Received: 5 November 2019
|
Revised: 15 January 2020
|
Accepted: 18 February 2020
DOI: 10.1111/jvh.13296
S H O R T C O M M U N I C AT I O N
Prevalence and 9-year incidence of hepatitis E virus infection
among North Italian blood donors: Estimated transfusion risk
Marta Spreafico1 | Livia Raffaele1 | Irene Guarnori1 | Barbara Foglieni1 |
Alessandra Berzuini2 | Luca Valenti2,3
| Alessandro Gerosa1 | Agostino Colli4 |
Daniele Prati2
Department of Transfusion Medicine and Hematology, Alessandro Manzoni Hospital, ASST-Lecco, Lecco, Italy
1
2
Department of Transfusion Medicine and Hematology, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy
3
Department of Pathophysiology and Transplantation, Università degli Studi di Milano, Milan, Italy
4
Department of Internal Medicine, Alessandro Manzoni Hospital, ASST-Lecco, Lecco, Italy
Correspondence: Daniele Prati, Department of Transfusion Medicine and Hematology, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Via
Francesco Sforza, 35 20122 Milano, Italy.
Email: daniele.prati@policlinico.mi.it
Funding information
This study was partially supported by a grant from the European Union (the Blood and Organ Transmissible Infectious Agents (BOTIA) project, No. SP23CT-2006-006487), and a contribution from Confartigianato imprese-Giovani Imprenditori, Lecco.
Keywords: hepatitis E virus, incidence, prevalence, transfusion transmission
1 | I NTRO D U C TI O N
pressure is not stable over time. This implies that NAT yields determined in the relatively short time frame of a prevalence study
Hepatitis E virus (HEV) is mainly spread in humans by contaminated
may not be entirely representative of the risk of transfusion-related
food and water, but it is increasingly being recognized as a threat to
transmission, and serological incidence data may be more useful.
blood transfusion safety because of its documented transmission by
means of viremic blood components.1,2
Taking advantage of a longitudinal biorepository financed by the
European Union,5 we calculated the prevalence and incidence of
The risk of transfusion-related infection is generally estimated
HEV infection over the last ten years in donors from Northern Italy
on the basis of the prevalence of HEV RNA among blood donors.
and used these data to estimate the risk of the transfusion-related
Nucleic acid testing (NAT) has detected a high rate of viremic do-
transmission of HEV infection.
nations (up to one in 600) in a number of European countries.1,2
There is some evidence of high prevalence of viremia and anti-HEV
reactivity among donors in Abruzzo (Central Italy),3 although a ret-
2 | S U B J EC T S A N D M E TH O DS
rospective analysis conducted in plasma pools by the Italian National
Blood Centre suggests that the pattern of HEV circulation might be
The study was conducted within the framework of the EU-funded
different in other Italian regions.4
Blood and Organ Transmissible Infectious Agents (BOTIA) project
However, pooling procedures can limit the analytical sensi-
(SP23-CT-2006-006487).5 The study protocol was approved by our
tivity of NAT and so donations should undergo individual test-
local Institutional Review Board and conducted in accordance with
ing. Furthermore, a number of reports indicate that the infection
Italian Authorisation No. 9/2014 of 11 December 2014 concerning
Abbreviations: CIs, confidence intervals; HEV, hepatitis E virus; ID-NAT, individual nucleic acid testing; NAT, nucleic acid testing.
This is an open access article under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in any medium,
provided the original work is properly cited.
© 2020 The Authors. Journal of Viral Hepatitis published by John Wiley & Sons Ltd
858
|
wileyonlinelibrary.com/journal/jvh
J Viral Hepat. 2020;27:858–861.
�|
SPREAFICO Et Al.
personal data protection for scientific research purposes. The do-
859
of years of follow-up and expressed as a number per 10 000 per
nors underwent biochemical and virological testing as prescribed by
year. The risk of receiving an infectious blood unit was estimated
Italian regulations.
using two methods: HEV RNA yield and serological incidence, as-
Frozen plasma samples from donations collected at the
Department of Transfusion Medicine and Hematology in Lecco in
suming a viremia duration of four weeks in the case of asymptomatic
infections.6
2015-2016 were tested for the presence of circulating HEV RNA by
means of individual NAT (ID-NAT), using the Procleix HEV assay and
Panther instruments (Grifols, Barcelona, Spain), with a 95% limit of
3 | R E S U LT S
detection of 7.9 IU/mL. Donors found to be initially ID-NAT reactive
were re-tested on a different aliquot, tested for anti-HEV IgG and
IgM (DiaPro HEV IgG and HEV IgM kits; Diagnostic BioprobesSrl)
and followed up at subsequent donations.
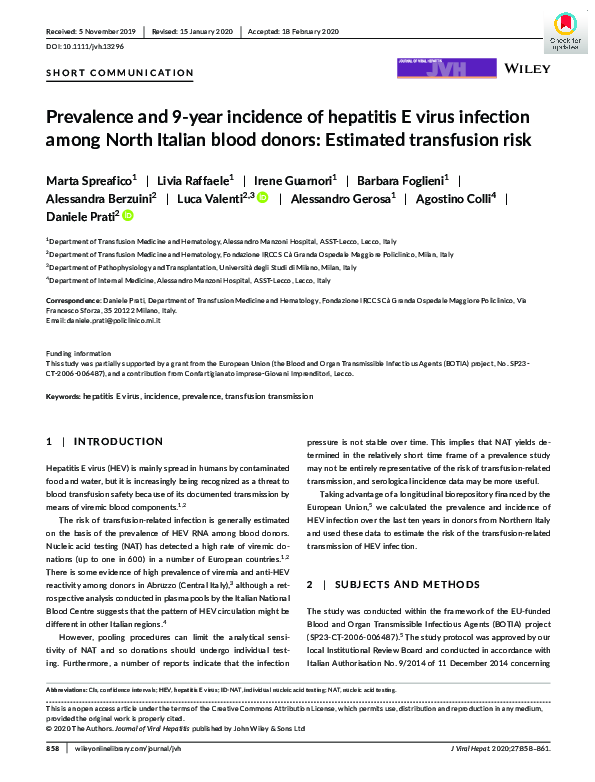
Figure 1 summarizes the study results.
A total of 9726 donor samples were collected for the HEV RNA
study: 7253 (74.5%) taken from males and 2473 (25.5%) taken from
A subset of samples was also analysed for the presence of an-
females, with a mean age of 43 years (range: 18-67).
ti-HEV IgG in order to study the prevalence of past exposure to HEV.
The ID-NAT assay showed that ten of the samples were initially
Confirmation of initially reactive samples was based on repeated
reactive, but repeated testing confirmed reactivity in only one.
testing and, when possible, on follow-up.
The donor was a 63-year-old female who had normal alanine ami-
Finally, in order to evaluate the dynamics of HEV infection over
nostransferase levels (ie 22U/L) and was fully asymptomatic at the
time, we identified a subgroup of donors who had given two serial
pre-donation examination. She subsequently seroconverted to being
samples over a relatively long follow-up: that is the first at the start
anti-HEV IgG positive. None of the nine donors whose initial reac-
of the BOTIA project in 2007-2010, and the second in 2017. These
tivity was not confirmed seroconverted during the follow-up period.
samples were tested for anti-HEV IgG, and the incidence of infec-
Thus, the prevalence of HEV RNA was 0.01% (95% CI 0.00%-0.06%).
tion was calculated as the number of seroconversions by the total
In addition, 767 samples (76.7% males, 23.3% females, mean
number of initially negative cases, multiplied by the median number
age 43 years) were analysed in order to determine the prevalence
VIREMIA STUDY
9726 anonymized
blood donations
(July2015-July2016)
Procleix ID HEV Assay (Grifols)
If positive
SEROPREVALENCE STUDY
Prevalence of anti-HEV IgG
767 samples
6.8%
Anti-HEV IgG (DiaPro)
(95%CI 5.1% – 8.8%)
Anti-HEV
IgG & IgM
(DiaPro)
INCIDENCE STUDY
640 samples (320 pairs)
Anti-HEV IgG (DiaPro)
FOLLOW-UP
(1y)
Anti-HEV
IgG & IgM (DiaPro)
7.6 per 10 000 per year
BOTIA donor
sample repository
(2007-2010)
Prevalence of anti-HEV RNA
0.01%
(95%CI 0.00% – 0.06%)
FIGURE 1
Incidence of HEV infection
Flow chart and main results of the study
Donor
samples
(2017)
(95%CI 2.1% –27.5%)
�860
|
SPREAFICO Et Al.
of anti-HEV. Anti-HEV IgG reactivity was confirmed in fifty-two do-
rates recorded in previous studies is related to methodological
nors (45 males and 7 females), thus indicating an overall prevalence
differences.
of IgG of 6.8% (95% CI 5.1%-8.8%). None of them was concomitantly
As expected, the prevalence of anti-HEV increased with age,
anti-HEV IgM or HEV RNA positive. The prevalence of anti-HEV IgG
thus reflecting a cohort effect and the long-term persistence of anti-
increased across age strata, ranging from 1% (95% CI 0.0%-5.7%)
body reactivity after primary infection. The fact that the age-related
in donors of 18-30 years to 11.1% (95% CI,7%-16.5%) in those of
increases in prevalence were relatively uniform (data not shown)
50 years or older.
suggests that no major outbreak has occurred since the 1950s. Our
Finally, a subset of 320 donors contributed 640 paired samples
prospective repository of biological samples allowed us to calcu-
collected between 2007 and 2017 (mean interval between sampling:
late the incidence of HEV infection over a ten year period, which
9 years, range 8-10). Thirty-one donors (9.7%; 95% CI: 6.7-13.5%)
proved to be 7.6/10 000 per year and is substantially lower than the
were anti-HEV IgG positive at baseline, and all of them were still
calculated incidence in other European countries such as Germany
reactive when the second sample was collected. Two of the 289 do-
(35/10 000 per year).8 Furthermore, these data allowed us to esti-
nors who were initially anti-HEV-IgG negative had seroconverted
mate the local transfusion-related risk of infection using a method
by the time of the follow-up sample: they were both males and, in
based on the assumption that the viremic phase (and therefore, the
2017, were, respectively, 48 and 49 years old. The incidence was 7.6
infectiousness of the blood products collected during active infec-
(95% CI 2.1-27.5) per 10 000 per year. The estimated risk of transfu-
tion) lasted four weeks in each seroconverting blood donor.6 On the
sion-related infection based on HEV RNA yields was 1/10000 blood
basis of this calculation, approximately one out of 16 000 donors
donations (the upper limit of the 95% CI was 1/1,666); the estimate
should be positive at any given time, a figure that is in line with the
based on the incidence data was 1/16666 blood donations (95% CI
prevalence of HEV RNA found in this study and confirms that in-
1/4350-1/57000).
fection pressure remained quite stable in northern Italy during the
considered ten years.
The limitations of this study include the fact that we could not
4 | D I S CU S S I O N
look back on HEV transmission because all of the samples were
coded and blinded to investigators, according to current regula-
Our study combined HEV viremia and serological data in order to
tions. Secondly, the findings cannot be extended to the Italian
estimate transfusion risk over a ten year period. Using high sensi-
population as a whole because of the geographical heterogene-
tive individual testing, we found that only one of the ten initially
ity of the circulation of HEV. However, our study population was
HEV RNA reactive samples in our series was found to be truly
representative of the local community of blood donors as it in-
viremic, accounting for one out of almost ten thousand blood do-
cluded donors living in urban, suburban, rural and mountain areas.
nations. In addition, the overall seroprevalence of anti-HEV IgG
Lombardy is the most highly populated region in Italy, and its
was 6.8%. These data indicate that the frequency of current and
transfusion system provides 24% of the total Italian blood sup-
past HEV infections among blood donors in northern Italy is one
ply. Although the circulation of HEV is minimal in comparison with
of the lowest so far reported in Europe. According to recent re-
other European countries, our data indicate that some tens to
views, the prevalence of HEV RNA positivity ranges from 1/762 in
hundreds of HEV-infected blood components a year may be trans-
the Netherlands to 1/8416 in Austria and that of anti-HEV ranges
fused into blood recipients. Some of them, such as immunocom-
from 12% in England to 53% in south-western France. 2 Our find-
promised patients, are susceptible to the development of acute or
ings are also very different from those observed in Abruzzo, a
chronic liver failure, or a chronic infection that may rapidly prog-
region in central Italy. According to Lucarelli et al , almost half
ress to liver cirrhosis and death.1,2
3
of the subjects donating blood in L’Aquila during the first months
The findings of this study may be useful for the regional and na-
of 2014 showed serological signs of previous HEV exposure, and
tional blood authorities responsible for making policy decisions given
one out of 166 had detectable viremia. The highly endemic nature
that recent European guidelines1 recommend that HEV screening
of the infection in this area has been attributed to local dietary
policies should be based on local risk assessment studies. Whether
habits favouring zoonotic transmissions, but another possibility is
or not to introduce HEV NAT screening therefore requires careful
contaminated water, as the circulation of some faecal pathogens
consideration: donor screening may very effectively minimize iatro-
increased in the area of L’Aquila for several years after the cata-
genic HEV infection, but it is very costly and can be expected to have
strophic earthquake in 2006.
a relatively minor impact on the number of HEV infections in the
7
Given that nine of the ten initially NAT-reactive samples were
not confirmed by further testing or at serological follow-up, it seems
population as a whole because the vast majority of new infections
seems to be due to dietary exposure.1,2
that a single determination of HEV RNA has little positive predictive
value. The impact of false-positive results might be more evident
C O N FL I C T O F I N T E R E S T
when testing samples at low risk of infection, like blood donors. It
Grifols Italia S.p.A (Milan, Italy) and Diagnostic BioprobesSrl, (Milan,
is therefore possible that some of the variability in the prevalence
Italy) provided the kits for serological and molecular analyses.
�|
SPREAFICO Et Al.
ORCID
Luca Valenti
https://orcid.org/0000-0001-8909-0345
Daniele Prati
https://orcid.org/0000-0002-2281-7498
REFERENCES
1. European Association for the Study of the Liver. EASL Clinical
Practice Guidelines on hepatitis E virus infection. J Hepatol.
2018;68:1256-1271.
2. Ankcorn MJ, Tedder RS. Hepatitis E: the current state of play. Transfus
Med. 2017;27:84-95.
3. Lucarelli C, Spada E, Taliani G, et al. High prevalence of anti-hepatitis E virus antibodies among blood donors in central Italy, February
to March 2014. Euro Surveillance. 2016;21(30):pii:30299. https://doi.
org/10.2807/1560-7917.ES.2016.21.30.30299
4. Spada E, Pupella S, Pisani G, et al. A nationwide retrospective study
on prevalence of hepatitis E virus infection in Italian blood donors.
Blood Transfus. 2018;16:413-421.
5. Spreafico M, Berzuini A, Foglieni B, et al. Poor efficacy of nucleic
acid testing in identifying occult HBV infection and consequences for
safety of blood supply in Italy. J Hepatol. 2015;63:1068-1076.
861
6. Vollmer T, Diekmann J, Eberhardt M, Knabbe C, Dreier J. Hepatitis E
in blood donors: investigation of the natural course of asymptomatic
infection, Germany, 2011. Euro Surveillance. 2016;21(35): pii:30332.
https://doi.org/10.2807/1560-7917.ES.2016.21.35.30332
7. Nigro G, Bottone G, Maiorani D, Trombatore F, Falasca S, Bruno G.
Pediatric epidemic of salmonella entericaserovartyphimurium in the
area of L'Aquila, Italy, four years after a catastrophic earthquake. Int J
Environ Res Public Health. 2016;13(5):475.
8. Juhl D, Baylis SA, Blümel J, Görg S, Hennig H. Seroprevalence and
incidence of hepatitis E virus infection in German blood donors.
Transfusion. 2014;54:49-56.
How to cite this article: Spreafico M, Raffaele L, Guarnori I, et
al. Prevalence and 9-year incidence of hepatitis E virus
infection among North Italian blood donors: Estimated
transfusion risk. J Viral Hepat. 2020;27:858–861. https://doi.
org/10.1111/jvh.13296
�
 Luca Valenti
Luca Valenti