Comment
Health risks of climate change: act now or pay later
www.thelancet.com Vol 384 September 20, 2014
measures that will reduce the damage to health caused by
climate change, to which the world is already committed.
Society also needs to prepare for the possibility of more
serious changes later in the century. For example, in the
next 20–30 years, net global food production might be
maintained as a result of increased crop yields in cooler,
high latitudes. However, continued warming after
2050 would adversely affect crop yields in most parts
of the world, at a time when demand for food will be
rising strongly due to projected population growth and
economic development.6
Both a high absolute level and a rapid rate of global
climate change will severely test biological and social
mechanisms for adaptation, with limits to adaptation
becoming increasingly evident. Examples range from
emergency preparedness in the face of shortening
return periods after potentially catastrophic floods,
to saltwater intrusion into freshwater lenses in small
islands which would potentially compromise water
quality to such an extent that migration might be the
only option.7 Furthermore, limits to adaptation will
arise when hazards associated with a changing climate
6·0
Global average surface temperature change (°C)
There is growing scientific consensus that climate change
is happening, is largely human induced, and will have
serious consequences for human health. The impact
of climate change on global health is probably not yet
large, compared with major risk factors, but will become
greater later in this century, especially if the world follows
one of the so-called high-end emission pathways, such
as Representative Concentration Pathway (RCP) 8·5,
outlined in the UN Intergovernmental Panel on Climate
Change (IPCC) Fifth Assessment Report.1,2
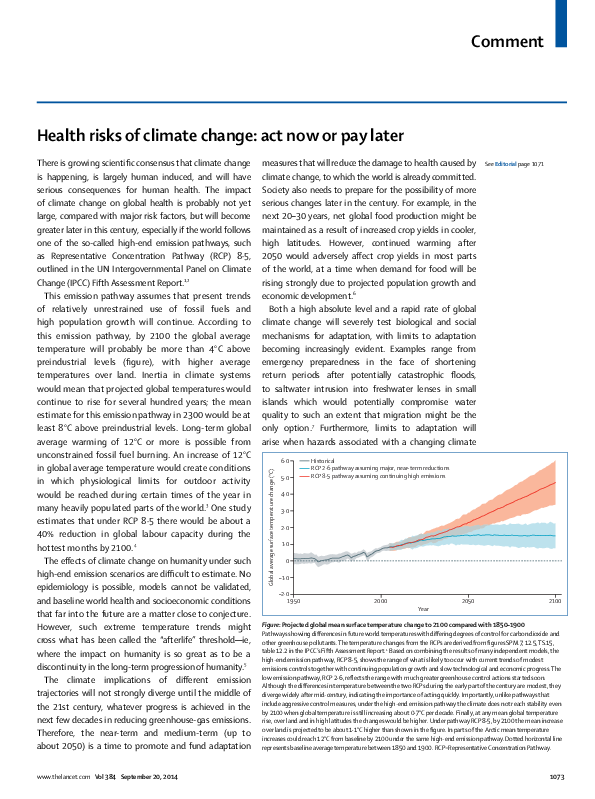
This emission pathway assumes that present trends
of relatively unrestrained use of fossil fuels and
high population growth will continue. According to
this emission pathway, by 2100 the global average
temperature will probably be more than 4°C above
preindustrial levels (figure), with higher average
temperatures over land. Inertia in climate systems
would mean that projected global temperatures would
continue to rise for several hundred years; the mean
estimate for this emission pathway in 2300 would be at
least 8°C above preindustrial levels. Long-term global
average warming of 12°C or more is possible from
unconstrained fossil fuel burning. An increase of 12°C
in global average temperature would create conditions
in which physiological limits for outdoor activity
would be reached during certain times of the year in
many heavily populated parts of the world.3 One study
estimates that under RCP 8·5 there would be about a
40% reduction in global labour capacity during the
hottest months by 2100.4
The effects of climate change on humanity under such
high-end emission scenarios are difficult to estimate. No
epidemiology is possible, models cannot be validated,
and baseline world health and socioeconomic conditions
that far into the future are a matter close to conjecture.
However, such extreme temperature trends might
cross what has been called the “afterlife” threshold—ie,
where the impact on humanity is so great as to be a
discontinuity in the long-term progression of humanity.5
The climate implications of different emission
trajectories will not strongly diverge until the middle of
the 21st century, whatever progress is achieved in the
next few decades in reducing greenhouse-gas emissions.
Therefore, the near-term and medium-term (up to
about 2050) is a time to promote and fund adaptation
5·0
See Editorial page 1071
Historical
RCP 2·6 pathway assuming major, near-term reductions
RCP 8·5 pathway assuming continuing high emissions
4·0
3·0
2·0
1·0
0
–1·0
–2·0
1950
2000
2050
2100
Year
Figure: Projected global mean surface temperature change to 2100 compared with 1850–1900
Pathways showing differences in future world temperatures with differing degrees of control for carbon dioxide and
other greenhouse pollutants. The temperature changes from the RCPs are derived from figures SPM.7, 12.5, TS.15,
table 12.2 in the IPCC’s Fifth Assessment Report.1 Based on combining the results of many independent models, the
high-end emission pathway, RCP 8·5, shows the range of what is likely to occur with current trends of modest
emissions controls together with continuing population growth and slow technological and economic progress. The
low emission pathway, RCP 2·6, reflects the range with much greater greenhouse control actions started soon.
Although the differences in temperature between the two RCPs during the early part of the century are modest, they
diverge widely after mid-century, indicating the importance of acting quickly. Importantly, unlike pathways that
include aggressive control measures, under the high-end emission pathway the climate does not reach stability even
by 2100 when global temperature is still increasing about 0·7°C per decade. Finally, at any mean global temperature
rise, over land and in high latitudes the changes would be higher. Under pathway RCP 8·5, by 2100 the mean increase
over land is projected to be about 1·1°C higher than shown in the figure. In parts of the Arctic mean temperature
increases could reach 12°C from baseline by 2100 under the same high-end emission pathway. Dotted horizontal line
represents baseline average temperature between 1850 and 1900. RCP=Representative Concentration Pathway.
1073
�Comment
interact with inappropriate development pathways—eg,
where building occurs on flood plains. Adaptation limits
might also occur when health systems fail to proactively
design and implement adaptation actions needed to
address a particular health risk. The need to strengthen
health-system capacity in low-income countries to
prepare for, cope with, and recover as far as possible from
the health effects of climate change that do occur could
be partly addressed by equitable partnerships between
high-income and low-income countries.
The health community has a role in the promotion
of policies to reduce emissions of all climate-active
pollutants, both because many of these pollutants are
health hazards now and because all push the climate
towards possible extremes within this century. Major
reductions in mortality would ensue from measures
to reduce combustion of carbon-containing fuel and
consequent carbon dioxide and fine particle emissions,
for example by curbing coal combustion. Furthermore,
there are co-benefits for both health and climate
from actions to reduce short-lived climate pollutants,
such as black carbon and methane, the second most
important greenhouse gas and the primary precursor
to ozone in the lower atmosphere.8,9 Provision of wider
access to reproductive health services could also reduce
carbon dioxide emissions over the century and improve
maternal and child health.10
Wise policies to develop low-emission economies
that use the full range of available technological options
would provide many societal benefits and only have
moderate impacts on economic growth projections.9
Nevertheless, such changes tend to be opposed by those
with a stake in current economic pathways.
The burden of disease and injury due to climate change
falls mainly on specific vulnerable groups, particularly
those living in poverty. Vulnerability to climate change is
in many cases inversely related to historical greenhouse
gas emissions. Thus, the responsibility for leading
policies to reduce these emissions should be shouldered
by those nations and commercial interests that have
enjoyed the benefits of fossil-fuel-driven development.
Since emerging economies are responsible for a growing
proportion of emissions, however, they too must
move towards development with low greenhouse gas
emissions, which some are starting to do.
The timescale is daunting but not a reason for
inaction: the health community needs to argue for
1074
a long-term perspective on climate change. Article
2 of the United Nations Framework Convention on
Climate Change states that the objective is to avoid
dangerous anthropogenic interference with the Earth’s
climate.11 Without decisive action this objective cannot
be achieved. The world’s carbon budget to keep global
increases in temperature below 2°C is likely to be
exceeded by 2040.9 Society must, therefore, enhance
efforts to adapt to reduce adverse effects on human
health, particularly for the most vulnerable. The prospect
of extreme climates beyond mid-century, however,
should impel the health community to promote deep
cuts in emissions of climate-active pollutants now for the
long-term protection of human welfare, starting with
co-benefit actions that protect both health and climate.
*Andy Haines, Kristie L Ebi, Kirk R Smith, Alistair Woodward
Departments of Social and Environmental Health Research and
Population Health, London School of Hygiene & Tropical Medicine,
London WC1H 9SH, UK (AH); Department of Global Health,
University of Washington, Seattle, WA, USA (KLE); School of Public
Health, University of California Berkeley, Berkeley, CA, USA (KRS);
and School of Population Health, University of Auckland,
Auckland, New Zealand (AW)
andy.haines@lshtm.ac.uk
The authors were members of the UN Intergovernmental Panel on Climate
Change Fifth Assessment Report and contributed to chapter 11 on human
health. This Comment represents their own views and not necessarily those of
the UN Intergovernmental Panel on Climate Change.
1
2
3
4
5
6
7
8
Stocker TF, Qin D, Plattner G-K, eds. IPCC, 2013: Climate Change 2013: the
Physical Science Basis. Contribution of Working Group I to the Fifth
Assessment Report of the Intergovernmental Panel on Climate. Cambridge:
Cambridge University Press, 2013.
Riahi K, Krey V, Rao S, et al. RCP-8.5: exploring the consequence of high
emission trajectories. Climatic Change 2011; 109: 33–57.
Sherwood S, Huber M. An adaptabiity limit to climate change from heat
stress. Proc Natl Acad Sci USA 2010; 107: 9552–55.
Dunne JP, Stouffer RJ, John JG. Reductions in labour capacity from heat
stress under climate warming. Nat Climate Change 2014; 3: 563–66.
Smith KR. Planetary overload and the “Afterlife”: McMichael meets
Scheffler. In: Butler CD, Dixon J, Capon AC, eds. Healthy people, places and
planet: reflections based on Tony McMichael’s four decades of contribution
to epidemiological understanding. Canberra: ANU E-Press, 2014: chapter
34 (in press).
Porter JR, Xie L, Challinor AJ, et al. 2014: Food security and food
production systems. In: Field CB, Barros VR, Dokken DJ, et al, eds. Climate
Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and
Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment
Report of the Intergovernmental Panel on Climate Change. Cambridge:
Cambridge University Press, 2014. http://ipcc-wg2.gov/AR5/images/
uploads/WGIIAR5-Chap7_FGDall.pdf (accessed Sept 15, 2014).
McMichael C, Barnett J, McMichael A. An ill wind? Climate change,
migration and health. Environ Health Perspect 2012; 120: 646–54.
Smith KR, Woodward A, Campbell-Lendrum D, et al. 2014: Human health:
impacts, adaptation, and co-benefits. In: Field CB, Barros VR, Dokken DJ,
et al, eds. Climate Change 2014: Impacts, Adaptation, and Vulnerability.
Part A: Global and Sectoral Aspects. Contribution of Working Group II to the
Fifth Assessment Report of the Intergovernmental Panel on Climate
Change. Cambridge: Cambridge University Press, 2014. http://ipcc-wg2.
gov/AR5/images/uploads/WGIIAR5-Chap11_FGDall.pdf (accessed
Sept 15, 2014).
www.thelancet.com Vol 384 September 20, 2014
�Comment
9
Edenhofer O, Pichs-Madruga R, Sokona Y, et al, eds. IPCC, 2014: Climate
Change 2014: Mitigation of Climate Change. Contribution of Working
Group III to the Fifth Assessment Report of the Intergovernmental Panel on
Climate Change. Cambridge: Cambridge University Press, 2014. http://
report.mitigation2014.org/drafts/final-draft-postplenary/ipcc_wg3_ar5_
final-draft_postplenary_full.pdf (accessed Sept 15, 2014).
10
11
O’Neill B, Liddle B, Jiang L, et al. Demographic change and carbon dioxide
emissions. Lancet 2012; 380: 157–64.
United Nations Framework Convention on Climate Change. Article 2
objective. 2014. http://unfccc.int/essential_background/convention/
background/items/1353.php (accessed Sept 7, 2014).
Midwifery is commonly misunderstood. The Series of
four papers and five Comments we publish today sets
out to correct that misunderstanding. One important
conclusion is that application of the evidence presented
in this Series could avert more than 80% of maternal
and newborn deaths,1 including stillbirths. Midwifery
therefore has a pivotal, yet widely neglected, part
to play in accelerating progress to end preventable
mortality of women and children.
A frequent view is that midwifery is about
assisting childbirth. It is, but it is also much more
than that. As defined in this Series,2 midwifery is
“skilled, knowledgeable, and compassionate care for
childbearing women, newborn infants, and families
across the continuum throughout pre-pregnancy,
pregnancy, birth, post partum, and the early weeks
of life”. Midwifery includes family planning and the
provision of reproductive health services. The services
provided by midwives are best delivered not only in
hospital settings but also in communities—midwifery
is not a vertical service offered as a narrow segment of
the health system. Midwifery services are a core part of
universal health coverage.
A re-evaluation of midwifery and midwifery
services matters because progress in reducing child
and maternal mortality is now revealing critical new
obstacles to further success. Superficially, the recent
decrease in maternal and child deaths suggests steady
gains towards the Millennium Development Goals
(MDGs). But two facts provide reasons for a more
cautious conclusion. First, the number of maternal
deaths, although falling, is doing so at rates that will
prevent most countries from achieving MDG-5 by
the end of 2015. Second, although overall under-5
mortality has decreased sharply during the past
decade, the proportion of under-5 deaths taking
place in the newborn period has increased. Indeed,
a substantial number of countries with the highest
burdens of mortality have seen their absolute numbers
www.thelancet.com Vol 384 September 20, 2014
of newborn deaths either increase or remain the same.
New approaches to defeat maternal and newborn
mortality are needed.
Although this Series is about midwives and
midwifery services, the frames of reference are the
needs of the woman and her newborn infant. The
technical evidence this Series summarises is based on
a particular set of values and a distinctive philosophy.
These values include respect, communication,
community knowledge and understanding, and
care tailored to a woman’s circumstances and needs.
The philosophy is equally important—to optimise
the normal biological, psychological, social, and
cultural processes of childbirth, reducing the use of
interventions to a minimum.
Much of the programmatic work on maternal and
child health in recent years has focused on delivering
life-saving interventions to women. Although
important, coverage of women with services is
insufficient by itself to improve health outcomes.
Attention to quality is needed with equal force.
Indeed, the Series calls for “a system-level shift”,3 from
fragmented services for women and newborn infants
to interdisciplinary and integrated skilled care and
teamwork.
The work reported in this Series is not a panacea.
Sub-Saharan Africa is identified as a region especially
vulnerable to continued difficulty.4 Here, demographic
trends point to large increases in population in
coming decades. The expansion of education for
midwives to address these population shifts will
struggle to meet the rapidly increasing demand. But
this challenge is one more reason why the hopeful
and pragmatic messages contained within this Series
are so important. As governments slowly come to an
agreement about development priorities post-2015,
it is clear that maternal and newborn health will be
essential foundations of any vision for sustainable
development between 2015 and 2030. The work
Save the Children Liberia/Jonathan Hyams
The power of midwifery
Published Online
June 23, 2014
http://dx.doi.org/10.1016/
S0140-6736(14)60855-2
See Comment pages e39, e41,
and e42
See Perspectives page 1089
See Series pages 1129 and 1146
See Online/Comments
http://dx.doi.org/10.1016/
S0140-6736(14)60857-6
See Online/Series
http://dx.doi.org/10.1016/
S0140-6736(14)60919-3, and
http://dx.doi.org/10.1016/
S0140-6736(14)60930-2
1075
�
 Kristie L Ebi
Kristie L Ebi