zyxwv
zyxwv
zyxwvuts
zyxw
Scandinavian Journal of Psychology, 1991, 32, 193-207
Parental grief following the death of an infanta follow-up over one year
ATLE DYREGROV and STIG BERGE MATTHIESEN
zyxwvu
zyxwvuts
zyxwvutsrqp
Department of Pediatrics, University of Bergen, Norway
Dyregrov, A. Br Matthiesen, S. B. (1991). Parental grief following the death of an infanta follow-up over one year. Scandinavian Journal of Psychology, 32, 193-207.
The course of parental bereavement during the first year following an infant’s death was
investigated. Also, the differences in mothers’ and fathers’ reactions, the differences according to the mothers’ occupational role, and the similarities in couples’ reactions were studied.
From a total sample of 59 families, 13 families answered their questionnaires at all three
time points ( I , 6 and 13 months), 22 families responded at two time points, and 37 families
responded at some point following the loss. Measures relating to anxiety, depression, bodily
discomfort, general well being and impact of event were used at the three time points. The
results showed that grief, as measured by the different inventories, decreased over time. The
decrease was most evident from 6 to 13 months, and most prominent in women. A
considerable number of the parents were still actively dealing with the loss all through the
first year of bereavement. In most couples the mother reported most distress. Mothers were
significantly more depressed than fathers at all time points, and mothers also had significantly higher anxiety and lower general health at 1 and 13 months, and intrusive scores of
1 and 6 months. Women at home evidenced more grief at all three time points than women
employed outside the home. A high or low score in one spouse was more strongly correlated
with a similar score in the other at I and 13 months, than at 6 months. The implications for
counselling of parents, with special emphasis on the employment situation of the mother, is
emphasized.
Key words: Infant loss, bereaved parents, grief reactions
Atle Dyregrov. Center for Crish Psychology, Fabrikkgaten 5, 5037 Solheimsvik, Norway
Many studies indicate a decline in grief over time following the loss of an infant child
(DeFrain & Ernst, 1978; Clarke & Williams, 1979; Lowman, 1979; Price et at., 1985).
However, the time proposed for satisfactory adjustment vanes considerably. The grief
reactions of the majority of parents continued throughout the first year of bereavement
(Jensen & Zahourek, 1972; DeFrain & Emst, 1978; Forrest, Standish & Baum, 1982; Price
et al., 1985; Videka-Sherman & Lieberman, 1985), and there are indications of long-term
consequences (several years) of child bereavement with little diminishing of grief over time
(Jurk et ul., 1981; Laurell-Borulf, 1982; Miles, 1985; Rando, 1983; Lehman et ul., 1987).
However, others (Lowman,1979; Cooper, 1980) have found that the majority of parents had
returned to normal function after 6 months.
Clinical reports and retrospective studies focusing on the father’s grief find it to be less
intense and shorter than the mother’s following the death of a infant (e.g. Benfield et ul., 1978;
Helmrath & Steinitz, 1978; Peppers & Knapp, 1980; Wilson el uf., 1982; LaRoche et ul., 1984;
Videka-Sherman & Lieberman, 1985; Dyregrov & Matthiesen. 19870). It has been reported
that the majority of men were shown to have recovered within 6 months of the loss (Forrest
et al., 1982; CornweU et al., 1977). Systematic measurements of grief reactions have shown that
fathers report less grief than mothers (Dyregrov & Matthiesen, 1987~;Kennel et uf., 1970).
There is mounting evidence suggesting that working women in general fare better
emotionally than housewifes (Haw, 1982; Kessler & McRae, 1982; Verbrugge, 1983). Women
�194
zyxwvu
zyxwvut
zyxw
zyxw
zyx
zyxwvut
A. Dyregrov and S. B. Matthiesen
%and J Psycho1 32 (1991)
in the housewife role have been found to have lower self-esteem than their employed
counterparts (Birnbaum, 1975), and they are significantly more depressed than wifes employed outside the home. Employed wives do not significantly differ in level of depression
from comparable men (Gore & Mangione, 1983). Following infant loss, it is known that
many men become increasingly involved outside the home (Mandell ef al., 1980). Men are
said to find the structured activity of their work helpful. It is not known how work outside
the home affects women’s grief reactions. In this report this question will be addressed.
Mothers who report strong (or mild) reactions tend to have partners who report strong (or
mild) reactions (Benfield et al., 1978; Dyregrov & Matthiesen, 1987~).No prospective study
has been conducted to see whether this changes during the course of bereavement.
The inconsistent findings in the various reports can be due to problems in measurement
and method. The vast majority of studies have been retrospective, and systematic measures
to rate various components of grief have seldomly been applied. In this article we will assess
grief reactions prospectively over the first year of bereavement. We will apply 5 different
psychological inventories to ensure a measurement of various components of grief, and both
mens’ and womens’ grief reactions will be measured.
The following issues are addressed:
1. Is there a gradual decline in grief reactions, as measured during the first year of
bereavement?
2. To what extent do mothers’ and fathers’ grief reactions differ during the first year of
bereavement?
3. Do mothers’ reactions differ according to their occupational role?
4. Do the two members of a couple react in a similar or different way?
METHOD
Subjects
Fifty nine families who lost a child during the first year of life received questionnaires. One family
consisted of a mother only. This constituted all families (with the exception of 9 families mentioned
below) who suffered the IOU of their child at the Neonatal Intensive Care Unit at the Department of
Pediatrics, Haukeland Hospital, Bergen within a 24 year period, and all Sudden Infant Death (SIDS)
families that were in contact with the Department of Pediatrics in the same time period. Nine families
were excluded because of practical, clinical or ethical reasons: foreigners (2). twin birth with the death
of one or both twins (2) extremely adverse psychosocial family situation (4). address unknown (1).
In 13 of the 50 families who received the questionnaires both parents answered their questionnaire on
all 3 occasions ( I , 6 & 13 months) after the loss of their child. Some parents failed to fill in the whole
questionnairr. In 9 additional families both parents responded on 2 occasions. Data from the 37 families
who reported at one or more time points following the death of their child will be included (maximum
N for women = 37 and for men = 33). The return rate at I , 6 and 13 months were 51%, 35% and 37%
for women, and 50%, 32% and 32% for men.
Based on hospital records, the families of responding (returned the questionnaire one or more times)
and non-responding families were compared on some selected variables. There were no significant
differences between the groups (1 > 0.05, two-tailed test) on variables such as: the child‘s weigth at birth,
the life-span of the child, the mother’s age, the presence of siblings in the family, and whether the family
lived in rural or urban areas. Comparisions on the same variables between the families who responded
only at 1 month, and those who responded at two or three time points, likewise revealed no significant
differences (r > 0.05, two-tailed test).
The mean age was 29.3 years for men and 27.4 years for women. 64.4% lived in urban areas. 16.9%
of all the parents had primary school as their highest level of education, 62.7% had high school or the
equivalent, and 20.3% had a university background.
The sample consisted of 8 families who experienced a SIDS-death and 29 families who experienced a
peri- or neonatal death. Five children died within the first week of life.
zyxw
zyxwvutsr
�zyxwvutsrqp
zyxwvutsrqpo
zy
zy
zy
Sfand J Psycho1 32 (1991)
Parental grief
All parents who had lost children at the Neonatal Intensive Care Unit (NICU) or in SIDS were
offered grief crisis counselling as part of a three year project aimed at supporting families who had lost
newborns and infants. All but 8 families received such intervention. The grief crisis intervention is
described in more detail elsewhere (Dyregrov, 1990).
Measures
zyxwvu
zyxwvut
Questionnaires were distributed at I, 6 and 13 months following the loss. The first questionnaire
contained questions providing sociodemographic information, and questions related to the loss itself,
including the parent’s immediate reactions to the loss and their perception of support from partner and
family. The questionnaires sent out at 6 and 13 months explored the parent’s perception of support from
spouse, family and others, their sense of recovery, and sibling reactions. Questions for the instrument
were based on previous studies concerning parental reactions to the death of a child (i.e. Kennel1 et al.,
1970; Cullberg, 1966; Rowe er ul., 1978; Mandell et al., 1980), and on exploratory interviews and
meetings with parents who had lost a child.
To investigate adaption to the loss over time, 5 inventories measuring different components of grief
were included at all three time points:
1 . The Impact of Event Scale (IES) (Horowitz er al., 1979; Zilberg et ul., 1982) which provides a
2.
3.
4.
5.
195
measure of intrusive thinking (IES-I) and periods of avoidance (IES-A) following traumatic life
events.
The 20 item version of the Goldberg General Health Questionnaire (GHQ) (Goldberg, 1978) was
used to assess psychological impairment of health.
The state version of the State-Trait Anxiety Inventory (STAI X-I) (Spielberger et ul., 1970) was used
to,assess the degree of residual anxiety.
The Bodily Symptom Scale (BSS) (Persson & SjBberg, 1981) was employed to provide a measure of
bodily discomforts.
The short form of the Beck Depression Inventory (BDI) (Beck & Beck, 1972) was employed to
provide a measure of depression.
Mothers and fathers filled out separate questionnaires.
All the inventories used in our study showed adequate psychometric properties (inter-item reliability),
over time. Cronbach’s Alpha varied between 0.81 and 0.97.
Procedure
Whenever possible, parents met with the crisis counsellor (first author) within the first two days after the
death. Contact was not established with 8 families, and these families received no grief follow-up
intervention from the hospital. For anticipated deaths, contact was most often established with parents
prior to the death. Following the death of their child, parents were informed about our effort to gain
more information on parental responses to infant deaths, and that they would receive questionnaires at
1, 6 and 13 months following the death. We stressed that they were free to decline answering the
questionnaire should the questions upset them. Failure to answer the questionnaires was not brought up
in clinical sessions. However, parents received a questionnaire at 6 or 13 months even if they had failed
to respond to an earlier request.
When contact was not established during the first period following the loss, the family received the
questionnaires through the postal service at I, 6 and 13 months. An introductory letter explained the
objectives of the study, i.e. to increase health personnels’ knowledge of family reactions after the loss of
a child, and to improve hospital support for such families. The parents were offered our grief crisis
counselling, as well as other assistance should they need it.
Mothers and fathers received identical questionnaires except that the mother’s questionnaire also
contained questions about sibling reactions, and questions requiring only one of the parents to answer
(factual information). Estimated fill-in time for the questionnaire was 45-60 minutes (somewhat shorter
for the father). As questionnaires were shorter at 6 and 13 months, fill-in time was reduced.
Statistics
T3e data from the questionnaires were coded and entered on a permanent data file. SPSS-X (SPSS inc.,
1983) and MULTIVARIANCE (Finn, 1972) was used for the statistical computations.
�196
zy
zyxwvutsrqpon
zyxwvu
zyxw
zyxwvutsrq
zyxwvutsrqp
A . Dyregrov and S. B. Matthiesen
Scand J Psycho1 32 (1991)
STATE ANXIETY
(STAI
X-1)
GROUPS
.
.
.
I
I
\
I MONTH
0 MONTHS
1) YM
2) T O Y M
3) W.-AT
WORK
4) -.-AT
HOYI
13 MONTHS
RYE
DEPRESSION
(B D 1)
GROUPS
.
I
.
1)MEN
2) -03) T.-AT
WORK
4) W.-AT
HOYI
BODILY SYMPTOMS
(0 5
s>
w
GROUPS
I ) YEN
M
0 ) WOMEN
g so
4
7s
-1
-1
\
b 70
E
-... ...............
...
'21
I:
se
1 M0"M
0 MONTHS
TIYE
13 MONTHS
.
3) W.-AT
WORK
4) w . - A r
HOME
�zyx
zyxwvutsrqp
zyxwvutsrqpon
zyxwv
zyxwv
Scand J Psycho1 32 (1991)
_--
Parental grief
---.
-
197
_.
GENERAL HEALTH
" 0)
(G
13.5
a) WOMEN
.
_1
1.5
3) w.-Ar
WORK
4) W . - A I
AOUC
t
0'
1 MOMH
ia
YOHIHS
1
YO-
TIYE
1 M o m
._.-
Yo-
6
15 Yo-
zyxwvutsrqp
16.0 -
14.5
GROUPS
..
.*.
/
13.0
"
/.
/
m
11'=::
d
g
6.5.'
gz
7.0''
g
/'
.
I
\
'.
\.
.
I
\.
---_-.
1) Mi
2) W O M i
5 ) W.-AT
WORX
4) W.-AT
WOLP
.
*---..
1 41
\
'\Z)
5.5..
4.0
'.
\
'\ 1)
--.-......___.____
31
2.5
"
-5
A
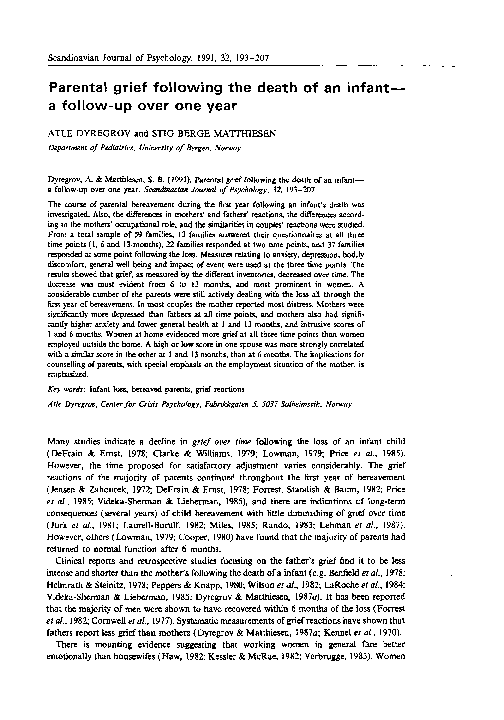
Fig. 1. Mothers' and fathers' grief at I , 6 & 13 months after the death of their child.
�198
zyxwvuts
zy
zyxwvutsrqp
zyxw
A . Dyregrov and S. B. Matthiesen
Scand J Psycho1 32 (1991)
Table I . Number of respondent (N) and mean scores ( M ) for the direrent inventories
1 month
WOMEN
N
M
6 months
N
M
13 months
N
M
STAI X-1
BDI
29
27
28
28
26
27
42.3
7.4
76.9
9.3
17.9
8.8
20
19
19
19
19
20
43.8
6.8
73.7
7.5
15.4
8.5
19
21
19
19
20
20
28
25
26
27
26
27
35.0
3.2
65.7
4.9
11.3
6.3
18
17
18
17
17
18
37.2
3.4
63.7
4.3
11.3
7. I
17
17
17
17
18
18
BSS
GHQ
IES I
IES A
STAI X-l
BDI
BSS
GHQ
IES I
MEN
zyxw
zyxw
Inventory
IES A
38.8
5.1
68.6
5.0
10.7
6.4
32.2
2.8
58.8
2.5
8. I
4.6
RESULTS
37 families (62.7Y0) returned their questionnaire at one or more occasions.
Exact Nand the mean scores for men and women, based upon all available questionnaires
for each of the three time points, are listed in Table 1.
Fig. 1 presents the mean grief scores of men and women at the three time points, as well
as women split into two groupings; those who continued working outside the home and those
who continued working at home.
Womens’ (all women included in one group) and mens’ mean score generally show a
decline over time. The statistical analysis (ANOVA, repeated measures, and MULTIVARIANCE, using Helmert contrasts) are restricted to cases with valid data for all three points
(max. N = 22 for STAI X-1, min. N = 18 for IES-I). The number of respondents included in
the mean scores in Fig. 1 is therefore higher than in the ANOVA and MULTIVARIANCE
analysis. However the means for the total sample and the means from the restricted sample
are similar. The statistical analysis shows that the trend in the data (grief over time) is
basically the same when using the whole or a restricted part of the sample. ANOVA,
repeated measurements, shows that in women, the change in grief score is significant for the
following measures: BDI (F(2/18) = 1.95, p < 0.001), GHQ (F(2/18) = 2.76, p ~ 0 . 0 0 1 )and
IES Intrusion (F(2/16) = 3.82, p < 0.001). Fig. 1 indicates that the reduction in mean grief
scores is most evident among women, with the exception of anxiety where their mean level
rises from 1 to 6 months.
ANOVA, repeated measurements, shows that for men the decline in grief is significant for
the following measures: STAI X-l (F(2/20) = 2.24, p c 0.001), BSS (F(2/16) = 2.52,
p <0.001), GHQ (F(2/16) = 1 . 0 1 , ~<0.05), and IES Intrusion (F(2/16) = 1.88, p <0.001).
The mean levels of anxiety, depression, and avoidance for men rise from 1 to 6 months,
otherwise the levels decline.
Multivariance, using Helmert contrasts, was selected to create a factorial design with sex
as an independent variable. Sex was investigated in relation to two constrast factors: the
difference between time points 1 and 2, summed up for all informants with valid answers on
each of the 3 time points (trend I), and correspondingly, the mean of time point 1 and 2,
.
contrasted to time point 3. However, none of the contrast models for each of the grief
inventories revealed significant overall effects.
zyxwvuts
�zyxwvutsrqponm
zyxwvutsrqp
zyxwvutsrqponm
zyxwvutsrqp
Scand J Psycho1 32 ( 1991)
Parental grief
199
zyxwvuts
Fig. 1 indicates that mens’ and womens’ (all women) mean values differ from each other
at all three time points. There is a parallel drop (and rise in anxiety) in the two sexes’ scores,
and at no time and on no measures is the mean score of fathers higher than that of mothers.
The differences between men and women are significant on the following measures: BDI 1
month (t(2/50) = -2.65, p <0.05), BDI 6 months (t(2/34) = -2.26, p <0.05), GHQ 1
month (t(2/53) = -2.23, p < 0.05), IES Intrusion 1 month (t(2/50) = -2.13, p < 0.05).
The group of women were split into ‘working’ women (employed outside the house) and
housewives, and Fig. 1 shows that women at home have a higher level of distress than their
working counterparts on all measures, at all times. 9 of 18 possible comparisons reveal
significant differences between working women and housewives’ grief scores ( p < 0.05, using
Student t-tests, two-tailed, see note 1 below). Differences are significant for STAI-X-1 (all
time points), BDI (at 6 months), BSS (at 13 months), GHQ (at 6 months). IES Intrusion (at
6 and 13 months), and finally IES A (at 6 months). (For exact f-tests see note 1). For most
measures the housewifes’ mean scores either peak (anxiety, depression, avoidance) or remain
stable (bodily symptoms, general health) at 6 months, but for intrusion the scores indicate a
gradual decline. For working mothers there is a gradual decline from 1 to 13 months, except
for anxiety and intrusion which peaks at 6 months. The score on GHQ drops from 1 to 6
months, and then remains at this level at 13 months.
Working womens’ mean inventory scores are similar to those of men, while housewives
show scores indicating much higher levels of distress. For some of the inventories the
working mothers’ score is below that of men (GHQ, IES Intrusion and IES Avoidance).
In Table 2 we have compared parent’s grief reactions as a couple at I , 6 and 13 months,
using Wilcoxon matched-pairs signed ranks test. For all inventories, at all time points, there
is a majority of couples where the mother has a higher score than her spouse, except for
bodily symptoms at 6 months where the couples’ score is equally distributed between
mothers and fathers. In a majority of the couples it is the mother that indicates most distress.
For depression the difference is significant at all three time points, for anxiety and general
health it is significant at 1 and 13 months, and for intrusion at 1 and 6 months. In spite of
these general results, however, it should be noted that the fathers in many couples indicate
more distress than the mother.
For BDI (short version) a cutoff point score of 4 was used to identify those who evidenced
mild, moderate or severe depression (Beck & Beck, 1972). We found that more women than
men evidenced some form of depression at all three time points (see Table 3). The majority
of women were above the cutoff point for depression all through the first year of bereavement,
while 1/4 to 1/3 of the men were above this point. For both sexes there were more persons
above the cutoff point at 6 months than at the other two time points.
With a a cutoff score of 4 in the GHQ (Goldberg, 1978), Table 3 shows that there is a
decline over time in the percentage of men who score above the cutoff level. The percentage
of women who score above the cutoff point remains the same from 1 to 6 months, with some
decline at 13 months. There are more women than men who score above the cutoff point at
all three time points.
zyxwvutsrqpo
zyxwvuts
zyxwvu
zyxw
‘Significant t-tests between working women and housewives grief scores
STAI X-1: t = -3.05, d f = 1/27, p(O.01 ( I month), f = -2.97, d f = 1/18, p <O.O ( 6 months),
t = -2.37, df = 1/17,p < 0.05 (13 months).
BDI:
t = -2.41, df = 1/17, p < 0.05 ( 6 months).
BSS:
t = -2.36, d f = 1/17. p <0.05 (13 months).
GHQ:
t = -2.84, df = 1/17, p < 0.05 ( 6 months).
IES I:
t = -3.35, df = 1/24, p ~ 0 . 0 1
( I month), f = -2.66, df = 1/18. p < 0.05 (13 months)
IES A:
f = -2.98, df = 1/18, p < 0.01 (6 months).
�200
zyxwvutsrq
zyxwvut
zyxwvutsrq
zy
zy
A . Dyregrov and S. B. Matthiesen
Scand J Psycho1 32 (1991)
Table 2. Comparison of parent's grief reactions 1, 6 and 13 months ajier the loss. Diferences on
inventories tested for significance by the use of Wilcoxon matched-pairs signed ranks test for related
samples
Direction of differences
Father
highest score
Mother
highest score
Wilcoxon
zyxwvutsrq
Inventory
STAI
BDI
BSS
GHQ
IES-I
IES-A
STAI
BDI
BSS
GHQ
IES-I
IES-A
STAI
BDI
BSS
GHQ
I Month
8
2
6
6
20
17
15
19
17
8
18
10
6 Months
7
Equal score
- 1.97.
- 3.28***
- 1.91
-3.07'.
-2.55..
- 1.74
- 1.09
9
13
8
2
8
4
4
-
2.27*
-0.78
-1.73
-2.12*
-0.16
10
12
8
8
z
zyxwvuts
zyxwvutsrqpo
13 Months
3
3
7
3
-2.63**
-2.42.
- 1.73
-2.23.
14
11
9
I1
*p < 0.05; **p < 0.01; ***p < 0.001
Table 3. Percentages of men and women above the recommended cutofpoints' at I , 6 and I3 months
following an insant loss
1 month
Inventory'
~
~
~~
6 month
13 months
men
women
men
women
men
women
28
41
54(19)
26( 4)
52
57
69(42)
33(7)
35
29
47( 12)
12(6)
63
58
79(21)
25( 10)
24
18
28(6)
17(0)
57
41
40(20)
20(5)
~
Depression (BDI)
General health (GHQ)
Intrusion3 (IES-I)
Avoidand (IES-A)
'For BDI and GHQ the recommended cutoff score is 4. For the IES the low distress score is less than
9, medium distress score from 9 to 19, the high distress score is above 19. *N for the different time points
are Found in Table 1. 'High and medium distress levels combined, with high distress only in parenthesis.
When using Horowitz' (1982) criteria for high (more than 19). medium (9-19) and low
distress (less than 9) levels, we again found that for intrusion more women than men had a
high or medium level of distress at all three time points. For both sexes there is a drop in
distress from 6 to 13 months. 40% of the women still experience high or medium levels of
intrusive distress at 13 months.
The percentages scoring above the cutoff points are lower for avoidance than for intrusion.
Although womens' scores exceed men at all three time points, the differences are less
�zyxwvutsrqpo
zyxwvutsrqp
zyx
zyxwvutsrqp
Parental grief
Scand i Rychol 32 (1991)
201
Table 4. Rank order correlation (Speormons rho) between fathers' and mothers' grief (the spouses in each
couple is compored directly) for those poirs that completed the questionnaire ot I , 6 and 13 months
zyxwvu
zyxwvut
zyxwv
zyxwvuts
zyxwvutsr
Inventories
Father vs. mother'
1 month
6 months
13 months
IES
IES
Intrusion
Avoid.
0.44**
0.18
0.27
0.30
0.33
0.34
0.17
0.22
0.15
STAI X-1
BDI
BSS
GHQ
0.31*
0.06
0.25
0.43**
0.32
0.35'
0.16
0.37.
0.50.'
'At 1 month N varies between 25 and 28, at 6 months N vanes between 15 and 18, and at 13 months
N vanes between 16 and 18.
*p < 0.05; * p c 0.01; ***p < 0.001, two-tailed test.
pronounced. While the percentage of women indicating distress decreases, there are more
men who indicate distress at 13 months than at 6 months.
The spouses grief reactions correlated significantly in 4 out of 6 inventories at 1 month
following the loss, none at 6 months, and 2 at 13 months (see Table 4). This indicates that
the spouses tend to have similar grief reactions early following bereavement, more dissimilar
reactions at 6 months, and somewhat more similar reactions at 13 months.
The subjects who received grief intervention experienced significantly less anxiety (STAI
X-1) at 1 month (t(2/55) =2.10, p <0.05) and 13 months (f(2/34) =2.30, p <0.05), and
significantly more bodily symptoms (BSS) at 13 months (t(2/34) =2.58, p <0.05) and
intrusive thoughts (IES-Intrusion) at 1 month ( t ( 2/50) = 2.72, p < 0.05) than those who did
not receive grief intervention.
The reactions of parents in families with a living child did not differ significantly from
families without children, except from mothers with living children who reported significantly
more depression at 6 months than those without children (F = 7.12, df 1/15, p < 0.05). There
were no significant differences on the 5 inventories between those parents expecting a new
child, and those who did not.
DISCUSSION
Resolution of grief over time
Grief, as measured by different inventories, showed decrease over time. The decrease was
most prominent in women. When the decline in mean grief scores and the decline in
percentages scoring above cut-off points are considered together, the decline in grief reactions
is most evident from 6 to 13 months.
If we compare the mean values found at 13 months in this study with the mean values
found in an earlier retrospective study where data were collected with the same measures at
a mean of 27 months following the death (Dyregrov & Matthiesen, 1987a), we find that the
mean scores in the retrospective study are somewhat lower, but not much. This can,
cautiously, be taken as an indication that by 13 months much of the adaption to the loss has
taken place. The recovery process for the parents in this study may have been accelerated as
a majority of the parents received grief crisis intervention. However, the results show that
although the parents who received grief intervention reported less anxiety at 1 and 13
months, they also reported more intrusive thoughts at 1 month and more bodily symptoms
at 13 months. As the majority of parents received intervention, and only 8 couples did not,
it is premature to draw firm conclusions based on these results.
�202
zyxwvutsrqpo
zyxwvu
zyxwvutsr
zy
zy
zyxwvutsr
A. Dyregrov and S. B. Matthiesen
Scand J Psycho1 32 (1991)
Anxiety did not show the same decline pattern as the other measures. We have previously
documented that anxiety constitutes a special problem for parents that have lost a child
(Dyregrov & Mathiesen, 1987b). Their illusion of invulnerability is shattered and they expect
the worst to happen, and their anxiety is increased by hearing or reading of other peoples’
misfortunes.
The mean STAI X-1 scores for women at 6 months in this study were quite similar to
those found by Rubin (1982) in his investigation of grief reactions in mothers 7 months after
the loss of an infant. Rubin found a mean STAI X-1 score of 45.0 in women who had lost
children an average of 7 months earlier, while our womens’ mean STAI X-1 score at 6
months follow up were 43.8 (SD = 14.4). Rubin (1982) also studied a group of women who
had experienced a loss about 52 months earlier, and found a STAI X-1 score that was almost
identical to the mean STAI X-1 score found in mothers in our retrospective study (see
Dyregrov & Matthiesen, 1987~)where about 27 months had elapsed since the death. Both
Rubin’s and our own findings indicate that bereaved mothers’ anxiety scores remain elevated
for years following the loss.
The level of state anxiety reported in normative population samples vanes around a score
of 30 (Speilberger et al., 1970). In a discussion of the Norwegian version of the STAI X-1,
Weiszth (1984) argued that there was a tendency to rate one’s anxiety too low in a
Norwegian sample. According to Weiszth, the Norwegian baseline state anxiety score was
somewhat lower than the U.S normative samples.
We found that the loss of a child resulted in increased anxiety among parents (especially
in housewives), well above normative samples, and that this anxiousness continued during
the first year of bereavement.
The mean scores on the Bodily Symptoms Scale were above those found in a ‘normal’
group, and a group suffering from chronic disease (chronic rheumatism) in a Swedish study
(Persson & Sj~berg,in press). The scores of the bereaved parents on the Impact of Event
Scale, especially for intrusion, were mostly above those found in a Norwegian prospective
study which measured intrusion and avoidance within 7 days, at 6-9 months, and 24 years
following adults’ hospitalization for accidental injury (Malt, 1988).
The percentage of persons scoring above the cutoff points for both depression and general
health, as well as the percentage experiencing high to medium degrees of intrusiveness, are
relatively high, suggesting that many bereaved parents show little evidence of resolution
within 13 months. A considerable number of the parents still seemed to be actively dealing
with the loss all through the first year of bereavement.
zyxwvutsrq
zyxwvuts
Differences in mothers’ and fathers’ grief score
As in our retrospective study (Dyregrov & Matthiesen, 1987a), we found mothers reporting
more distress than fathers. Wilcoxon signed rank test also revealed that for all inventories,
at all three time points, except bodily symptons at 6 months, there were more couples where
the mother had a higher score than the father.
Fathers were much more reluctant to express their feelings than mothers both verbally and
in writing. While mothers often cried in the clinical sessions, fathers almost never did this. On
the questionnaires many mothers wrote long accounts on how they had experienced different
aspects of the loss, while fathers usually gave brief ‘matter of fact’ answers. Although both
women and men more freely reported their reactions in clinical encounters than in question. naires, our impression is, in line with others (e.g. Mandell et al., 1980). that fathers’ grief
often goes unarticulated. Fathers have generally more difficulties in setting words to their
emotions. Although employed women had similar grief scores to the men on the inventories,
�zyxwvutsrqponm
zyxwvutsrqp
zyxwvutsrqpon
zy
Scand J Psycho1 32 (1991)
zyxw
Parental grief
203
they did not differ from women who stayed at home concerning their verbalization of
emotions throughout the clinical follow-up.
Data from the child bereavement literature (Tudehope et al., 1986; Nixon & Pearn, 1977;
Mandell et al., 1980; Wilson er al., 1982), and from other crisis situations, such as having a
child with cancer (Cheder & Barbarin, 1984), also suggests that fathers avoid dealing with
their own feelings and utilize their support systems less than mothers. Furthermore, men may
have more difficulty in asking for intimate emotional help, or being open to such help, than
women (Gourash, 1978). The males’ images of strength, family leadership, and being
emotionally unaffected, seems to prevent them from expressing their needs and receiving help
when needed, while it is more socially acceptable for women to express various emotions. It
is also our impression that the social environment is more focused on the mother’s reactions,
and thus the father’s needs are more unrecognized.
It has been speculated whether men are more able to distort the situation in the face of a
stressful experience than females (Sowa & Lustman, 1984). The opportunity to concentrate
on other aspects of life may be a function of one’s occupational (or social) role, more than
inborn or socialized traits.
In several couples men scored higher than women on the inventories, so it is probably not
male inexpressiveness but masculine inexpressiveness that is the operable phenomenon, as
Ganong & Coleman (1985) emphasize. Sex-role orientation in males and females would
probably have been more significant in determining how freely emotions were expressed. In
forthcoming studies we need to include measures on sex-role orientation.
Employed mothers us. housewives
We found that the housewives were more distressed than their working counterparts on all
measures. The scores of men and working women were similar on most measures. However,
these results, and the following discussion must be viewed in light of the small number of
women in the two groups, and the lack of background data regarding their occupational
choices. There were almost no changes in the occupational status of the mothers following
the loss.
The loss of a child may signify less threat to the self of the working mother than the
housewife, as their self-image and self-respect also are tied to their occupational role in
addition to their role as mothers. The loss of a child threatens the housewives’ primary role,
and may influence her sense of worth as a mother and a women. Do housewives place more
value on children, become more attached to them, and are they willing to sacrifice more for
them? If so, one would expect more distress following a loss.
The data from this study show that mothers who return to work have a grief pattern, as
reflected in the inventory scores over time, which are similar to fathers. A job confronts the
parent with situational demands that must be met and these are apt to draw one’s attention
from personal troubles. Returning to work can therefore influence distress level by keeping
parents from ruminating about the loss and keeping their thoughts on other issues.
Verbrugge (1983) notes that health risks may generally be lower for socially active than for
less active people, and that activity level associated with a job leads to less time spent on
anxious or depressed states.
In several studies it has been commented on the mothers’ loneliness and isolation when
staying at home following their child’s death (Stringham et ul., 1982). There is a tendency for
mothers to isolate themselves from their social environment (Berg et uf., 1978). This social
isolation may be a health hazard for housewives (Lopata, 1971). An inadequate social
network appears to place housewives in special jeopardy when they are faced with a
crisis-especially a marital crisis (Brown & Hams, 1978).
zyxw
�204
zy
zyxwvu
zyxwvutsrqp
zyxwvu
A . Dyregrov and S. B. Matthiesen
S c a d J Psycho1 32 (1991)
Housewives experienced more intrusive thoughts than working mothers. In fact the lowest
level of intrusiveness experienced by housewives (at 13 months), was higher than the highest
level experienced by working mothers (at 6 months). Preoccupation with thoughts about the
lost child hinders relinquishment of the attachment, a part of the grief work considered
neceSSary to adapt to the loss. Furthermore housewives are usually faced with a social
environment where they are constantly reminded of their loss. Videka-Sherman (1982) found
that persistant preoccupation with the death was associated with persisting depression.
The demands on housewives with children at home may be especially hard, as attending to
the needs of surviving children can indeed be stressful for mothers (Dyregrov, 1990). The
sample was too small to further split it into working mothers with and without children at
home and employed women with and without children. However, there was little difference
between women with alive children compared to women without living children, except for
significantly more depression at 6 months for mothers of living children. A study with a
larger number of respondents is called for to differentiate the effects of living children and
employment status on the reactions of bereaved parents.
SeIective factors may also account for some of the differences between housewives and
working mothers. The mothers who enter and keep a job may be more “healthy” Originally.
The difference may also reflect other differences between working women and women in the
housewife role. Due to lack of background data, the study does not permit firm conclusion
in this area.
clinically we have not noted any difference between housewives and working women in
their ability to express emotions and thoughts about the loss. We therefore believe that these
two groups of women similarly express their emotions, even though one group returns to
work. This indicates that the role of the work place as a potential for social support for
people in crisis should be more emphasized, and studied in more depth. Specifically, we need
to know if the two sexes differs in utilizing social support at their work place.
The low number of women in the two groups, and the existence of several competing
hypotheses for the differences between the two female groups, call for systematic research in
this specific area.
zyxwvuts
zyxwvut
zyxwvu
Grief c o r r e s p o h c e within the couples
As in our retrospective study (Dyregrov & Matthiesen, 1987a), we again found that the
spouses’ grief reactions are correlated, as others also have found (Benfield et a/., 1978). This
suggests that the spouses influence each other’s grief and that there may be family patterns
of grieving. 6 months following the loss the two spouses’ reaction differed most. This suggests
that there is a period in the first year of bereavement when spouses are less well syncronized
in their grief. This should be taken into account when counselling efforts are considered. This
is a period when mothers often complain bitterly to the counsellor about the lack of support
they receive from their social network-and when the father is sometimes felt to “join the
opposition”.
Methoabgical comments
The results presented here are based on a relatively small sample, with a high attrition rate
which also increased with time. The attrition rate is high( er) in other comparable studies (e.g.
Cooper, 1980; Videka-Sherman, 1982). In a follow-up study Videka-Sherman (1982) surveyed parents at two time points following a child loss, and only 17% of her original parents
- answered at the second time point. From other research on bereavement it is known that
non-responders usually are more emotionally affected following a loss than responders
(Clarke & Williams, 1979; Cooper, 1980; Lehman et a[., 1987). If so, our results may be
�zyxwvutsrqpon
zyxwvutsrqpo
zy
zy
Scand J Psycho1 32 (1991)
Parental grief
205
biased towards a better adjustment in parents than what would have been expected if all
parents returned their questionnaires throughout the study period. However, analyses
showed that there were no differences on the grief inventories between parents who only
responded at 1 month, compared to those who answered several times.
CONCLUSION
zyxwvuts
1. There is a reduction in grief scores over the first year. However, the decline is largest from
6 to 13 months, and the reduction is largest in women. 2. On most measures the mother
reports more grief than the father at the three time points. 3. The mother‘s grief reactions
differ according to their occupational role. Mothers occupied outside the home report less
grief than housewives. 4. The spouses reactions were found to correlate more at 1 and 13
months than at 6 months.
The results presented here have implications for the counselling of parents who have lost
children. Although there is a decline in grief over time, there are a considerable number of
parents who experience distress more than a year following their loss. Bereavement counselling programs have to address the need for long-term follow-up as well as the different
needs of those employed outside the home and those working at home. In particular there is
a need to note that housewives as a g o u p are more at risk for developing adverse reactions
as a consequence of their loss than women employed outside the home. Individual counselling aimed at reducing parents’ distress needs to be sensitive to this. When the mother
stays at home following the loss, the discrepancy between the mother’s and the father’s grief
will be most pronounced, and one would expect the risk of marital difficulties to be greater.
Periodical follow-up with families should therefore be arranged.
zy
Both the empirical research and the clinical experience reported here is based on work completed during
a Post-graduate Clinical Research Fellowship awarded to the first author by the Norwegian Research
Council for Science and the Humanities (NAVF‘). The authors are especially indebted to assitant
professor Hhkan Sundberg of the Department of Physiological Psychology at the University of Bergen
whose methodological and scientific knowledge has been of invaluable help. For their contribution to the
methodology and structure of the article we would also like to thank the following persons from the
Faculty of Psychology at the University of Bergen; professor Holger Ursin of the Department of
Physiological Psychology, assistant professor Knut Hagtvedt of the Department of Psychometrics, and
professor Leif Edvard Aare of the Department of Social Psychology and Organizational Psychology.
Former students, now psychologists, Ingeborg Huglen, &nte Lomeland and Astrid Rbberg are
acknowledged for stimulating us to take a closer look at the differences between employed women and
housewives.
zyxwvutsr
REFERENCES
Beck, A. T. & Beck, R. W. (1972). Screening depressed patients in family practice. Postgruduare
Medicine, 52, 81-85
Benfield, D. G., Leib, S. A. & Vollman, J. H. ( 1978). Grief nsponse of parents to neonatal death and
parent participation in deciding care. Pediatrics, 62, 171-177.
Berg, U., Ekenstein, G., Hojer, B., Sandros, I. & Tunell, R. (1978). Information cch stM ti1 foraldrar
som forlorat sitt barn vid fdelsen. Liikartidningen, 75, 128-132.
Bimbaum, J. A. (1975). Life patterns and self-esteem in gifted family-oriented and career-comitted
women. In M. T.S. Mednick, S. S. Tangri, & L. W. Hoffmann (Eds) Women und achievement: Social
and motivational unulyses. Washington D.C.: Hemisphere.
Brown, G. & Hams, T. (1978). Socinl origins of &pression: A study of psychintric disorder in women.
New York: Free Press.
Chesler, M.A. & Barbarin, 0. A. (1984). Difficulties of providing help in a crisis: Relationships between
parents of children with cancer and their friends. Journal of Social Issues, 40, 113-134.
�206
zy
zy
zyxwvu
zyxwvutsrqp
zyxwvutsrqp
zyxw
A . Dyregrov and S. B. Matthiesen
Scand J Psycho1 32 (1991)
Clarke, M. & Williams, A. J. (1979). Depression in women after perinatal death. Luncet, April 28,
916-91 7.
Cooper. J, D. (1980). Parental reactions to stillbirth. British Journal of Social Work, 10, 55-69.
Cornwell, J., Nurcombe, B. & Stevens, L. ( 1977). Family response to loss of a child by sudden infant
death syndrome. The Medical Journal of Australia, I , 656-659.
Cullberg, J. (1966). Reaktioner infor perinatal bamadBd (I): Psykiska foljder hos kvinnan. Liikartidnigen, 63, 3980-3986.
DeFrain. J. D. & Emst, L. (1978). The psychological effects of sudden infant death syndrome on
surviving family members. Journal of Family Practice, 6, 985-989.
Dyregrov, A. (1988). The loss of a child. The siblings’ perspective. In J. Kumar & I. Brockington (Eds),
Motherhood and mental illness 2. London: Wright.
Dyregrov, A. (1990). Crisis intervention following the loss of an infant child. Bereavement Care, Winter.
Dyregrov, A. & Matthiesen, S. B. (1987~). Similarities and differences in mothers’ and fathers’ grief
following the death of an infant. Scandinavian Journal of Psychology, 28, 1- 15.
Dyrcgrov. A. t Matthiesen, S. B. (19876). Anxiety and vulnerability in parents following the death of
an infant. Scandinavian Journal of Psychology, 28, 16-25.
Finn. J. D. ( 1972). Multivariance, univuriate and multiuariate anulysis of varimrce, covariance, and
regression. Version V . Ann Arbor, Michigan: National Educational Resources.
Forrest, G. C., Standish, E. & Baum, J. D. (1982). Support after perinatal death: A study of support and
counselling after perinatal bereavement. British Medical Journal, 285, 1475-1479.
Ganong, L. H. & Coleman, M. (1985). Sex, sex roles, and emotional expressiveness. The Journal of
Generic Psychology, 146, 405-41 1.
Goldberg. D. ( 1978). Manual of the General Health Questionnaire. Windsor: NFER.
Gore, S. & Mangione, T. W. (1983). Social roles, sex roles and psychological distress, additive and
interactive models of sex differences. Journal of Health and Social Behavior, 24, 300-312.
Gourash, N. ( 1978). Help-seeking: A review of the literature. American Journal of Community Psychology, 6, 413-423.
Haw, M. A. (1982). Women, work and stress: A review of agenda for the future. Journal of Health and
Social Behavior, 23, 132- 144.
Helmrath, T. A. & Steinitz, E. M. (1978). Death of an infant: Parental grieving and the failure of social
support. Journal of Family Practice, 6, 785-790.
Horowiy M. J. (1982). Stress response syndromes and their treatment. In L. Goldberger & S. Bresnitz
(Eds), Handbook of stress-Theoretical and clinical aspects. New York: The Free Press.
Horowitz. M. J., Wilner. N., & Alvam, W. (1979). Impact of event scale: A measure of subjective stress.
Psychosomatic Medicine, 41,209-218.
Jensen, J. S. & Zahourek, R. (1972). Depression in mothers who have lost a newborn. Rocky Mountain
Medical Journal, 69, 61 -63.
Jurk, I. H., Ekert, H. & Jones, H. J. (1981). Family responses and mechanisms of adjustment following
death of children with cancer. Australian Paediarric Journal, 17. 85-88.
Kennel, J. H.,Slyter, H. 8 Klaus, M. H. (1970). The mourning response of parents to the death of a
newborn infant. New England Journal of Medicine, 238, 344-349.
Kessler, R. C. & McRae, J. A. (1982). The effect of wives’ employment on the mental health of married
men and women. American Sociological Review, 47, 216-221.
LaRoche, C., Lalinec-Michaud, M., Engelsmann, F., Fuller, N., Copp, M. & McQuarde-Soldatos, L.
(1984). Grief reactions to perinatal death-a follow-up study. Canadian Journal of Psychiarry, 29.
zyxwvutsrqp
zyxwvuts
zyxwvut
14-19.
Laurell-Bodf, Y . ( 1982). Kris16sning i Idngtidsperspektiu. Lund: Studentlitteratur.
Lehman, D. R., Wortman, C.B. & Williams, A. F. (1987). Long-term effects of losing a spouse or child
in a motor vehicle crash. Journal of Personality and Social Psychology, 52, 218-231.
Lopata, H. Z. (1971). Occupation: Housewife. New York Oxford University Press.
Lowman, J. (1979). Grief intervention and sudden infant death syndrome. American Journal of
Community Psychology, 7, 665 -677.
Malt, U. (1988). The long-term psychiatric consequences of accidental injury. A longitudinal study of
107 adults. British Journal of Psychiatry, f53,810-818.
F., McAnulty, E. & Rcax, R. M. (1980). Observations of parental response to sudden
Mandell,
.
unanticipated infant death. Pediatrics, 65, 221-225.
Miles, M. S. (1985). Emotional symptoms and physical health in bereaved parents. Nursing Research, 34,
76-81.
�zyxwvutsrqponml
zyxwvutsrqp
zyxwvutsrqpo
zy
zy
zyxwvutsrqp
Scand J Psycho1 32 (1991)
Parental grief
207
zyxwvut
Nixon, J. & Pearn, J. (1977). Emotional sequelae of parents and sibs following the drowning or
near-drowning of a child. Australian and New Zealand Journal of Psychiairy, 11, 265-268.
Peppers, L. G. & K ~ p p R.
, J. (1980). Maternal reactions to unvoluntary fetal/infant death. Psychiatry,
43, 155-159.
Persson, L-0. & Sj6berg, L. ( 1981). Mood and body feelings. Department of Psychology, University of
Gciteborg, Sweden.
Persson. L-0. & SjGberg. L. Mood and somatic symptoms. Journal of Psychosomatic Research, in press.
Price, M., Carter, B. D., Shelton, T. L. & Bendell, R. D. ( 1985). Maternal perceptions of Sudden Infant
Death Syndrome. CHC, 14, 22-31.
Rando, T. A. ( 1983). An investigation of grief and adaption in parents whose children have died from
cancer: Journal of Pediatric Psychology, 8, 3-20.
Rowe, J., Clyman, R., Green, C., Mikkelsen, C., Haight, J. & Ataide, L. (1978). Follow up of families
who experience a pennatal death. Pediatrics, 62, 166-170.
Rubin, S. (1982). Persisting effects of loss. A model of mourning. Series in Clinical Community
Psychology: Stress and anxiety, 8,275-282.
Spielberger, C. D., Gorsuch, R. L. & Lushene, R. E. (1970). Manual for ihe Siaie-Trait Anxiety
Inventory. Palo Alto: Consulting Psychologists Press.
Sowa, C . J. & Lustman, P. J. (1984). Gender differences in rating stressful events, depression. and
depressive cognition. Journal of Clinical Psychology. 40, 1334- 1337.
SPSS Inc. ( 1983). SPSS-X. Users guide. A complete guide io SPSS-X lunguage und operations. New
York: McGraw-Hill.
Stringham, J. G., Riley, J. H. & Ross, A. ( 1982). Silent birth: mourning a stillborn baby. Social Work,
27. 322-327.
Tudehope, D. I., Iredell, J.. Rodgers, D. & Gunn, A. (1986). Neonatal death: grieving families. Medical
Journal of Ausiralia, 144, 290-292.
Verbrugge. L. M. ( 1983). Multiple roles and physical health of women and men. Journal of Health and
Social Behavior. 24, 16-30.
Videka-Sherman, L. (1982). Coping with the death of a child: A study over time. American Journal of
Orihopsychiairy, 52, 688-698.
Videka-Sherman, L. & Lieberman, M. ( 1985). The effects of self-help and psychotherapy intervention on
child loss: The limits of recovery. American Journal of Orthopsychiairy. 55, 70-82.
Weissth L. ( 1984). Stress reaciions to an indusirial disaster. Oslo: Division of Disaster Psychiatry,
Institute for Psychiatry, Gaustad & The Psychiatric Institute, Vinderen. University of Oslo & The
Joint Nonveigan Armed Forces Medical Services.
Wilson, A. L., Fenton, L. J., Stevens, D. C. & Soule, 0. J. (1982). The death of a newborn twin: An
analysis of parental bereavement. Pediatrics, 70, 587-59 I.
Zilberg. N. 1.. Weiss, D. S. & Horowitz, M. J. ( 1982). Impact of event scale: A cross-validation study
and some empirical evidence supporting a conceptual model of stress response syndromes. Journal of
Consulting and Clinical Psychology, 50, 407-414.
Received 13 December 1988
�
 Atle Dyregrov
Atle Dyregrov