記録された有益なパラメータである。
Pressure measurements and / or calculated airflow metrics represent the quality or intensity of inhalation from the
無吸入事象は、30Lpmより小さい空気流量等の、特定の閾値より低い圧力測定値および/または気流に関するメトリックスに関係づけられる。無吸入事象は、対象者が、マウスピースカバー108を開いた後であって測定サイクルの間に、マウスピース106から吸入を行わなかったときに生じる。また、無吸入事象は、対象者による吸入が、解砕器121を作動させる、すなわち投薬カップ116内で薬剤をエアロゾル化するのには不十分な気流しか発生させられなかったとき等の、対象者の吸入が流路119を通じた薬剤の適切な投与を保証するのには不十分であるときに生じる。
Non-inhalation events are associated with pressure measurements and / or airflow metrics below a certain threshold, such as air flow below 30 Lpm. The non-inhalation event occurs when the subject does not inhale from the
低吸入事象は、30Lpm~45Lpm等の特定の数値範囲内にある圧力測定値および/または気流に関するメトリックスに関係づけられる。低吸入事象は、対象者がマウスピースカバー108を開いた後にマウスピース106から吸入を行い、対象者の吸入によっても、1回分の薬剤のうちの少なくとも1部のみが流路119を通じて投与されただけであるときに生じる。すなわち、吸入は、解砕器121を作動させて少なくとも1部の薬剤を投薬カップ116からエアロゾル化するのには不十分である。
Low inhalation events are associated with pressure measurements and / or airflow metrics within a certain numerical range, such as 30 Lpm to 45 Lpm. In the low inhalation event, the subject inhaled from the
良好吸入事象は、45Lpm~200Lpm等の低吸入事象より上の圧力測定値および/または気流に関するメトリックスに関係づけられる。良好吸入事象は、対象者がマウスピースカバー108を開いた後にマウスピース106から吸入を行い、対象者の努力によって、解砕器121を作動させて投与カップ116内において1回分の薬剤の全てをエアロゾル化するのに十分な気流を発生させたとき等の、対象者の努力によって、流路119を通じた薬剤の適切な投与が保証されるのに十分な吸入がなされたときに生じる。
Good inhalation events are associated with pressure measurements and / or airflow metrics above low inhalation events such as 45 Lpm to 200 Lpm. In a good inhalation event, the subject inhales from the
過剰吸入事象は、200Lpmを超える空気流量等の、良好吸入事象より上の圧力測定値および/または気流に関するメトリックスに関係づけられる。過剰吸入事象は、対象者が吸入器100の正常な作動パラメータを超えた吸入を行ったときに生じる。過剰吸入事象は、また、たとえ対象者が正常な範囲内の吸入を行ったとしても、吸入器100が使用中に適切な位置に配置または保持されていないときにも生じる。例えば、計算された空気流量は、対象者がマウスピース106から吸入を行っている間に、(例えば、1本の指または親指によって)換気口が塞がれまたは遮られたときに200Lpmを超える。
Excessive inhalation events are associated with pressure measurements and / or airflow metrics above good inhalation events, such as air flow rates above 200 Lpm. The over-inhalation event occurs when the subject inhales beyond the normal operating parameters of the
任意の適当な閾値または数値範囲が特定の事象を分類するために使用される。いくつかの事象またはすべての事象が使用される。例えば、無吸入事象は45Lpmより低い空気流量に関係づけられ、良好吸入事象は45Lpm~200Lpmの範囲内の空気流量に関係づけられる。よって、低吸入事象は、場合によっては、全く使用されない。 Any suitable threshold or numerical range is used to classify a particular event. Some or all events are used. For example, a non-inhalation event is associated with an air flow rate below 45 Lpm, and a good inhalation event is associated with an air flow rate in the range of 45 Lpm to 200 Lpm. Therefore, low inhalation events may not be used at all.
圧力測定値および/または計算された気流に関するメトリックスは、また、吸入器100の流路119を通じた気流の向きも表す。例えば、圧力測定値が負の圧力変化を反映するとき、圧力測定値は流路119を通じてマウスピース106から出ていく気流を表す。圧力測定値が正の圧力変化を反映するとき、圧力測定値は流路119を通じてマウスピース106内に入ってくる気流を表す。したがって、圧力測定値および/または気流に関するメトリックスは、対象者がマウスピース106内に空気を吐き出しているかどうかを判定するために使用され、それによって、対象者が吸入器100を正しく使用していないことを知らせる。
The pressure measurements and / or the calculated airflow metrics also represent the direction of the airflow through the
吸入器100は、肺機能に関するメトリックスの測定を可能にするための肺活量計またはそれに類似の動作をする装置を有している。例えば、吸入器100は、対象者の肺活量に関係するメトリックスを得るための測定を行う。肺活量計またはそれに類似の動作をする装置は対象者によって吸引されおよび/または吐き出された空気の体積を測定する。歯活量計またはそれに類似の動作をする装置は、圧力トランスデューサー、超音波または水位計を使用して吸引されたおよび/または吐き出された空気の体積の変化を検出する。
The
吸入器100の使用から収集された、または吸入器100の使用に基づいて計算されたパーソナライズされたデータ(例えば、圧力に関するメトリックス、気流に関するメトリックス、肺機能に関するメトリックス、投薬確認情報等々)は、さらに、(部分的にまたは全体的に)外部装置によって計算されおよび/または評価される。
より一般的には、電子モジュール120の無線通信回路129は、送信器および/または受信器(例えば、トランシーバー)だけでなく付加的な電気回路もまた有している。例えば、無線通信回路129は、ブルートゥースチップセット(例えば、ブルートゥース低電力チップセット)、ジグビーチップセット、スレッドチップセット等々を有している。よって、電子モジュール120は、圧力測定値および/または気流に関するメトリックスおよび/または肺機能に関するメトリックスおよび/または投薬確認情報および/または吸入器100の使用に関するその他の状況等のパーソナライズされたデータを、スマートフォンを含む外部装置に対し無線で提供する。パーソナライズされたデータは外部装置に対しリアルタイムで提供され、それによって、吸入器100からの、使用回数および吸入器100がどのように使用されたのかをを示すリアルタイムデータ、および対象者の肺機能および/または治療に関するリアルタイムデータ等の、吸入器のユーザーに関するパーソナライズされたデータに基づいて、増悪リスクの予測をすることが可能となる。外部装置は、受信した情報を処理し、吸入器100のユーザーに対してグラフィックユーザーインターフェイス(GUI)を介して順守フィードバックを提供するためのソフトウェアを有している。
Personalized data collected from the use of the
More generally, the
気流に関するメトリックスは、吸入/吐出の平均流量および/または吸入/吐出の最大流量(例えば、受信された最大吸入流量)および/または吸入/吐出量および/または時間対吸入/吐出最大および/または吸入/吐出の継続時間のうちの1または2以上等の、吸入器100からリアルタイムで収集されたパーソナライズされたデータを含んでいる。気流に関するメトリックスは、また、流路119を通る気流の向きを表す。すなわち、負の圧力変化はマウスピース106からの吸入に対応する一方、正の圧力変化はマウスピース106への吐き出しに対応する。気流に関するメトリックスの計算に際し、電子モジュール120は、環境条件によって引き起こされる歪みを除去しまたは最小限にするように構成される。例えば、電子モジュール120は、気流に関するメトリックスを計算する前または計算した後、大気圧の変化を考慮に入れるための計算を行う。1または2以上の圧力測定値および/または気流に関するメトリックスは、タイムスタンプを押された後、電子モジュール120のメモリに記録される
Airflow metrics include average inhalation / discharge flow and / or maximum inhalation / discharge flow (eg, maximum inhalation flow received) and / or inhalation / discharge volume and / or time vs. inhalation / discharge maximum and / or inhalation. / Contains personalized data collected in real time from the
気流に関するメトリックスに加えて、吸入器100または別の計算装置は、気流に関するメトリックスを用いて付加的なパーソナライズされたデータを生成する。例えば、吸入器100の電子モジュール120のコントローラは、気流に関するメトリックスを、例えば、最大吸気流量および/または最大呼気流量および/または1秒間努力呼気肺活量(FEV1)等の医療パラメータであると解される対象者の肺機能および/または肺の健康を表す他のメトリックスに翻訳する。吸入器100の電子モジュール120は、回帰モデル等の数学的モデルを用いて対象者の肺機能および/または肺の健康の尺度を計算する。数学的モデルは、全吸入量およびFEV1間の相関関係を特定する。数学的モデルは、最大吸入流量およびFEV1間の相関関係を特定する。数学的モデルは、全吸入量および最大呼気流量間の相関関係を特定する。数学的モデルは、最大吸入流量および最大呼気流量間の相関関係を特定する。
In addition to the airflow metrics, the
電池126はPCB122の部品に電力を供給する。電池126は、例えば、コイン電池等の、電子モジュール120に電力を供給するための任意の適当な電源からなっている。電池126は再充電可能または再充電不可能である。電池126はバッテリーホルダー124内に収納されている。バッテリーホルダー124はPCB122に取り付けられ、電池126が持続的にPCB122に接触するようにおよび/またはPCB122の部品に電気的に接触するようになっている。電池126は、電池126の寿命に影響を及ぼす特定のバッテリー容量を有している。以下にさらに説明するように、電池126からPCB122の1または2以上の部品への電力の分配は、電池126が吸入器100の耐用年数および/またはその内部に含まれた薬剤の有効期間にわたって電子モジュール120に電力供給を行うことが保証されるように管理される。
The
接続された状態で、通信回路およびメモリが電源オンされ、電子モジュール120は、スマートフォン等の外部装置とペアリングされる。コントローラはメモリからデータを検索し、そのデータを外部装置に対し無線で送信する。コントローラはメモリに最新に記憶されたデータを検索し、送信する。コントローラは、また、メモリに最新に記憶されたデータの一部を検索し、送信する。例えば、コントローラはデータのどの部分が既に外部装置に送信されでいるかを判定し、次いで、まだ送信されていないデータの部分を送信することができる。あるいは、外部装置は、コントローラから、特定の時間の後あるいは外部装置への最新の送信の後に電子モジュール120によって収集されたデータ等の、特定のデータを要求する。コントローラは、もしあれば、メモリからその特定のデータを検索し、検索したデータを外部装置に送信する。
In the connected state, the communication circuit and the memory are turned on, and the
電子モジュール120のメモリに記憶されたデータ(例えば、スイッチによって生成された信号および/またはセンサーシステム128によって取得された圧力測定値および/またはPCB122のコントローラによって計算された気流に関するメトリックス)が外部装置に送信される。外部装置は、そのデータを処理、分析し、吸入器100に関係づけられた有益なパラメータを計算する。さらに、モバイルデバイス上にあるモバイルアプリケーションは、電子モジュール120から受信したデータに基づき、ユーザーに対するフィードバックを生成する。例えば、モバイルアプリケーションは、日報、月報、年報を生成しおよび/またはユーザーに対してエラー事象の確認または通知を行いおよび/またはユーザーに対して有益なフィードバックを提供しおよび/またはそれらと同様のことを行う。
The data stored in the memory of the electronic module 120 (eg, the signal generated by the switch and / or the pressure measurement obtained by the
上で説明された実施例は、本発明の構成を説明するための1例にすぎず、よって本発明の構成を限定するものではない。上で説明された実施例の別の変形例が、当業者によって、本発明の実施において図面、明細書および添付の請求の範囲を研究することからから、理解され、もたらされ得る。特定の手段が互いに異なる引用形式請求項に規定されているという事実は、それらの手段の組み合わせが有利に使用され得ないことを示しているわけではない。 The examples described above are merely examples for explaining the configuration of the present invention, and thus do not limit the configuration of the present invention. Another variation of the embodiments described above can be understood and provided by those skilled in the art from studying the drawings, specification and claims in practice of the present invention. The fact that certain means are set forth in different citation-type claims does not indicate that a combination of those means cannot be used in an advantageous manner.
Claims (23)
前記対象者に救急薬を投与するための第1の吸入器を備え、前記第1の吸入器は前記対象者が前記第1の吸入器を使用することで実行される救急吸入を計測するように構成された使用検出システムを有し、さらに、
定期吸入の間に前記対象者に維持管理薬を投与するための選択的な第2の吸入器と、
前記第2の吸入器が前記システムにおいて使用される場合に、前記第2の吸入器を使用した前記救急吸入および/または前記定期吸入の間に気流に関するパラメータを測定するように構成されたセンサーシステムと、
第1の期間内に前記救急吸入の回数を測定し、少なくとも数回の前記救急および/または前記定期吸入の間の前記パラメータの測定値を受け取り、重みづけされたモデルを用いて、前記救急吸入の回数および前記パラメータの測定値に基づき前記喘息の増悪の確率を計算するように構成されたプロセッサーと、を備え、
前記モデルは、前記救急吸入の回数が前記確率の計算において前記パラメータの測定値よりも有意となるように重みづけされていることを特徴とするシステム。 A system that calculates the probability of exacerbation of asthma in a subject.
A first inhaler for administering the first inhaler to the subject is provided, the first inhaler to measure the emergency inhalation performed by the subject using the first inhaler. Has a use detection system configured in, and also
A second inhaler, selective for administering maintenance medication to the subject during regular inhalation, and
A sensor system configured to measure airflow parameters during the emergency inhalation and / or the periodic inhalation using the second inhaler when the second inhaler is used in the system. When,
The number of such emergency inhalations is measured during the first period, and the measured values of the parameters are received during at least several times of the emergency and / or the periodic inhalations, and the weighted model is used to obtain the emergency inhalation. With a processor configured to calculate the probability of exacerbation of the asthma based on the number of times and the measured values of the parameters.
The model is characterized in that the number of emergency inhalations is weighted to be more significant than the measured value of the parameter in the calculation of the probability.
薬剤タンクと、
前記薬剤タンクから1回分の薬剤を計量するように構成された計量アッセンブリーと、を有し、
前記使用検出システムは、前記計量アッセンブリーによる前記1回分の薬剤の計量を記録するように構成され、それによって、前記1回分の薬剤の計量は前記対象者の前記第1の吸入器の使用によって実行された前記救急吸入を示すことを特徴とする請求項1~請求項11のいずれかに記載のシステム。 The first inhaler is
With the drug tank,
It has a weighing assembly configured to weigh a single dose of the drug from the drug tank.
The use detection system is configured to record the metering of the single dose of the drug by the weighing assembly, whereby the single dose of the drug is performed by the use of the first inhaler of the subject. The system according to any one of claims 1 to 11, wherein the first-aid inhalation is shown.
前記プロセッサーが、前記喘息の増悪の確率を、前記重みづけされたモデルを用いて、前記救急吸入の回数および前記パラメータの測定値および前記入力を受けた前記指標に基づいて計算するように構成されていることを特徴とする請求項1~請求項12のいずれかに記載のシステム。 Further equipped with a user interface for receiving input of an index indicating the pathological condition of the respiratory disease suffered by the subject.
The processor is configured to calculate the probability of exacerbation of the asthma using the weighted model based on the number of emergency inhalations and the measured values of the parameters and the index received. The system according to any one of claims 1 to 12, wherein the system is characterized by the above.
第1の期間内に前記対象者によって実行された救急薬の救急吸入の回数を受け取り、
少なくとも数回の前記救急吸入の間および/または前記対象者によって実行された維持管理薬の定期吸入の間の気流に関するパラメータの測定値を受け取り、
重みづけされたモデルを用いて、前記喘息の増悪の確率を前記救急吸入の回数および前記パラメータの測定値に基づいて決定し、
前記モデルは、前記確率の計算において前記救急吸入の回数が前記パラメータの測定値よりも有意となるように重みづけされていることを特徴とする方法。 A method for calculating the probability of exacerbation of asthma in a subject.
Received the number of first-aid inhalations of the first-aid drug performed by the subject within the first period,
Receives measured values of airflow parameters during at least several such emergency inhalations and / or during routine inhalations of maintenance medication performed by the subject.
Using a weighted model, the probability of exacerbation of the asthma was determined based on the number of emergency inhalations and the measured values of the parameters.
The model is characterized in that the number of emergency inhalations is weighted to be more significant than the measured value of the parameter in the calculation of the probability.
請求項14~請求項16のいずれかに記載の方法を実施し、
前記確率が予め決定された上限に達するかまたは前記上限を超えるかどうかを判定し、あるいは、前記確率が予め決定された下限に達するかまたは前記下限よりも低いかどうかを判定し、
前記上限に達したまたは前記上限を超えた前記確率に基づいて、または前記下限に達したまたは前記下限よりも低くなった前記確率に基づいて前記喘息を治療することを特徴とする方法。 A method of treating an exacerbation of asthma in a subject
The method according to any one of claims 14 to 16 is carried out, and the method is carried out.
Determining whether the probability reaches or exceeds a predetermined upper limit, or determines whether the probability reaches a predetermined lower limit or is lower than the lower limit.
A method comprising treating asthma based on the probability of reaching or exceeding the upper limit, or based on the probability of reaching or lowering the lower limit.
請求項14~請求項16のうちのいずれかに記載の方法を実施し、
前記確率が、前記喘息の増悪を表す予め決定された上限に達するかまたは前記上限を超えるかどうかを判定し、
前記上限に達したまたは前記上限を超えた前記確率に基づいて、前記喘息の増悪を診断することを特徴とする方法。 It ’s a way to diagnose the exacerbation of asthma.
The method according to any one of claims 14 to 16 is carried out, and the method is carried out.
Determining whether the probability reaches or exceeds a predetermined upper limit representing the exacerbation of the asthma.
A method comprising diagnosing an exacerbation of the asthma based on the probability of reaching or exceeding the upper limit.
前記対象者の母集団に属するそれぞれの前記対象者に対して請求項14~請求項16のいずれかに記載の方法を実施し、
それによって、前記母集団に属するそれぞれ前記対象者に対する前記確率を計算し、
前記亜集団に対して計算した前記確率を前記母集団の残りに対して計算した前記確率から区別する確率の閾値または前記確率の範囲を設定し、
前記確率の閾値または前記確率の範囲を用いて前記亜集団を前記母集団の残りから画定することを特徴とする方法。 A method for demarcating subpopulations of subjects
The method according to any one of claims 14 to 16 is carried out for each of the subjects belonging to the population of the subjects.
Thereby, the probability for each of the subjects belonging to the population is calculated.
A threshold of probability or a range of probabilities that distinguishes the probabilities calculated for the subpopulation from the probabilities calculated for the rest of the population is set.
A method comprising defining the subpopulation from the rest of the population using the probability threshold or the range of probabilities.
Applications Claiming Priority (13)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| GB1906078.9 | 2019-04-30 | ||
| GBGB1906078.9A GB201906078D0 (en) | 2019-04-30 | 2019-04-30 | Inhaler system |
| GB1910776.2 | 2019-07-29 | ||
| GBGB1910776.2A GB201910776D0 (en) | 2019-07-29 | 2019-07-29 | Inhaler system |
| GB1919070.1 | 2019-12-20 | ||
| GB1919081.8 | 2019-12-20 | ||
| GB1919076.8 | 2019-12-20 | ||
| GBGB1919076.8A GB201919076D0 (en) | 2019-12-20 | 2019-12-20 | Inhaler system |
| GBGB1919081.8A GB201919081D0 (en) | 2019-12-20 | 2019-12-20 | Inhaler system |
| GBGB1919070.1A GB201919070D0 (en) | 2019-12-20 | 2019-12-20 | Inhaler system |
| GBGB2003534.1A GB202003534D0 (en) | 2020-03-11 | 2020-03-11 | Inhaler system |
| GB2003534.1 | 2020-03-11 | ||
| PCT/IB2020/054056 WO2020222146A1 (en) | 2019-04-30 | 2020-04-30 | Inhaler system |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| JP2022530963A true JP2022530963A (en) | 2022-07-05 |
| JP7664181B2 JP7664181B2 (en) | 2025-04-17 |
Family
ID=70614362
Family Applications (5)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| JP2021564374A Active JP7636345B2 (en) | 2019-04-30 | 2020-04-30 | Inhaler System |
| JP2021564396A Active JP7606469B2 (en) | 2019-04-30 | 2020-04-30 | Inhaler System |
| JP2021564397A Active JP7664181B2 (en) | 2019-04-30 | 2020-04-30 | Inhaler System |
| JP2024218300A Pending JP2025060689A (en) | 2019-04-30 | 2024-12-13 | Inhaler System |
| JP2025021174A Pending JP2025081422A (en) | 2019-04-30 | 2025-02-13 | Inhaler System |
Family Applications Before (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| JP2021564374A Active JP7636345B2 (en) | 2019-04-30 | 2020-04-30 | Inhaler System |
| JP2021564396A Active JP7606469B2 (en) | 2019-04-30 | 2020-04-30 | Inhaler System |
Family Applications After (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| JP2024218300A Pending JP2025060689A (en) | 2019-04-30 | 2024-12-13 | Inhaler System |
| JP2025021174A Pending JP2025081422A (en) | 2019-04-30 | 2025-02-13 | Inhaler System |
Country Status (9)
| Country | Link |
|---|---|
| US (5) | US20220203050A1 (en) |
| EP (3) | EP3797424B1 (en) |
| JP (5) | JP7636345B2 (en) |
| KR (3) | KR20220003585A (en) |
| CN (3) | CN114007673B (en) |
| AU (3) | AU2020266043A1 (en) |
| CA (3) | CA3138454A1 (en) |
| ES (1) | ES3053866T3 (en) |
| WO (3) | WO2020222147A1 (en) |
Families Citing this family (17)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP3767632B1 (en) * | 2012-06-25 | 2024-05-29 | Gecko Health Innovations, Inc. | Devices, systems, and methods for adherence monitoring and patient interaction |
| WO2021148966A1 (en) * | 2020-01-23 | 2021-07-29 | Novartis Ag | A computer-implemented system and method for outputting a prediction of an exacerbation and/or hospitalization of asthma |
| US20220233093A1 (en) * | 2021-01-22 | 2022-07-28 | AsthmaTek, Inc. | Systems and methods to provide a physician interface that enables a physician to assess asthma of a subject and provide therapeutic feedback |
| US12051492B2 (en) | 2021-01-29 | 2024-07-30 | AsthmaTek, Inc. | Systems and methods to determine a therapy regimen to treat asthma of a subject |
| GB2605170B (en) * | 2021-03-24 | 2023-09-27 | Respiratory Analytics | An inhaler monitoring device |
| GB202106254D0 (en) * | 2021-04-30 | 2021-06-16 | Teva Uk Ltd | Inhaler system |
| GB202108919D0 (en) * | 2021-06-22 | 2021-08-04 | Royal College Surgeons Ireland | Method and system to quantify and predict changes in lung function |
| CN117677417A (en) * | 2021-07-08 | 2024-03-08 | 阿斯利康(瑞典)有限公司 | Devices and systems for detection and analysis of inhaler use |
| US20250190863A1 (en) | 2022-04-12 | 2025-06-12 | Norton (Waterford) Limited | Drug delivery device with electronics |
| WO2023225407A1 (en) * | 2022-05-20 | 2023-11-23 | Muttil Pavan | Smart inhaler |
| GB2630925A (en) * | 2023-06-12 | 2024-12-18 | Pharmatics Ltd | An AI-powered detachable inhaler monitoring device and method |
| WO2025012114A1 (en) | 2023-07-07 | 2025-01-16 | Norton (Waterford) Limited | An inhalable formulation of fluticasone propionate and albuterol sulfate for the treatment of asthma |
| EP4487842A1 (en) | 2023-07-07 | 2025-01-08 | Norton (Waterford) Limited | An inhalable formulation of fluticasone propionate and albuterol sulfate for the treatment of asthma |
| AU2024294145A1 (en) | 2023-07-07 | 2025-12-04 | Norton (Waterford) Limited | An inhalable formulation of fluticasone propionate and albuterol sulfate for the treatment of asthma |
| WO2026013023A1 (en) | 2024-07-08 | 2026-01-15 | Norton (Waterford) Limited | A fixed-dose dry powder inhalation formulation of fluticasone propionate and albuterol sulfate for the treatment of asthma |
| EP4678170A1 (en) | 2024-07-08 | 2026-01-14 | Norton (Waterford) Limited | A fixed-dose dry powder inhalation formulation of fluticasone propionate and albuterol sulfate for the treatment of asthma |
| CN120771398B (en) * | 2025-09-04 | 2025-11-14 | 徐州市第一人民医院 | A monitoring method and system for inhalation therapy based on the Internet of Things |
Citations (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050172958A1 (en) * | 2003-08-20 | 2005-08-11 | The Brigham And Women's Hospital, Inc. | Inhalation device and system for the remote monitoring of drug administration |
| US20100094099A1 (en) * | 2007-02-05 | 2010-04-15 | The Brigham And Women's Hospital, Inc. | Instrumented Metered-Dose Inhaler and Methods for Predicting Disease Exacerbations |
| JP2013514822A (en) * | 2009-12-19 | 2013-05-02 | コーニンクレッカ フィリップス エレクトロニクス エヌ ヴィ | COPD exacerbation prediction system and method |
| WO2013085910A1 (en) * | 2011-12-04 | 2013-06-13 | Temple University | System and method for assessing a condition of a patient with a chronic illness |
| US20150150484A1 (en) * | 2011-08-22 | 2015-06-04 | Bioguidance Llc | Asthma monitoring device |
| US20170213145A1 (en) * | 2016-01-21 | 2017-07-27 | Verily Life Sciences Llc | Adaptive model-based system to automatically quantify fall risk |
| WO2018011113A1 (en) * | 2016-07-14 | 2018-01-18 | Koninklijke Philips N.V. | System and method for monitoring asthma symptoms |
| US20180056018A1 (en) * | 2016-08-31 | 2018-03-01 | Cephalon, Inc. | Inhalation Systems, Devices and Methods |
| WO2019030632A1 (en) * | 2017-08-11 | 2019-02-14 | Restech S.R.L. | A method for the early identification of recurrences of chronic obstructive pulmonary disease |
| JP2019506939A (en) * | 2016-01-28 | 2019-03-14 | ノバルティス アーゲー | Method, inhaler, and system for measuring flow characteristics in an inhaler |
Family Cites Families (198)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4972842A (en) | 1988-06-09 | 1990-11-27 | Vital Signals, Inc. | Method and apparatus for precision monitoring of infants on assisted ventilation |
| US4984158A (en) | 1988-10-14 | 1991-01-08 | Hillsman Dean | Metered dose inhaler biofeedback training and evaluation system |
| US5071453A (en) | 1989-09-28 | 1991-12-10 | Litton Systems, Inc. | Oxygen concentrator with pressure booster and oxygen concentration monitoring |
| US5394866A (en) | 1991-03-05 | 1995-03-07 | Aradigm Corporation | Automatic aerosol medication delivery system and methods |
| US5363842A (en) | 1991-12-20 | 1994-11-15 | Circadian, Inc. | Intelligent inhaler providing feedback to both patient and medical professional |
| US5505192A (en) | 1993-11-12 | 1996-04-09 | New-Med Corporation | Dispenser monitoring system |
| US6390088B1 (en) | 1993-12-13 | 2002-05-21 | Boehringer Ingelheim Kg | Aerosol inhaler |
| DE69424992T2 (en) | 1994-02-14 | 2000-10-26 | Aradigm Corp., Hayward | Inhalation exercise device |
| SE9400570D0 (en) | 1994-02-21 | 1994-02-21 | Astra Ab | Inhalation device, inhaler and processing unit |
| US5839429A (en) | 1994-03-25 | 1998-11-24 | Astra Aktiebolag | Method and apparatus in connection with an inhaler |
| SE9402237D0 (en) | 1994-06-23 | 1994-06-23 | Astra Ab | Measurement methods and systems |
| GB9421687D0 (en) | 1994-10-27 | 1994-12-14 | Aid Medic Ltd | Dosimetric spacer |
| US5809997A (en) | 1995-05-18 | 1998-09-22 | Medtrac Technologies, Inc. | Electronic medication chronolog device |
| AUPN332295A0 (en) | 1995-06-01 | 1995-06-29 | Butler, Donald Lewis | Personal pulmonary function analysers |
| US5957125A (en) | 1996-11-05 | 1999-09-28 | Medical Safety Products, Inc. | Apparatus for indicating proper orientation for oral and nasal inhalers |
| GB2320489A (en) | 1996-12-20 | 1998-06-24 | Norton Healthcare Ltd | Inhaler dose counter |
| SE9801122D0 (en) | 1998-03-30 | 1998-03-30 | Astra Ab | Inhalation device |
| SE9801121D0 (en) | 1998-03-30 | 1998-03-30 | Astra Ab | Electrical device |
| SE9801115D0 (en) | 1998-03-30 | 1998-03-30 | Astra Ab | Electrical device |
| US6283923B1 (en) | 1998-05-28 | 2001-09-04 | The Trustees Of Columbia University In The City Of New York | System and method for remotely monitoring asthma severity |
| JP2002517849A (en) | 1998-06-08 | 2002-06-18 | グラクソ グループ リミテッド | Disease management / education systems and methods |
| BR9911098A (en) | 1998-06-12 | 2002-01-29 | Microdose Technologies Inc | Measurement, packaging and administration of pharmaceutical drugs and medicines |
| PL349441A1 (en) | 1998-11-30 | 2002-07-29 | Novo Nordisk As | A medical system and a method of controlling the system for use by a patient for medical self treatment |
| US6990975B1 (en) | 1999-03-06 | 2006-01-31 | Smithkline Beecham Corporation | Medicament delivery system |
| GB9911388D0 (en) | 1999-05-18 | 1999-07-14 | Glaxo Group Ltd | Dispenser |
| US6466133B1 (en) | 1999-08-31 | 2002-10-15 | Airadvice, Inc. | Apparatus for allergen detection and air/asthma advice provision |
| US20030192535A1 (en) | 1999-09-24 | 2003-10-16 | Astrazeneca Ab. | Inhaler |
| EP1224601A1 (en) | 1999-10-01 | 2002-07-24 | Glaxo Group Limited | Remote patient assessment system |
| CA2399464C (en) | 2000-02-11 | 2008-10-07 | Medic-Aid Limited | Drug delivery apparatus |
| GB0003839D0 (en) | 2000-02-19 | 2000-04-05 | Glaxo Group Ltd | Housing for an inhaler |
| GB0004456D0 (en) | 2000-02-26 | 2000-04-19 | Glaxo Group Ltd | Medicament dispenser |
| WO2002005879A1 (en) | 2000-07-15 | 2002-01-24 | Glaxo Group Limited | Medicament dispenser |
| GB0021024D0 (en) | 2000-08-29 | 2000-10-11 | Glaxo Group Ltd | Inhalation device |
| GB0025749D0 (en) | 2000-10-20 | 2000-12-06 | Glaxo Group Ltd | Inhaler |
| GB0026646D0 (en) | 2000-10-31 | 2000-12-13 | Glaxo Group Ltd | Medicament dispenser |
| GB0108213D0 (en) | 2001-04-02 | 2001-05-23 | Glaxo Group Ltd | Medicament dispenser |
| GB0108208D0 (en) | 2001-04-02 | 2001-05-23 | Glaxo Group Ltd | Medicament dispenser |
| GB0108228D0 (en) | 2001-04-02 | 2001-05-23 | Glaxo Group Ltd | Medicament dispenser |
| US20080177154A1 (en) | 2001-08-13 | 2008-07-24 | Novo Nordisk A/S | Portable Device and Method Of Communicating Medical Data Information |
| GB0127989D0 (en) | 2001-11-22 | 2002-01-16 | Glaxo Group Ltd | Medicament dispensing system |
| GB0217199D0 (en) | 2002-07-25 | 2002-09-04 | Glaxo Group Ltd | Medicament dispenser |
| WO2003063754A1 (en) | 2002-01-30 | 2003-08-07 | Glaxo Group Limited | Compliance aid |
| GB0209531D0 (en) | 2002-04-26 | 2002-06-05 | Glaxo Group Ltd | Medicament dispenser |
| US7233228B2 (en) | 2002-04-29 | 2007-06-19 | Glaxo Group Limited | Alerting system |
| GB0209782D0 (en) | 2002-04-29 | 2002-06-05 | Glaxo Group Ltd | Medicament dispenser |
| GB0216831D0 (en) | 2002-07-19 | 2002-08-28 | Glaxo Group Ltd | Medicament dispenser |
| WO2004011068A1 (en) | 2002-07-25 | 2004-02-05 | Glaxo Group Limited | Medicament dispenser |
| GB2397527A (en) * | 2003-01-23 | 2004-07-28 | David Wald | Angina medication dose dispenser with log and analysis means for the diagnosis of risk of myocardial infartion |
| GB0311461D0 (en) | 2003-05-19 | 2003-06-25 | Glaxo Group Ltd | Display system |
| GB2406283B (en) | 2003-09-24 | 2006-04-05 | Altana Pharma Ag | Compliance monitor and method |
| GB2398065A (en) | 2003-10-16 | 2004-08-11 | Bespak Plc | Dispensing apparatus |
| US20050108046A1 (en) | 2003-11-18 | 2005-05-19 | Boehringer Ingelheim Pharmaceuticals, Inc. | Clinical management system and methods |
| GB0328859D0 (en) | 2003-12-12 | 2004-01-14 | Clinical Designs Ltd | Dispenser and counter |
| US8403865B2 (en) | 2004-02-05 | 2013-03-26 | Earlysense Ltd. | Prediction and monitoring of clinical episodes |
| US9131891B2 (en) | 2005-11-01 | 2015-09-15 | Earlysense Ltd. | Monitoring a condition of a subject |
| DE102004009435A1 (en) | 2004-02-24 | 2005-12-08 | Boehringer Ingelheim International Gmbh | atomizer |
| WO2006031712A2 (en) | 2004-09-13 | 2006-03-23 | Oriel Therapeutics, Inc. | Tubular dry powder drug containment systems, associated inhalers and methods |
| US8231573B2 (en) | 2005-02-01 | 2012-07-31 | Intelliject, Inc. | Medicament delivery device having an electronic circuit system |
| US8740789B2 (en) * | 2005-03-03 | 2014-06-03 | Cardiac Pacemakers, Inc. | Automatic etiology sequencing system and method |
| TWI442951B (en) | 2005-04-14 | 2014-07-01 | Astrazeneca Ab | Inhaler meter |
| KR20080030563A (en) | 2005-05-12 | 2008-04-04 | 코스 라이프 싸이언시즈, 인크. | Dose counter for metered dose inhalers |
| NZ540250A (en) | 2005-05-20 | 2008-04-30 | Nexus6 Ltd | Reminder alarm for inhaler with variable and selectable ring tone alarms |
| US8795170B2 (en) | 2005-11-29 | 2014-08-05 | Venture Gain LLC | Residual based monitoring of human health |
| US9242056B2 (en) | 2006-03-07 | 2016-01-26 | Bang & Olufsen Medicom A/S | Acoustic inhaler flow measurement |
| GB0610775D0 (en) | 2006-05-31 | 2006-07-12 | Glaxo Group Ltd | Dispensing device |
| US20070295329A1 (en) | 2006-06-13 | 2007-12-27 | Lieberman Eric A | Dose indicator |
| WO2008070516A2 (en) | 2006-12-01 | 2008-06-12 | Abbott Laboratories | Dose selective breath actuated inhaler |
| GB0625303D0 (en) | 2006-12-19 | 2007-01-24 | Jagotec Ag | Improvements in and relating to metered dose inhalers |
| JP4909156B2 (en) * | 2007-03-30 | 2012-04-04 | 富士フイルム株式会社 | Image presenting apparatus, image presenting method, and program |
| EP1992381A1 (en) | 2007-05-16 | 2008-11-19 | Boehringer Ingelheim Pharma GmbH & Co. KG | Dispensing device |
| JP2008301847A (en) | 2007-06-05 | 2008-12-18 | Canon Inc | Inhalation device and driving method thereof |
| GB0712803D0 (en) | 2007-07-02 | 2007-08-08 | Glaxo Group Ltd | Medicament dispenser |
| US20090151718A1 (en) | 2007-12-13 | 2009-06-18 | Next Safety, Inc. | Apparatuses and Methods for Diagnosing and Treating Respiratory Conditions |
| WO2009093969A1 (en) | 2008-01-23 | 2009-07-30 | Astrazeneca Ab | A medicament-containing dispenser provided with a display for presenting indicia to a user |
| US9550031B2 (en) | 2008-02-01 | 2017-01-24 | Reciprocal Labs Corporation | Device and method to monitor, track, map, and analyze usage of metered-dose inhalers in real-time |
| US20090221308A1 (en) | 2008-03-03 | 2009-09-03 | Novartis Ag | System and Method for Enhancing Drug-Taking Compliance |
| EP2106806A1 (en) | 2008-03-31 | 2009-10-07 | Fraunhofer-Gesellschaft zur Förderung der Angewandten Forschung e.V. | Nanoparticles for targeted delivery of active agents to the lung |
| JP5479465B2 (en) | 2008-06-20 | 2014-04-23 | マンカインド コーポレイション | Interactive device and method for profiling inhalation efforts in real time |
| US8844525B2 (en) * | 2008-07-25 | 2014-09-30 | Resmed Limited | Method and apparatus for detecting and treating heart failure |
| GB2462304B (en) | 2008-07-31 | 2010-12-01 | Laerdal Medical As | Device and method for detecting heart beats in a patient using the airway pressure |
| AU2009286377A1 (en) | 2008-08-25 | 2010-03-04 | Koninklijke Philips Electronics N.V. | Respiratory drug delivery apparatus which provides audio instructions |
| WO2010037058A2 (en) | 2008-09-26 | 2010-04-01 | Incube Labs, Llc | Controlled inhaler for distributing inhalant according to inhalation velocity |
| US8231541B2 (en) | 2008-10-22 | 2012-07-31 | Sharp Laboratories Of America, Inc. | Asthma status scoring method and system with confidence ratings |
| US8960189B2 (en) | 2008-12-11 | 2015-02-24 | Koninklijke Philips N.V. | System and method for monitoring a metered dose inhaler |
| NZ574666A (en) | 2009-02-05 | 2009-04-30 | Nexus6 Ltd | A medicament inhaler holder that uses optical means to count and display the number of doses used |
| US9526429B2 (en) * | 2009-02-06 | 2016-12-27 | Resmed Sensor Technologies Limited | Apparatus, system and method for chronic disease monitoring |
| WO2010103435A1 (en) | 2009-03-10 | 2010-09-16 | Koninklijke Philips Electronics N.V. | Diagnosis of asthma |
| NZ575836A (en) | 2009-03-27 | 2009-08-28 | Nexus6 Ltd | Improvements in or Relating to Medicament Delivery Systems |
| NZ575943A (en) | 2009-04-01 | 2009-07-31 | Nexus6 Ltd | Improvements in or Relating to Medicament Delivery Devices |
| US9060715B2 (en) | 2009-07-22 | 2015-06-23 | Koninklijke Philips N.V. | Nebulizer |
| US8547239B2 (en) | 2009-08-18 | 2013-10-01 | Cequr Sa | Methods for detecting failure states in a medicine delivery device |
| US8539945B2 (en) | 2009-08-18 | 2013-09-24 | Teva Pharmaceutical Industries Ltd. | Dose counter and recording method |
| US8758262B2 (en) | 2009-11-25 | 2014-06-24 | University Of Rochester | Respiratory disease monitoring system |
| WO2011083377A1 (en) | 2010-01-07 | 2011-07-14 | Koninklijke Philips Electronics N.V. | Respiratory drug delivery apparatus including a feedback and compliance device |
| US8620591B2 (en) | 2010-01-14 | 2013-12-31 | Venture Gain LLC | Multivariate residual-based health index for human health monitoring |
| JP5961116B2 (en) * | 2010-03-08 | 2016-08-02 | コーニンクレッカ フィリップス エヌ ヴェKoninklijke Philips N.V. | System and method for obtaining an objective measure of dyspnea |
| GB201006901D0 (en) | 2010-04-26 | 2010-06-09 | Sagentia Ltd | Device for monitoring status and use of an inhalation or nasal drug delivery device |
| PL2987522T3 (en) | 2010-05-18 | 2019-07-31 | Ivax Pharmaceuticals Ireland | DOSE COUNTERS FOR INHALERS |
| EP3108966B1 (en) | 2010-06-18 | 2019-10-09 | Boehringer Ingelheim International GmbH | Inhaler |
| WO2012123919A2 (en) | 2011-03-16 | 2012-09-20 | Koninklijke Philips Electronics N.V. | System and method of remotely monitoring and/or managing the treatment of a plurality of subjects with aerosolized medicament |
| US20140213925A1 (en) | 2011-09-20 | 2014-07-31 | Isonea Limited | Systems, methods and kits for measuring respiratory rate and dynamically predicting respiratory episodes |
| NZ595367A (en) | 2011-09-23 | 2012-02-24 | Nexus6 Ltd | A dose counting mechanism adapted to enclose a medicament delivery device |
| EP2788059A2 (en) | 2011-12-05 | 2014-10-15 | CHIESI FARMACEUTICI S.p.A. | Method and system for electronic mdi model |
| PT2797652T (en) | 2011-12-27 | 2019-02-19 | Vectura Gmbh | Inhalation device with feedback system |
| CN104023633B (en) | 2011-12-30 | 2017-05-24 | 皇家飞利浦有限公司 | Airway Impedance Measurement Integrated with Respiratory Treatment Devices |
| RU2480153C1 (en) * | 2012-02-10 | 2013-04-27 | Государственное Бюджетное Образовательное Учреждение Дополнительного Профессионального Образования "Иркутская Государственная Медицинская Академия Последипломного Образования" | Method of predicting course of moderate to severe chronic obstructive lung disease |
| WO2013138384A2 (en) | 2012-03-12 | 2013-09-19 | Uptoke Llc | Electronic vaporizing device and methods for use |
| ES2629479T3 (en) | 2012-03-15 | 2017-08-10 | Relevo Limited | Actuator device for inhalers |
| EP2858560B1 (en) | 2012-06-08 | 2021-03-17 | Koninklijke Philips N.V. | Method and system for monitoring the lung function of a patient |
| US11529072B2 (en) * | 2012-06-18 | 2022-12-20 | AireHealth Inc. | Method and apparatus for performing dynamic respiratory classification and tracking of wheeze and crackle |
| US9427534B2 (en) | 2012-07-05 | 2016-08-30 | Clement Clarke International Ltd. | Drug delivery inhaler devices |
| AU2013200972A1 (en) | 2012-07-27 | 2014-02-13 | Resmed Limited | System and Method for Tracking Medical Device Usage |
| US10258753B2 (en) | 2012-10-04 | 2019-04-16 | Boehringer Ingelheim International Gmbh | System, method, use and information storage medium for practicing of an inhalation process |
| US9179260B2 (en) | 2012-12-03 | 2015-11-03 | Mylan Inc. | Medicament information system and method |
| US9911308B2 (en) | 2012-12-27 | 2018-03-06 | Kaleo, Inc. | Devices, systems and methods for locating and interacting with medicament delivery systems |
| WO2014164897A2 (en) | 2013-03-11 | 2014-10-09 | Collins John R | Inhalator device and method |
| US9469527B2 (en) | 2013-03-14 | 2016-10-18 | Taiwan Semiconductor Manufacturing Company, Ltd. | MEMS pressure sensor and microphone devices having through-vias and methods of forming same |
| WO2015178907A1 (en) | 2013-05-21 | 2015-11-26 | Reciprocal Labs Corporation | Usage monitoring attachment for medicament dispenser |
| US8807131B1 (en) | 2013-06-18 | 2014-08-19 | Isonea Limited | Compliance monitoring for asthma inhalers |
| AU2014287059A1 (en) | 2013-07-12 | 2016-02-04 | Oscillari Llc | Acoustic based drug delivery monitor |
| WO2016049066A1 (en) | 2014-09-23 | 2016-03-31 | Oscillari Llc | Vibration sensor based drug delivery monitor |
| US10828434B2 (en) | 2013-08-30 | 2020-11-10 | Adherium (Nz) Limited | Compliance monitor for a medicament inhaler |
| US11424017B2 (en) * | 2013-10-19 | 2022-08-23 | Aptargroup, Inc. | Respiratory system and method that monitors medication flow |
| US10019555B2 (en) | 2013-10-19 | 2018-07-10 | Cohero Health, Inc. | Interactive respiratory device usage tracking system |
| WO2015066562A2 (en) | 2013-10-31 | 2015-05-07 | Knox Medical Diagnostics | Systems and methods for monitoring respiratory function |
| GB2519964A (en) * | 2013-11-01 | 2015-05-13 | Linde Aktiengesellshcaft | Apparatus and method for detecting health deterioration |
| US9188579B2 (en) | 2013-11-21 | 2015-11-17 | Qualcomm Incorporated | Sniffing smartphone |
| JP6097677B2 (en) | 2013-12-05 | 2017-03-15 | 日本光電工業株式会社 | Display device and display method |
| ES2934847T3 (en) | 2014-03-03 | 2023-02-27 | Adherium Nz Ltd | Compliance Monitor for Dry Powder Drug Delivery Device |
| US10743793B2 (en) | 2014-03-10 | 2020-08-18 | Respimetrix Gmbh | Systems and methods for delivering an agent to a user's lungs and for simultaneously monitoring lung health |
| PL3129087T3 (en) | 2014-04-07 | 2020-09-21 | Boehringer Ingelheim International Gmbh | Method, electronic device, inhalation training system for practicing and/or controlling an inhalation process of a patient |
| EP3142735A4 (en) | 2014-05-16 | 2018-01-24 | Adherium (NZ) Limited | Devices and methods for identification of medicament delivery devices |
| EP4487893A3 (en) | 2014-05-27 | 2025-03-26 | ResMed, Inc. | Remote data management for medical devices |
| US9679113B2 (en) | 2014-06-11 | 2017-06-13 | Aic Innovations Group, Inc. | Medication adherence monitoring system and method |
| EP3160343B1 (en) | 2014-06-27 | 2018-03-14 | Koninklijke Philips N.V. | Apparatus, system, method and computer program for assessing the risk of an exacerbation and/or hospitalization |
| AR102055A1 (en) | 2014-08-28 | 2017-02-01 | Norton (Waterford) Ltd | ASSISTANCE MODULE FOR THE CORRECT USE OF AN INHALER |
| EP3193990A1 (en) | 2014-09-15 | 2017-07-26 | Adherium (NZ) Ltd. | Adherence monitor for a dry powder medicament delivery device |
| US11497865B2 (en) | 2014-09-16 | 2022-11-15 | Medituner Ab | Computer controlled dosage system |
| CA2998709A1 (en) | 2014-09-17 | 2016-03-24 | Canary Medical Inc. | Devices, systems and methods for using and monitoring medical devices |
| US11033694B2 (en) | 2014-09-22 | 2021-06-15 | Koninklijke Philips N.V. | Inhaler with orientation sensor |
| US20160089089A1 (en) | 2014-09-25 | 2016-03-31 | Aedio, Inc. | Systems and methods for digital predictive disease exacerbation and pre-emptive treatment |
| US20160106935A1 (en) | 2014-10-17 | 2016-04-21 | Qualcomm Incorporated | Breathprint sensor systems, smart inhalers and methods for personal identification |
| US11051554B2 (en) | 2014-11-12 | 2021-07-06 | Rai Strategic Holdings, Inc. | MEMS-based sensor for an aerosol delivery device |
| CN107106794A (en) | 2014-11-20 | 2017-08-29 | 寇格尼塔有限责任公司 | Measurement, auxiliary and bearing calibration and device that inhalator is used |
| US10058661B2 (en) * | 2014-12-04 | 2018-08-28 | Norton (Waterford) Limited | Inhalation monitoring system and method |
| US11596738B2 (en) | 2014-12-04 | 2023-03-07 | Becton, Dickinson And Company | Force sensing resistor for liquid low-volume detection and occlusion sensing and methods and apparatuses for flow sensing along fluid path in fluid delivery device |
| CN107106796B (en) | 2015-01-09 | 2021-02-09 | 安瑞智能(新西兰)有限公司 | Monitor for a medicament inhaler |
| EP3248123A1 (en) | 2015-01-20 | 2017-11-29 | Novartis AG | Application unlock using a connected physical device and transfer of data therebetween |
| US20160283686A1 (en) | 2015-03-23 | 2016-09-29 | International Business Machines Corporation | Identifying And Ranking Individual-Level Risk Factors Using Personalized Predictive Models |
| US10726954B2 (en) * | 2015-04-22 | 2020-07-28 | Reciprocal Labs Corporation | Predictive modeling of respiratory disease risk and events |
| PL3111978T3 (en) | 2015-07-03 | 2022-01-24 | Novartis Ag | Inhaler adapted to read information stored in a data storage means of a container |
| US10664572B2 (en) | 2015-08-06 | 2020-05-26 | Microsoft Technology Licensing, Llc | Recommendations for health benefit resources |
| US11980484B2 (en) * | 2015-08-26 | 2024-05-14 | Resmed Sensor Technologies Limited | Systems and methods for monitoring and management of chronic disease |
| US20180221600A1 (en) | 2015-09-04 | 2018-08-09 | Presspart Gmbh & Co. Kg | Metered-Dose Inhaler Counter (MDI) with Lateral Switches and Metered-Does Inhaler Including such a Counter |
| US20190105450A1 (en) | 2015-09-25 | 2019-04-11 | Adherium (Nz) Limited | Adherence monitor for a medicament inhaler |
| US10957447B2 (en) | 2015-10-15 | 2021-03-23 | Reciprocal Labs Corporation | Pre-emptive chronic obstructive pulmonary disease risk notifications based on medicament device monitoring |
| US10255412B2 (en) | 2015-11-13 | 2019-04-09 | Reciprocal Labs Corporation | Real time adaptive controller medication dosing |
| US20170182267A1 (en) * | 2015-12-28 | 2017-06-29 | Lunatech, Llc | Electronic Vapor Device Spirometer |
| EP3416711B1 (en) | 2016-02-17 | 2022-04-06 | Adherium (NZ) Limited | Adherence monitor for a medicament inhaler with tethered cap |
| MA44627A (en) | 2016-04-04 | 2019-02-13 | Nexvap Sa | MOBILE INHALATOR AND CONTAINER USED AT THE SAME TIME |
| EP3228345A1 (en) | 2016-04-04 | 2017-10-11 | Nexvap SA | Inhaler and liquid composition |
| US11344684B2 (en) | 2016-04-05 | 2022-05-31 | Kindeva Drug Delivery L.P. | Medicinal inhaler refill assemblies comprising a lockout override mechanism |
| WO2017176704A1 (en) | 2016-04-05 | 2017-10-12 | 3M Innovative Properties Company | Medicinal inhaler refill assemblies comprising a lockout mechanism |
| US11244748B2 (en) | 2016-04-14 | 2022-02-08 | Mylan Inc. | Systems, devices and methods for assessing inhalation therapy |
| EP3448457B1 (en) | 2016-04-28 | 2024-01-17 | Embecta Corp. | Smart medication delivery devices for providing users with delivery infomatics and methods of using same |
| KR102295739B1 (en) | 2016-05-03 | 2021-08-30 | 뉴마 레스퍼러토리 인코포레이티드 | Droplet delivery device for delivery of fluids to the pulmonary system and methods of use |
| AU2017259982B2 (en) * | 2016-05-03 | 2021-04-01 | Pneuma Respiratory, Inc. | Systems and methods for pulmonary health management |
| EP3452152B1 (en) | 2016-05-03 | 2025-07-02 | Pneuma Respiratory, Inc. | A droplet delivery device for generating and delivering droplets to the pulmonary system |
| US10371737B2 (en) | 2016-06-17 | 2019-08-06 | Thin Film Electronics Asa | Wireless mechanism for detecting an open or closed container, and methods of making and using the same |
| FR3055052B1 (en) * | 2016-08-10 | 2020-02-21 | L'air Liquide, Societe Anonyme Pour L'etude Et L'exploitation Des Procedes Georges Claude | DATA PROCESSING SYSTEM FOR PREDICTING EXACERBATION CRISIS OF A PATIENT WITH CHRONIC RESPIRATORY DISEASE |
| EP3500227A4 (en) | 2016-08-16 | 2020-04-08 | Resolve Digital Health Inc. | Digital health ecosystem |
| US20180085540A1 (en) | 2016-09-28 | 2018-03-29 | Qualcomm Incorporated | Inhaler with one or more visual sensors |
| ES2871787T3 (en) | 2016-10-07 | 2021-11-02 | Boehringer Ingelheim Int | Medication compliance control system |
| DK3541288T3 (en) | 2016-11-15 | 2023-09-11 | Boehringer Ingelheim Vetmedica Gmbh | METHOD FOR PREDICTING A SPECIFIC RESPIRATORY PATHOGEN |
| US20180161530A1 (en) | 2016-12-14 | 2018-06-14 | Qualcomm Incorporated | Flow sensing medicine delivery device |
| US20190328278A1 (en) | 2017-01-03 | 2019-10-31 | 3M Innovative Properties Company | System and method for monitoring respiration |
| GB2558895B (en) | 2017-01-17 | 2019-10-09 | Cambridge Entpr Ltd | A thermal fluid flow sensor |
| GB2558896B (en) | 2017-01-17 | 2019-10-09 | Cambridge Entpr Ltd | A single membane flow-pressure sensing device |
| KR101846951B1 (en) * | 2017-02-22 | 2018-04-09 | 주식회사 씨씨앤아이리서치 | An application for predicting an acute exacerbation of chronic obstructive pulmonary disease |
| WO2018160073A1 (en) | 2017-03-01 | 2018-09-07 | Adherium (Nz) Limited | Adherence monitor for a medicament inhaler |
| EP3370175A1 (en) * | 2017-03-03 | 2018-09-05 | Linde Aktiengesellschaft | Method for providing a wearable device, method for predicting an acute exacerbation and system for predicting an acute exacerbation |
| EP3375473A1 (en) | 2017-03-17 | 2018-09-19 | PARI Pharma GmbH | Control device for aerosol nebulizer system |
| GB2563205A (en) * | 2017-06-01 | 2018-12-12 | Linde Ag | System and method for predicting an acute exacerbation of a patient's health condition |
| US20190014824A1 (en) | 2017-07-17 | 2019-01-17 | Torque Research and Development, Inc. | Portable device and method for vaporizing materials |
| ES2932836T3 (en) | 2017-07-25 | 2023-01-26 | Adherium Nz Ltd | Adhesion control method and device |
| US11195622B2 (en) * | 2017-10-04 | 2021-12-07 | Reciprocal Labs Corporation | Pre-emptive asthma risk notifications based on medicament device monitoring |
| US20190108912A1 (en) | 2017-10-05 | 2019-04-11 | Iquity, Inc. | Methods for predicting or detecting disease |
| TWI655411B (en) | 2017-10-17 | 2019-04-01 | 香港商維吉朗科技有限公司 | Roller counter spirometer |
| US11925485B2 (en) * | 2017-12-06 | 2024-03-12 | Cardiac Pacemakers, Inc. | Non-invasive system for monitoring and treating respiratory distress |
| WO2019115779A1 (en) * | 2017-12-14 | 2019-06-20 | Fluidda Respi Nv | Screening tool for patients pulmonary conditions |
| US11342057B2 (en) | 2017-12-19 | 2022-05-24 | Reciprocal Labs Corporation | Dynamic graphical user interface for interaction with patient respiratory disease data |
| US10890343B2 (en) | 2018-02-07 | 2021-01-12 | Government Of The United States As Represented By The Administrator Of The U.S. Environmental Protection Agency | System and method for assessment and management of air pollution exposures using personal devices |
| US11804303B2 (en) | 2018-03-01 | 2023-10-31 | Reciprocal Labs Corporation | Evaluation of respiratory disease risk in a geographic region based on medicament device monitoring |
| US20190290127A1 (en) | 2018-03-20 | 2019-09-26 | Aic Innovations Group, Inc. | Apparatus and method for user evaluation |
| US11769598B2 (en) | 2018-05-21 | 2023-09-26 | Reciprocal Labs Corporation | Pre-emptive asthma risk notifications based on medicament device monitoring |
| US11456079B2 (en) | 2018-08-16 | 2022-09-27 | Reciprocal Labs Corporation | Identification of asthma triggering conditions based on medicament device monitoring for a patient |
| WO2020087014A1 (en) | 2018-10-26 | 2020-04-30 | AIRx Health, Inc. | Devices and methods for remotely managing chronic medical conditions |
| CN110021397A (en) | 2019-02-01 | 2019-07-16 | 捷普科技(上海)有限公司 | Method and storage medium based on human body physiological parameter prediction dosage |
-
2020
- 2020-04-30 KR KR1020217038827A patent/KR20220003585A/en active Pending
- 2020-04-30 WO PCT/IB2020/054057 patent/WO2020222147A1/en not_active Ceased
- 2020-04-30 KR KR1020217038823A patent/KR20220003584A/en active Pending
- 2020-04-30 CN CN202080032344.4A patent/CN114007673B/en active Active
- 2020-04-30 AU AU2020266043A patent/AU2020266043A1/en not_active Abandoned
- 2020-04-30 WO PCT/IB2020/054056 patent/WO2020222146A1/en not_active Ceased
- 2020-04-30 CN CN202080032408.0A patent/CN114008721A/en active Pending
- 2020-04-30 EP EP20724568.9A patent/EP3797424B1/en active Active
- 2020-04-30 EP EP20724570.5A patent/EP3796962A1/en not_active Withdrawn
- 2020-04-30 WO PCT/IB2020/054059 patent/WO2020222148A1/en not_active Ceased
- 2020-04-30 CA CA3138454A patent/CA3138454A1/en active Pending
- 2020-04-30 CA CA3138446A patent/CA3138446A1/en active Pending
- 2020-04-30 AU AU2020265813A patent/AU2020265813A1/en not_active Abandoned
- 2020-04-30 CN CN202080032345.9A patent/CN114008720A/en active Pending
- 2020-04-30 KR KR1020217038816A patent/KR20220003583A/en active Pending
- 2020-04-30 JP JP2021564374A patent/JP7636345B2/en active Active
- 2020-04-30 AU AU2020264799A patent/AU2020264799A1/en not_active Abandoned
- 2020-04-30 EP EP20724938.4A patent/EP3797425B1/en active Active
- 2020-04-30 ES ES20724938T patent/ES3053866T3/en active Active
- 2020-04-30 JP JP2021564396A patent/JP7606469B2/en active Active
- 2020-04-30 JP JP2021564397A patent/JP7664181B2/en active Active
- 2020-04-30 US US17/607,442 patent/US20220203050A1/en active Pending
- 2020-04-30 CA CA3138456A patent/CA3138456A1/en active Pending
- 2020-12-22 US US17/131,154 patent/US12138387B2/en active Active
-
2022
- 2022-07-14 US US17/864,582 patent/US12036359B2/en active Active
-
2024
- 2024-06-24 US US18/751,627 patent/US20240342404A1/en active Pending
- 2024-06-25 US US18/753,326 patent/US20240342405A1/en active Pending
- 2024-12-13 JP JP2024218300A patent/JP2025060689A/en active Pending
-
2025
- 2025-02-13 JP JP2025021174A patent/JP2025081422A/en active Pending
Patent Citations (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050172958A1 (en) * | 2003-08-20 | 2005-08-11 | The Brigham And Women's Hospital, Inc. | Inhalation device and system for the remote monitoring of drug administration |
| US20100094099A1 (en) * | 2007-02-05 | 2010-04-15 | The Brigham And Women's Hospital, Inc. | Instrumented Metered-Dose Inhaler and Methods for Predicting Disease Exacerbations |
| JP2013514822A (en) * | 2009-12-19 | 2013-05-02 | コーニンクレッカ フィリップス エレクトロニクス エヌ ヴィ | COPD exacerbation prediction system and method |
| US20150150484A1 (en) * | 2011-08-22 | 2015-06-04 | Bioguidance Llc | Asthma monitoring device |
| WO2013085910A1 (en) * | 2011-12-04 | 2013-06-13 | Temple University | System and method for assessing a condition of a patient with a chronic illness |
| US20170213145A1 (en) * | 2016-01-21 | 2017-07-27 | Verily Life Sciences Llc | Adaptive model-based system to automatically quantify fall risk |
| JP2019506939A (en) * | 2016-01-28 | 2019-03-14 | ノバルティス アーゲー | Method, inhaler, and system for measuring flow characteristics in an inhaler |
| WO2018011113A1 (en) * | 2016-07-14 | 2018-01-18 | Koninklijke Philips N.V. | System and method for monitoring asthma symptoms |
| US20180056018A1 (en) * | 2016-08-31 | 2018-03-01 | Cephalon, Inc. | Inhalation Systems, Devices and Methods |
| WO2019030632A1 (en) * | 2017-08-11 | 2019-02-14 | Restech S.R.L. | A method for the early identification of recurrences of chronic obstructive pulmonary disease |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP7606469B2 (en) | Inhaler System | |
| US11419995B2 (en) | Inhaler system | |
| CN115942966A (en) | inhaler system | |
| KR20220119649A (en) | inhaler system | |
| US20240225479A1 (en) | Inhaler system |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| A521 | Request for written amendment filed |
Free format text: JAPANESE INTERMEDIATE CODE: A523 Effective date: 20220105 |
|
| A621 | Written request for application examination |
Free format text: JAPANESE INTERMEDIATE CODE: A621 Effective date: 20230418 |
|
| A977 | Report on retrieval |
Free format text: JAPANESE INTERMEDIATE CODE: A971007 Effective date: 20240131 |
|
| A131 | Notification of reasons for refusal |
Free format text: JAPANESE INTERMEDIATE CODE: A131 Effective date: 20240228 |
|
| A601 | Written request for extension of time |
Free format text: JAPANESE INTERMEDIATE CODE: A601 Effective date: 20240528 |
|
| A601 | Written request for extension of time |
Free format text: JAPANESE INTERMEDIATE CODE: A601 Effective date: 20240726 |
|
| A521 | Request for written amendment filed |
Free format text: JAPANESE INTERMEDIATE CODE: A523 Effective date: 20240805 |
|
| A131 | Notification of reasons for refusal |
Free format text: JAPANESE INTERMEDIATE CODE: A131 Effective date: 20241023 |
|
| A521 | Request for written amendment filed |
Free format text: JAPANESE INTERMEDIATE CODE: A523 Effective date: 20250117 |
|
| TRDD | Decision of grant or rejection written | ||
| A01 | Written decision to grant a patent or to grant a registration (utility model) |
Free format text: JAPANESE INTERMEDIATE CODE: A01 Effective date: 20250312 |
|
| A61 | First payment of annual fees (during grant procedure) |
Free format text: JAPANESE INTERMEDIATE CODE: A61 Effective date: 20250407 |
|
| R150 | Certificate of patent or registration of utility model |
Ref document number: 7664181 Country of ref document: JP Free format text: JAPANESE INTERMEDIATE CODE: R150 |