WO2025094107A1 - Methods for treating high-risk smoldering multiple myeloma - Google Patents
Methods for treating high-risk smoldering multiple myeloma Download PDFInfo
- Publication number
- WO2025094107A1 WO2025094107A1 PCT/IB2024/060769 IB2024060769W WO2025094107A1 WO 2025094107 A1 WO2025094107 A1 WO 2025094107A1 IB 2024060769 W IB2024060769 W IB 2024060769W WO 2025094107 A1 WO2025094107 A1 WO 2025094107A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- treatment
- doses
- bispecific antibody
- dose
- bcmaxcd3
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Pending
Links
Classifications
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2878—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the NGF-receptor/TNF-receptor superfamily, e.g. CD27, CD30, CD40, CD95
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2809—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against the T-cell receptor (TcR)-CD3 complex
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/30—Immunoglobulins specific features characterized by aspects of specificity or valency
- C07K2317/31—Immunoglobulins specific features characterized by aspects of specificity or valency multispecific
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/50—Immunoglobulins specific features characterized by immunoglobulin fragments
- C07K2317/52—Constant or Fc region; Isotype
Definitions
- Smoldering multiple myeloma is a precursor disease state that precedes the development of symptomatic multiple myeloma, which is a cancer of the plasma cells.
- Patients with SMM usually do not have symptoms but are at risk for progressing to active multiple myeloma (MM).
- Treatment options for multiple myeloma have improved overtime; however, despite recent therapeutic achievements, multiple myeloma remains an incurable malignancy with significant morbidity and mortality.
- There are currently no approved therapies for SMM and there remains a need for safe and effective treatment options, in particular for patients with high-risk smoldering multiple myeloma (HR-SMM), who are at high risk of developing active multiple myeloma.
- HR-SMM high-risk smoldering multiple myeloma
- a method of treating high-risk smoldering multiple myeloma comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody (e.g., teclistamab).
- a BCMAxCD3 bispecific antibody e.g., teclistamab
- the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
- the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 11, and the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
- the BCMAxCD3 bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype.
- the BCMAxCD3 bispecific antibody is an IgG4 isotype.
- the BCMAxCD3 bispecific antibody comprises one or more substitutions in its Fc region.
- the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region (according to EU index numbering).
- the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region (according to EU index numbering).
- the Fc region of the BCMA binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively (according to EU index numbering).
- the Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions (according to EU index numbering).
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
- HC1 first heavy chain having at least 90% identity to the amino acid sequence of SEQ ID NO: 12
- LC1 having at least 90% identity to the amino acid sequence of SEQ ID NO: 13
- HC2 having at least 90% identity to the amino acid sequence of SEQ ID NO: 22
- LC2 second light chain having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody is teclistamab.
- the subject has not received prior SMM directed therapy.
- the BCMAxCD3 bispecific antibody is administered as a monotherapy (i.e., without another concurrent SMM directed therapy).
- the method comprises subcutaneously administering each dose of the BCMAxCD3 bispecific antibody.
- the method comprises treating the subject according to a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles.
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg (e.g., on Day 1), a second step-up dose of 0.3 mg/kg (e.g., on Day 3), and then weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g.,
- the regimen comprises: in Cycle
- the method achieves a clinical response in the subject that is a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as defined by IMWG (2016) response criteria.
- PR partial response
- VGPR very good partial response
- CR complete response
- sCR stringent complete response
- the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 70% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR- SMM of 75% or higher. In certain embodiments, the method comprises the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 80% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 85% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 90% or higher.
- the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 95% or higher. In certain embodiments, the method achieves an overall response rate (ORR) of 100% in a population of subjects with HR-SMM.
- the method achieves a CR in at least 25% of a population of subjects with HR-SMM. In certain embodiments, the method achieves a CR in at least 30% of a population of subjects with HR-SMM. In certain embodiments, the method achieves a CR in at least 35% of a population of subjects with HR-SMM. In certain embodiments, the method achieves a CR in at least 40% of a population of subjects with HR-SMM.
- the method achieves MRD-negative disease in the subject.
- the subject after the subject has received at least four 28-day cycles of treatment with the BCMAxCD3 bispecific antibody, the subject’s HR-SMM does not progress.
- administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twenty-four (24) 28-day treatment cycles prevents the subject from developing multiple myeloma.
- administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twelve (12) 28-day treatment cycles prevents the subject from developing multiple myeloma.
- the method cures the HR-SMM and prevents the subject from developing MM.
- the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM that is greater than an ORR achieved in a reference population of subjects with HR-SMM, said reference population having been administered lenalidomide and dexamethasone but not the BCMAxCD3 bispecific antibody.
- ORR overall response rate
- the method achieves a percentage of complete responses (CRs) in a population of subjects with HR-SMM that is greater than a percentage of CRs achieved in a reference population of subjects with HR-SMM, said reference population having been administered lenalidomide and dexamethasone but not the BCMAxCD3 bispecific antibody.
- “About’’ when used in reference to numerical ranges, cutoffs, or specific values means within an acceptable error range for the particular value as determined by one of ordinary skill in the art, which will depend in part on how the value is measured or determined, i.e., the limitations of the measurement system. Unless explicitly stated otherwise within the Examples or elsewhere in the Specification in the context of an assay, result or embodiment, “about” means within one standard deviation per the practice in the art, or a range of up to 5%, whichever is larger.
- Antibodies is meant in a broad sense and includes immunoglobulin molecules including monoclonal antibodies including murine, human, humanized and chimeric monoclonal antibodies, antigen binding fragments, multispecific antibodies, such as bispecific, trispecific, tetraspecific etc., dimeric, tetrameric or multimeric antibodies, single chain antibodies, domain antibodies and any other modified configuration of the immunoglobulin molecule that comprises an antigen binding site of the required specificity.
- “Full length antibodies” are comprised of two heavy chains (HC) and two light chains (LC) inter-connected by disulfide bonds as well as multimers thereof (e.g. IgM).
- Each heavy chain is comprised of a heavy chain variable region (VH) and a heavy chain constant region (comprised of domains CHI, hinge, CH2 and CH3).
- Each light chain is comprised of a light chain variable region (VL) and a light chain constant region (CL).
- the VH and the VL regions can be further subdivided into regions of hypervariability, termed complementarity determining regions (CDR), interspersed with framework regions (FR).
- CDR complementarity determining regions
- FR framework regions
- Each VH and VL is composed of three CDRs and four FR segments, arranged from amino-to-carboxy-terminus in the following order: FR1, CDR1, FR2, CDR2, FR3, CDR3 and FR4.
- Immunoglobulins can be assigned to five major classes, IgA, IgD, IgE, IgG and IgM, depending on the heavy chain constant domain amino acid sequence.
- IgA and IgG are further sub-classified as the isotypes IgAl, IgA2, IgGl, IgG2, IgG3 and IgG4.
- Antibody light chains of any vertebrate species can be assigned to one of two clearly distinct types, namely kappa (K) and lambda (X), based on the amino acid sequences of their constant domains.
- K kappa
- X lambda
- Antigen binding fragments can be synthetic, enzymatically obtainable or genetically engineered polypeptides and include the VH, the VL, the VH and the VL, Fab, F(ab')2, Fd and Fv fragments, domain antibodies (dAb) consisting of one VH domain or one VL domain, shark variable IgNAR domains, camelized VH domains, minimal recognition units consisting of the amino acid residues that mimic the CDRs of an antibody, such as FR3- CDR3-FR4 portions, the HCDR1, the HCDR2 and/or the HCDR3 and the LCDR1, the LCDR2 and/or the LCDR3.
- dAb domain antibodies
- VH and VL domains can be linked together via a synthetic linker to form various types of single chain antibody designs where the VH/VL domains can pair intramolecularly, or intermolecularly in those cases when the VH and VL domains are expressed by separate single chain antibody constructs, to form a monovalent antigen binding site, such as single chain Fv (scFv) or diabody; described for example in Int. Patent Publ. Nos. W01998/44001, WO1988/01649, WO1994/13804 and WO 1992/01047.
- scFv single chain Fv
- BCMA refers to human B-cell maturation antigen, also known as CD269 or TNFRSF17 (UniProt Q02223).
- the extracellular domain of BCMA encompasses residues 1-54 of Q02223.
- Human BCMA comprises the amino acid sequence of SEQ ID NO: 1
- Bispecific antibody refers to an antibody that specifically binds two distinct antigens.
- the bispecific antibody can have cross-reactivity to other related antigens, for example to the same antigen from other species (homologs), such as human or monkey, for example Maccicci cynomolgus (cynomolgus, cyno) or Pan troglodytes, or can bind an epitope that is shared between two or more distinct antigens.
- BCMAxCD3 bispecific antibody refers to a bispecific antibody that specifically binds BCMA and CD3.
- Cancer refers to a broad group of various diseases characterized by the uncontrolled growth of abnormal cells in the body. Unregulated cell division and growth results in the formation of malignant tumors that invade neighboring tissues and can also metastasize to distant parts of the body through the lymphatic system or bloodstream.
- a “cancer” or “cancer tissue” can include a tumor.
- CD3 refers to a human antigen which is expressed on T cells as part of the multimolecular T cell receptor (TCR) complex and which consists of a homodimer or heterodimer formed from the association of two or four receptor chains: CD3 epsilon, CD3 delta, CD3 zeta and CD3 gamma.
- Human CD3 epsilon comprises the amino acid sequence of SEQ ID NO: 2.
- SEQ ID NO: 3 shows the extracellular domain of CD3 epsilon.
- CH3 region or “CH3 domain” refers to the CH3 region of an immunoglobulin.
- the CH3 region of human IgGl antibody corresponds to amino acid residues 341-446.
- the CH3 region can also be any of the other antibody isotypes as described herein.
- CDR complementarity determining regions
- CDR CDR
- HCDR1 CDR1
- HCDR2 CDR3
- LCDR1 CDR2
- LCDR3 CDR3
- Fc gamma receptor refers to well-known FcyRI, FcyRIIa, FcyRIIb or FcyRIII. Activating FcyR includes FcyRI, FcyRIIa and FcyRIII.
- Human antibody refers to an antibody that is optimized to have minimal immune response when administered to a human subject. Variable regions of human antibody are derived from human immunoglobulin sequences. If human antibody contains a constant region or a portion of the constant region, the constant region is also derived from human immunoglobulin sequences. Human antibody comprises heavy and light chain variable regions that are “derived from” sequences of human origin if the variable regions of the human antibody are obtained from a system that uses human germline immunoglobulin or rearranged immunoglobulin genes. Such exemplary systems are human immunoglobulin gene libraries displayed on phage, and transgenic non-human animals such as mice or rats carrying human immunoglobulin loci.
- Human antibody typically contains amino acid differences when compared to the immunoglobulins expressed in humans due to differences between the systems used to obtain the human antibody and human immunoglobulin loci, introduction of somatic mutations or intentional introduction of substitutions into the frameworks or CDRs, or both.
- “human antibody” is at least about 80%, 81%, 82%, 83%, 84%, 85%, 86%, 87%, 88%, 89%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% or 99% identical in amino acid sequence to an amino acid sequence encoded by human germline immunoglobulin or rearranged immunoglobulin genes.
- human antibody can contain consensus framework sequences derived from human framework sequence analyses, for example as described in Knappik et al., (2000) J Mol Biol 296:57-86, or synthetic HCDR3 incorporated into human immunoglobulin gene libraries displayed on phage, for example as described in Shi et al., (2010) J Mol Biol 397:385-96, and in Int. Patent Publ. No. W02009/085462.
- Antibodies in which at least one CDR is derived from a non-human species are not included in the definition of “human antibody”.
- Humanized antibody refers to an antibody in which at least one CDR is derived from non-human species and at least one framework is derived from human immunoglobulin sequences. Humanized antibody can include substitutions in the frameworks so that the frameworks can not be exact copies of expressed human immunoglobulin or human immunoglobulin germline gene sequences.
- Identity refers to a relationship between the sequences of two or more polypeptide molecules or two or more nucleic acid molecules, as determined by aligning and comparing the sequences. “Percent (%) sequence identity” with respect to a reference polypeptide sequence is defined as the percentage of amino acid residues in a candidate sequence that are identical with the amino acid residues in the reference polypeptide sequence, after aligning the sequences and introducing gaps, if necessary, to achieve the maximum percent sequence identity, and not considering any conservative substitutions as part of the sequence identity.
- Alignment for purposes of determining percent amino acid sequence identity can be achieved in various ways that are within the skill in the art, for instance, using publicly available computer software such as BLAST, BLAST-2, ALIGN, or MEGALIGN (DNAStar, Inc.) software. Those skilled in the art can determine appropriate parameters for aligning sequences, including any algorithms needed to achieve maximal alignment over the full length of the sequences being compared.
- isolated refers to a homogenous population of molecules (such as synthetic polynucleotides or a protein such as an antibody) which have been substantially separated and/or purified away from other components of the system the molecules are produced in, such as a recombinant cell, as well as a protein that has been subjected to at least one purification or isolation step.
- molecules such as synthetic polynucleotides or a protein such as an antibody
- isolated antibody refers to an antibody that is substantially free of other cellular material and/or chemicals and encompasses antibodies that are isolated to a higher purity, such as to 80%, 81%, 82%, 83%, 84%, 85%, 86%, 87%, 88%, 89%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 99% or 100% purity.
- “Monoclonal antibody” refers to an antibody obtained from a substantially homogenous population of antibody molecules, i.e., the individual antibodies comprising the population are identical except for possible well-known alterations such as removal of C-terminal lysine from the antibody heavy chain or post-translational modifications such as amino acid isomerization or deamidation, methionine oxidation or asparagine or glutamine deamidation.
- Monoclonal antibodies typically bind one antigenic epitope.
- a bispecific monoclonal antibody binds two distinct antigenic epitopes.
- Monoclonal antibodies can have heterogeneous glycosylation within the antibody population.
- Monoclonal antibody can be monospecific or multispecific such as bispecific, monovalent, bivalent or multivalent.
- “Mutation” refers to an engineered or naturally occurring alteration in a polypeptide or polynucleotide sequence when compared to a reference sequence.
- the alteration can be a substitution, insertion or deletion of one or more amino acids or polynucleotides.
- Negative minimal residual disease status or “negative MRD status” or “MRD negative” refers to the PerMillionCount (i.e., a point estimate of malignant myeloma cells per million nucleated cells) in a patients on-study bone marrow sample relative to their reference bone marrow sample (i.e., Teclistamab treatment naive bone marrow sample). Based on this PerMillionCount, each sample is determined to be positive or negative. Samples are positive if the PerMillionCount is greater than or equal to the limit of sensitivity, otherwise they are negative. Negative minimal residual disease status can be determined at a sensitivity of 0.01% (IO -4 ), 0.001% (10 -5 ) or 0.0001% (10‘ 6 ). Negative minimal residual disease status can be determined using next generation sequencing (NGS).
- NGS next generation sequencing
- “Pharmaceutical composition” refers to composition that comprises an active ingredient and a pharmaceutically acceptable carrier.
- “Pharmaceutically acceptable carrier” or “excipient” refers to an ingredient in a pharmaceutical composition, other than the active ingredient, which is nontoxic to a subject.
- “Recombinant” refers to DNA, antibodies and other proteins that are prepared, expressed, created or isolated by recombinant means when segments from different sources are joined to produce recombinant DNA, antibodies or proteins.
- Refractory multiple myeloma refers to disease that is non-responsive to therapy or stops responding to therapy.
- Step-up dose refers to a dose of an active agent that is administered to a subject prior to a treatment dose.
- a step-up dose is lower than the treatment dose.
- a “priming” dose strategy may include one or more lower step-up dose(s) followed by the higher treatment doses.
- a “step-up phase” refers to an initial phase of a therapeutically effective regimen in which at least one step-up dose of a therapeutic is administered to the subject.
- a step-up phase may also include one or more treatment doses, z.e., a step- up phase may include one or more step-up doses followed by one or more treatment doses; for example, a step-up phase may include two step-up doses followed by two treatment doses.
- the step-up phase is 28 days, z.e., the step- up phase is a 28-day cycle of a therapeutically effective regimen.
- Subject refers to a human subject. Except when noted, the terms “patient” or “subject” are used interchangeably.
- T cell redirecting therapeutic refers to a molecule containing two or more binding regions, wherein one of the binding regions specifically binds a cell surface antigen on a target cell or tissue and wherein a second binding region of the molecule specifically binds a T cell antigen.
- cell surface antigen include a tumor associated antigen, such as BCMA.
- T cell antigen include, e.g., CD3. This dual/multi-target binding ability recruits T cells to the target cell or tissue leading to the eradication of the target cell or tissue.
- “Therapeutically effective amount” refers to an amount effective, at doses and for periods of time necessary, to achieve a desired therapeutic result.
- a therapeutically effective amount can vary depending on factors such as the disease state, age, sex, and weight of the individual, and the ability of a therapeutic or a combination of therapeutics to elicit a desired response in the individual. Exemplary indicators of an effective therapeutic or combination of therapeutics that include, for example, improved well-being of the patient.
- Treatment refers to both therapeutic treatment and prophylactic or preventative measures, wherein the object is to prevent or slow down (lessen) an undesired physiological change or disorder.
- Beneficial or desired clinical results include alleviation of symptoms, diminishment of extent of disease, stabilized (i.e., not worsening) state of disease, delay or slowing of disease progression, amelioration or palliation of the disease state, and remission (whether partial or total), whether detectable or undetectable.
- Treatment can also mean prolonging survival as compared to expected survival if a subject was not receiving treatment.
- Those in need of treatment include those already with the condition or disorder as well as those prone to have the condition or disorder or those in which the condition or disorder is to be prevented.
- Treatment dose refers to a dose of the active agent that is administered to a subject to treat a disease.
- a treatment dose may be administered at a regular dosing interval on a repetitive basis (e.g., weekly, biweekly, monthly).
- a treatment dose may be preceded by one or more step-up doses.
- a patient that is “triple-class exposed” refers to a multiple myeloma patient that has previously been treated with (at a minimum) a proteasome inhibitor, an immunomodulatory agent and an anti-CD38 monoclonal antibody.
- Tumor cell or a “cancer cell” refers to a cancerous, pre-cancerous or transformed cell, either in vivo, ex vivo, or in tissue culture, that has spontaneous or induced phenotypic changes. These changes do not necessarily involve the uptake of new genetic material. Although transformation can arise from infection with a transforming virus and incorporation of new genomic nucleic acid, uptake of exogenous nucleic acid or it can also arise spontaneously or following exposure to a carcinogen, thereby mutating an endogenous gene.
- Transformation/cancer is exemplified by morphological changes, immortalization of cells, aberrant growth control, foci formation, proliferation, malignancy, modulation of tumor specific marker levels, invasiveness, tumor growth in suitable animal hosts such as nude mice, and the like, in vitro, in vivo, and ex vivo.
- the goal of therapy in high-risk SMM should be to deliver as highly effective therapy as possible to ultimately achieve cure or significant delay in progression-free survival (PFS) without compromising safety.
- PFS progression-free survival
- the present inventors have developed novel methods for treating high-risk SMM using BCMAxCD3 bispecific antibodies, which provide significant efficacy compared to patients with relapsed/refractory multiple myeloma that receive the same therapy.
- Teclistamab (marketed as TECVAYLI®) is the first BCMA-directed bispecific antibody approved for the treatment of patients with relapsed or refractory multiple myeloma.
- Teclistamab is a bispecific B-cell maturation antigen (BCMA)- directed CD3 T-cell engager indicated for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least three or four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent and an anti- CD38 monoclonal antibody.
- BCMA bispecific B-cell maturation antigen
- teclistamab The efficacy of teclistamab is continuing to be evaluated in patients with relapsed or refractory multiple myeloma in a multi-center clinical study (MajesTEC-1, NCT03145181 [Phase 1] and NCT04557098 [Phase 2]).
- the study has included patients who previously received at least three prior therapies, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody.
- teclistamab demonstrated rapid, deep and durable responses, with an overall response rate (ORR) of 63% and median progression-free survival (mPFS) of 11.3 months.
- AEs hematologic adverse events
- neutropenia 64.2 percent
- anemia 37 percent
- lymphopenia 32.7 percent
- thrombocytopenia 21.2 percent
- Infections occurred in 76.4 percent of patients (44.8 percent grade 3/4).
- CRS cytokine release syndrome
- any suitable BCMAxCD3 bispecific antibody known to those skilled in the art in view of the present disclosure can be used.
- Various bispecific antibody formats include formats described herein and recombinant IgG-like dual targeting molecules, wherein the two sides of the molecule each contain the Fab fragment or part of the Fab fragment of at least two different antibodies; IgG fusion molecules, wherein full length IgG antibodies are fused to an extra Fab fragment or parts of Fab fragment; Fc fusion molecules, wherein single chain Fv molecules or stabilized diabodies are fused to heavy-chain constant-domains, Fc- regions or parts thereof; Fab fusion molecules, wherein different Fab-fragments are fused together; ScFv- and diabody-based and heavy chain antibodies (e.g., domain antibodies, nanobodies) wherein different single chain Fv molecules or different diabodies or different heavy-chain antibodies (e.g.
- bispecific formats include dual targeting molecules include Dual Targeting (DT)-Ig (GSK/Domantis), Two-in-one Antibody (Genentech) and mAb2 (F- Star), Dual Variable Domain (DVD)-Ig (Abbott), DuoBody (Genmab), Ts2Ab (Medlmmune/AZ) and BsAb (Zymogenetics), HERCULES (Biogen personal) and TvAb (Roche), ScFv/Fc Fusions (Academic Institution), SCORPION (Emergent BioSolutions/Trubion, Zymogenetics/BMS) and Dual Affinity Retargeting Technology (Fc-DART) (MacroGenics), F(ab)2 (Medarex/AMGEN), Dual-Action or Bis-Fab (Genentech), Dock-and-Lock (DNL) (Immun
- the BCMAxCD3 bispecific antibody comprises any one of the BCMA binding domains described in W02017/031104, the entire content of which is incorporated herein by reference. In some embodiments, the BCMAxCD3 bispecific antibody comprises any one of the CD3 binding domains described in W02017/031104. In some embodiments, the BCMAxCD3 bispecific antibody comprises any one of the BCMAxCD3 bispecific antibodies described in W02017/031104. [0079] In some embodiments, the BCMAxCD3 bispecific antibody is chimeric, humanized or human.
- the bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype. In preferred embodiments, the bispecific antibody is an IgG4 isotype.
- An exemplary wild-type IgG4 comprises an amino acid sequence of SEQ ID NO: 34.
- the bispecific antibody can be of any allotype. It is expected that allotype has no influence on properties of the bispecific antibodies, such as binding or Fc-mediated effector functions. Immunogenicity of therapeutic antibodies is associated with increased risk of infusion reactions and decreased duration of therapeutic response (Baert et al., (2003) N Engl J Med 348:602-08). The extent to which therapeutic antibodies induce an immune response in the host can be determined in part by the allotype of the antibody (Stickler et al., (2011) Genes and Immunity 12:213-21). Antibody allotype is related to amino acid sequence variations at specific locations in the constant region sequences of the antibody. Table 2 shows select IgGl, IgG2 and IgG4 allotypes.
- the bispecific antibody comprises one or more Fc substitutions that reduces binding of the bispecific antibody to a Fey receptor (FcyR) and/or reduces Fc effector functions such as Clq binding, complement dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC) or phagocytosis (ADCP).
- FcyR Fey receptor
- CDC complement dependent cytotoxicity
- ADCC antibody-dependent cell-mediated cytotoxicity
- ADCP phagocytosis
- Fc positions that can be substituted to reduce binding of the Fc to the activating FcyR and subsequently to reduce effector function are substitutions L234A/L235A on IgGl, V234A/G237A/P238S/H268A/V309L/A330S/P331S on IgG2, F234A/L235A on IgG4, S228P/F234A/ L235A on IgG4, N297A on all Ig isotypes, V234A/G237A on IgG2, K214T/E233P/ L234V/L235A/G236- deleted/A327G/P331A/D365E/L358M on IgGl, H268Q/V309L/ A330S/P331S on IgG2, S267E/L328F on IgGl, L234F/L235E/D265A on IgGl, L234A
- Fc substitutions that can be used to reduce CDC are a K322A substitution.
- Well-known S228P substitution can further be made in IgG4 antibodies to enhance IgG4 stability.
- the bispecific antibody comprises one or more asymmetric substitutions in a first CH3 domain or in a second CH3 domain, or in both the first CH3 domain and the second CH3 domain.
- the one or more asymmetric substitutions is selected from the group consisting of F405L/K409R, wild-type/F405L_R409K, T366Y/F405A, T366W/F405W, F405W/Y407A, T394W/Y407T, T394S/Y407A, T366W/T394S, F405W/T394S and T366W/T366S_L368A_Y407V, L351Y_F405A_Y407V/T394W, T366I_K392M_T394W/F405A_Y407V, T366L_K392M_T394W/F405A_Y407V, L351Y_Y4O7A/T366A_K4O9F, L351Y_Y4O7A/T366V_K4O9F, L351Y_Y4O7
- the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises phenylalanine at position 405 and arginine at position 409 in a first heavy chain (HC1) and leucine at position 405 and lysine at position 409 in a second heavy chain (HC2), wherein residue numbering is according to the EU Index.
- the BCMAxCD3 bispecific antibody comprises proline at position 228, alanine at position 234 and alanine at position 235 in both the HC1 and the HC2.
- Tables 3 and 4 provide sequences of an exemplary embodiment of a BCMAxCD3 bispecific antibody, according to the Kabat numbering system.
- the BCMAxCD3 bispecific antibody is CC-93269, BI 836909, JNJ-64007957 (teclistamab), or PF-06863135.
- the BCMAxCD3 bispecific antibody is teclistamab (also referred to herein as Tec), which has the sequences described in Tables 3 and 4.
- the BCMAxCD3 bispecific antibody has an amino acid sequence with at least 80%, at least 85%, at least 90%, at least 95%, at least 98%, or at least 99% sequence identity to the amino acid sequence of teclistamab.
- BCMAxCD3 bispecific antibodies that may be used in accordance with the methods are described below.
- the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
- the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 11, and the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
- the BCMAxCD3 bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype.
- the BCMAxCD3 bispecific antibody is an IgG4 isotype.
- the BCMAxCD3 bispecific antibody comprises one or more substitutions in its Fc region.
- the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region (according to EU index numbering).
- the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region (according to EU index numbering).
- the Fc region of the BCMA binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively (according to EU index numbering).
- the Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions (according to EU index numbering).
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
- HC1 first heavy chain having at least 90% identity to the amino acid sequence of SEQ ID NO: 12
- LC1 having at least 90% identity to the amino acid sequence of SEQ ID NO: 13
- HC2 having at least 90% identity to the amino acid sequence of SEQ ID NO: 22
- LC2 second light chain having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody is teclistamab.
- the inventors have developed novel methods of treating human subjects that have been diagnosed with high-risk smoldering multiple myeloma (HR-SMM). BCMAxCD3 bispecific antibodies disclosed herein are safe and highly effective in treating HR-SMM.
- the diagnosis of smoldering (asymptomatic) multiple myeloma (SMM) is based on the demonstration of M-protein in serum (>3 gm/dL) or urine and/or the presence of 10-60% clonal bone marrow plasma cells (BMPC). Patients with SMM generally have an annual risk of progression of 10% for the first 5 years.
- SMM is thought to comprise a mixture of high-risk patients, who may benefit from early therapeutic intervention before irreversible organ damage and symptoms appear.
- These high-risk SMM patients are defined as having a 50% progression rate within 2 years.
- the rationale is that early therapeutic interception of disease progression in these high-risk individuals will prevent/delay end-organ damage with all of its morbidities.
- early intervention before clonal evolution with secondary acquisition of mutations along with immune-suppressive deregulation of the microenvironment may lead to a significant improvement in disease response, progression-free survival, and overall survival.
- a patient with high-risk smoldering multiple myeloma generally meets either the Mayo 2018 Criteria (“20-2-20” critieria) or the International Myeloma Working Group Scoring System for SMM (see, e.g., Lakshman A, et al. Risk stratification of smoldering multiple myeloma incorporating revised IMWG diagnostic criteria. Blood Cancer J 2018;8:59; and Mateos MV, et al. International Myeloma Working Group risk stratification model for smoldering multiple myeloma. Blood Cancer J 2020; 10: 102, which are incorporated by reference herein).
- a patient with high-risk smoldering multiple myeloma generally meets one of the following two diagnostic criteria (i.e., either Diagnostic Criteria #1 or Diagnostic Criteria #2 below) as shown in Table 7:
- Embodiments provide methods of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
- HR-SMM high-risk smoldering multiple myeloma
- the subject has not received prior SMM directed therapy.
- the BCMAxCD3 bispecific antibody is administered as a monotherapy (i.e., without another concurrent SMM directed therapy).
- methods of preventing or inhibiting development of HR-SMM into symptomatic multiple myeloma (MM) in a subject in need thereof comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
- methods of curing HR-SMM in a subject in need thereof comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
- methods of achieving a complete response (CR) in a subject diagnosed with HR-SMM comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
- methods of achieving an overall response rate (ORR) of 100% in a population of subjects diagnosed with HR-SMM comprising administering to each of the subjects a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
- the inventors have developed novel dosing regimens for the treatment of HR- SMM that achieve deep and durable clinical responses.
- weight-based refers to administration of a dose amount that is based on the subject’s specific body weight; for example, 3 mg/kg refers to a dose of 3 milligrams of antibody per kilogram of the subject’s body weight. Unless otherwise specified herein, when a dose is described in a unit of “mg/kg” or “pg/kg,” weight-based dosing is being employed.
- a BCMAxCD3 bispecific antibody such as teclistamab
- teclistamab is administered on a dosing schedule based on sequential 28-day cycles, for example, Cycle 1 starts on Day 1 of Cycle 1 and ends on Day 28 of Cycle 1, and then Day 1 of Cycle 2 starts the day after Day 28 of Cycle 1 and ends on Day 28 of Cycle 2, and then Day 1 of Cycle 3 starts the day after Day 28 of Cycle 2 and ends on Day 28 of Cycle 3, and so on.
- Cycle 1 starts on Day 1 of Cycle 1 and ends on Day 28 of Cycle 1
- Day 1 of Cycle 2 starts the day after Day 28 of Cycle 1 and ends on Day 28 of Cycle 2
- Day 1 of Cycle 3 starts the day after Day 28 of Cycle 2 and ends on Day 28 of Cycle 3 and so on.
- Cycles 3-6 (Cycles 3, 4, 5 and 6).
- a cycle number with a “+” symbol refers to that cycle and all subsequent cycles, e.g., “C3+” refers to from Cycle 3 and all subsequent cycles (i.e., C3, C4, C5, C6, C7, and so on).
- Q4W means once every four weeks
- Q2W also referred to as “bi-weekly” or “biweekly”
- QW also referred to as “weekly”
- Q4W is sometimes referred to herein as “monthly” but technically refers to once every 4 weeks or once every 28 days (e.g., in 28-day cycles, a first treatment dose occurs on Day 1 of Cycle 1, a second treatment dose occurs on Day 1 of Cycle 2, etc.).
- Administration of a treatment dose once weekly is also referred to herein as a weekly dosing schedule; for example, a 28-day treatment cycle may have a weekly dosing schedule that comprises four doses one week apart from each other (e.g., on Days 1, 8, 15 and 22), or three doses one week apart from each other (e.g., on Days 8, 15 and 22), or two doses one week apart from each other (e.g., on Days 8 and 15).
- Administration of a treatment dose once every two weeks (Q2W) is also referred to herein as a bi-weekly dosing schedule.
- Administration of a treatment dose once every four weeks (Q4W) is also referred to herein as a monthly dosing schedule.
- Dosing regimens may be described herein in terms of the dose amount and frequency; for example, “Cl: 1.5 mg/kg QW” refers to administration of 1.5 mg/kg once per week in Cycle 1 of a therapeutically effective regimen, “C3-6: 3 mg/kg Q2W” refers to administration of 3 mg/kg once every two weeks from Cycle 3 through Cycle 6, “C7+: 3 mg/kg Q4W” refers to administration of 3 mg/kg once every four weeks starting in Cycle 7, etc.
- a “BCMAxCD3 treatment cycle” refers to each treatment cycle in a therapeutically effective regimen in which at least one treatment dose of a BCMAxCD3 bispecific antibody is administered to the subject.
- the first BCMAxCD3 treatment cycle in a therapeutically effective regimen is preceded by a step-up phase.
- CR complete response
- PR partial response
- Q2W once every 2 weeks
- Q4W once every 4 weeks
- QW once weekly
- RP2D recommended phase 2 dose
- SUD step-up dose
- methods of treating HR-SMM are effective in eliciting a clinical response in a subject as determined by International Myeloma Working Group (IMWG) 2016 response criteria.
- the methods of treatment are effective in eliciting a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as determined by IMWG 2016 response criteria.
- overall response rate refers to the percentage of patients in a population that achieve a partial response (PR) or better, i.e., a partial response, very good partial response, complete response or stringent complete response.
- PR, VGPR, CR and sCR are as defined by the IMWG (2016) criteria.
- IMWG (2016) response criteria are known in the art, and provided in Table A below. Table 8.
- Clarifications to the criteria for coding progressive disease bone marrow criteria for progressive disease are to be used only in participants without measurable disease by M-protein and by FLC levels; “25% increase” refers to M-protein, and FLC, and does not refer to bone lesions, or soft-tissue plasmacytomas and the “lowest response value” does not need to be a confirmed value.
- IMWG criteria for response to Multiple Myeloma treatment are also described, for example, in Durie et al., Kumar et al. and Rajkumar et al., which are incorporated by reference herein: Durie BG, Harousseau JL, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9): 1467-1473; Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328-346; Rajkumar SV, Harousseau JL, Durie B, et al. Consensus recommendations for the uniform reporting of clinical Trials: report of the International Myeloma Workshop Consensus Panel 1. Blood. 2011; 117(18):4691-4695.
- Embodiments provide methods of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising treating the subject according to a therapeutically effective regimen that comprises sequential BCMAxCD3 treatment cycles.
- HR-SMM multiple myeloma
- each sequential BCMAxCD3 treatment cycle is 28 days.
- the method comprises administering each dose of the BCMAxCD3 bispecific antibody subcutaneously.
- one or more step-up doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during a step-up phase (e.g., wherein the step-up phase is Cycle 1 of a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles).
- the step-up phase is 28 days.
- 1-3 step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
- two step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
- the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody.
- the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody and a second step-up dose of 0.3 mg/kg of the BCMAxCD3 bispecific antibody.
- one or more treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
- two or three treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, after the one or more step-up doses have been administered.
- each of the treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase is 0.72 mg/kg or 1.5 mg/kg or 3.0 mg/kg.
- each of the one or more treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase is administered in an amount of 1.5 mg/kg.
- the step-up phase comprises subcutaneously administering two step-up doses and three treatment doses of the BCMAxCD3 bispecific antibody.
- the step-up phase comprises subcutaneously administering two step-up doses and two treatment doses of the BCMAxCD3 bispecific antibody.
- two or three treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
- QW weekly dosing schedule
- the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg and a second treatment dose of 1 .5 mg/kg.
- the second step-up dose is administered 2-4 days after first step-up dose.
- the second step-up dose is administered 2 days after first step-up dose.
- the first treatment dose is administered 4-7 days after the second step-up dose.
- the first treatment dose is administered 5 days after the second step-up dose.
- the second treatment dose is administered 5-9 days after the first treatment dose.
- the second treatment dose is administered 7 days after the first treatment dose.
- the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg, a second treatment dose of 1.5 mg/kg and a third treatment dose of 1.5 mg/kg.
- the third treatment dose is administered 5-9 days after the second treatment dose. In certain embodiments, the third treatment dose is administered 7 days after the second treatment dose.
- the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step- up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8 and a second treatment dose of 1.5 mg/kg on Day 15.
- the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8, a second treatment dose of 1 .5 mg/kg on Day 15 and a third treatment dose of 1.5 mg/kg on Day 22.
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses.
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., six, twelve or eighteen BCMAxCD3 treatment cycles), subcutaneously administering monthly (Q4W) treatment doses.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously administering one or more
- each treatment dose of the BCMAxCD3 bispecific antibody is administered to the subject in an amount of 1.5 mg/kg or 3 mg/kg.
- each weekly (QW) treatment dose is 1.5 mg/kg
- each bi-weekly (Q2W) treatment dose is 3.0 mg/kg
- each monthly (Q4W) treatment dose is 3.0 mg/kg.
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg.
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, in Cycle 2, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg; and [0141] starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering biweekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (QW) treatment doses
- the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg (e.g., on Day 1), a second step-up dose of 0.3 mg/kg (e.g., on Day 3), and then weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g.,
- the regimen comprises: in Cycle
- Cycle 1 Dose is administered on Days 1, 3, 8, 15 and 22 of a 28-day treatment cycle. Step-up doses are given on Days 1 and 3 of Cycle 1; treatment doses are given on Days 8, 15 and 22 of Cycle 1.
- Cycles 3-6 28-day cycles: treatment is administered on Days 1 and 15.
- Treatment Cycle 1 step-up phase of an exemplary dosing regimen
- one or more pretreatment medications are administered to the subject prior to administration of a dose of the BCMAxCD3 bispecific antibody.
- one or more pretreatment medications are administered to the subject during Cycle 1 (step-up phase).
- one or more pretreatment medications are administered to the subject during Cycle 1 (step-up phase) and Cycle 2.
- one or more pretreatment medications are selected from the group consisting of dexamethasone, diphenhydramine, acetaminophen, and any combination thereof.
- pretreatment medications are administered to the subject as shown in Table 13, in which “x” signifies administration of the pretreatment medication for the indicated day.
- the methods achieve a clinical response in the subject that is a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as defined by IMWG (2016) response criteria.
- PR partial response
- VGPR very good partial response
- CR complete response
- sCR stringent complete response
- the methods achieve a CR, VGPR, or PR in the subject, as defined by IMWG (2016) response criteria.
- the methods achieve a VGPR or PR in the subject, as defined by IMWG (2016) response criteria.
- the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 70% or higher.
- the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 75% or higher.
- the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 80% or higher.
- the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 85% or higher.
- the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 90% or higher.
- the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 95% or higher.
- the methods achieve an overall response rate (ORR) of 100% in a population of subjects with HR-SMM.
- the methods achieve a CR in at least 25% of a population of subjects with HR-SMM.
- the methods achieve a CR in at least 30% of a population of subjects with HR-SMM.
- the methods achieve a CR in at least 35% of a population of subjects with HR-SMM.
- the methods achieve a CR in at least 40% of a population of subjects with HR-SMM.
- the methods achieve MRD-negative disease in the subject.
- the subject after the subject has received at least four 28 -day cycles of treatment with the BCMAxCD3 bispecific antibody, the subject’s HR-SMM does not progress.
- administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twenty-four (24) 28-day treatment cycles prevents the subject from developing multiple myeloma.
- administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twelve (12) 28-day treatment cycles prevents the subject from developing multiple myeloma.
- the method cures the HR- SMM and prevents the subject from developing MM.
- the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM that is greater than an ORR achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
- the method achieves a percentage of complete responses (CRs) in a population of subjects with HR-SMM that is greater than a percentage of CRs achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
- HR-SMM high-risk smoldering multiple myeloma
- the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
- the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 11
- the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
- BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region (according to EU index numbering).
- BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region (according to EU index numbering).
- Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions (according to EU index numbering).
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
- the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
- step-up doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during a step-up phase (e.g., wherein the step-up phase is Cycle 1 of a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles).
- step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody.
- step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody and a second step-up dose of 0.3 mg/kg of the BCMAxCD3 bispecific antibody.
- step-up phase comprises subcutaneously administering two step-up doses and two treatment doses of the BCMAxCD3 bispecific antibody.
- step-up phase comprises subcutaneously administering two step-up doses and three treatment doses of the BCMAxCD3 bispecific antibody.
- step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg and a second treatment dose of 1.5 mg/kg.
- step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8 and a second treatment dose of 1.5 mg/kg on Day 15.
- step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg, a second treatment dose of 1.5 mg/kg and a third treatment dose of 1.5 mg/kg.
- step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8, a second treatment dose of 1.5 mg/kg on Day 15 and a third treatment dose of 1.5 mg/kg on Day 22.
- any of embodiments 1-48 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- any of embodiments 1-48 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment
- any of embodiments 1-48 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., six, twelve or eighteen BCMAxCD3 treatment cycles), subcutaneously administering monthly (Q4W) treatment doses.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously
- any of embodiments 1-48 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, in Cycle 2, subcutaneously administering weekly (QW) treatment doses, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses; and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses.
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, in Cycle 2, subcutaneously administering weekly (QW) treatment doses, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses; and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles
- each treatment dose of the BCMAxCD3 bispecific antibody is administered to the subject in an amount of 1.5 mg/kg or 3 mg/kg (e.g., wherein each weekly treatment dose is 1.5 mg/kg, each biweekly treatment dose is 3.0 mg/kg, and each monthly treatment dose is 3.0 mg/kg).
- any of embodiments 1-53 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- any of embodiments 1-54 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg.
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-week
- any of embodiments 1-55 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg
- any of embodiments 1-56 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, in Cycle 2, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg; and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
- the BCMAxCD3 bispecific antibody e.g., teclistamab
- any of embodiments 1-57 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
- the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (
- any of embodiments 1-58 comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg (e.g., on Day 1), a second step-up dose of 0.3 mg/kg (e.g., on Day 3), and then weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.
- the regimen comprises:
- Anti-BCMA/anti-CD3 antibody teclistamab also called Tec
- Teclistamab comprises a BCMA binding arm BCMB69 and a CD3 binding arm CD3B219, the amino acid sequences of which are shown in Table 5 and Table 6, respectively.
- teclistamab also referred to as “TEC” or “Tec”
- HR- SMM high-risk smoldering multiple myeloma
- This study has an initial, safety run-in cohort of 6 patients treated with TEC. All patients receive 2 step-up doses of subcutaneous TEC. In the safety run-in, patients receive a dose lower than the recommended phase 2 dose (RP2D) of TEC. If no dose limiting toxicities (DLTs) are observed, the next cohort receives the RP2D of TEC.
- RP2D recommended phase 2 dose
- DLTs dose limiting toxicities
- TEC is given at a dose of 1.5 mg/kg weekly for cycles 1 and 2 followed by 3 mg/kg on days 1 and 15 for cycles 3 to 6, and monthly starting with cycle 7 for a total of 24 cycles (2 years).
- lenalidomide is given at a dose of 25 mg orally on days 1-21 and dexamethasone 40mg is given weekly during the 28-day cycle for 24 cycles. All eligible patients undergo stem cell collection after 4 cycles of therapy.
- the primary objective is complete response rate. Secondary objectives include PFS, ORR, MRD negativity rates, pharmacokinetics of TEC, and safety. Exploratory objectives include mass spectrometry quantification of M protein, molecular evolution of tumor cells, and immune biomarkers of response. Eligibility Criteria:
- BMPC Bone Marrow Plasma Cell
- BMPC Bone Marrow Plasma Cell
- FISH Fluorescence In Situ Hybridization
- Evolving pattern o Evolving M-Protein (eMP: >10% increase in Serum Mi- Protein) over a 6 month period OR; o Evolving change in hemoglobin (eHb) > 0.5 g/dl decrease over a 12 month period OR; o Progressive Involved light chain increase > 10% over a 6 month period along with a light chain ratio > 8
- Bone lesions lytic lesions or generalized osteoporosis with compression fractures
- Serum involved/uninvolved FLC ratio >100 is not considered a MDE if urinary monoclonal protein is ⁇ 200mg/24 hours.
- Symptomatic Multiple Myeloma or any evidence of CRAB criteria including presence of myeloma defining events (MDE). Any prior therapy for active Myeloma should also be excluded. Prior therapy for smoldering myeloma is not an exclusion criterion. Bisphosphonates are not excluded.
- Prior therapy with bisphosphonate is allowed.
- Prior radiation therapy to a solitary plasmacytoma is allowed but had to be at least 6 months prior to enrollment on the trial.
- Prior clinical trials or therapy for smoldering MM or MGUS are allowed per exclusion criteria described above. Serious medical or psychiatric illness likely to interfere with participation in this clinical study.
- Uncontrolled intercurrent illness including, but not limited to, ongoing or active infection, symptomatic congestive heart failure, unstable angina pectoris, cardiac arrhythmia, or psychiatric illness/social situations that would limit compliance with study requirements.
- Pregnant or breast-feeding or planning to become pregnant while enrolled in this study or within 90 days after receiving the last dose of study drug are preferred.
- HIV human immunodeficiency virus
- HBV hepatitis B virus
- HCV hepatitis C virus
- hepatitis B virus vaccine Participants who are seropositive because of hepatitis B virus vaccine are eligible. Participants who are positive for HIV 1 and 2 antibody, hepatitis B core antibody or hepatitis B surface antigen must have a negative polymerase chain reaction (PCR) result before enrollment. Those who are PCR positive will be excluded. Contraindications or life-threatening allergies, hypersensitivity, or intolerance to any study drug or its excipients (refer to the teclistamab Investigator’s Brochure and appropriate package inserts).
- PCR polymerase chain reaction
- N0M0 Localized prostate cancer
- o With a Gleason score of ⁇ 6, treated within the last 24 months, or untreated and under surveillance o With a Gleason score of 3+4 that has been treated >6 months prior to full study screening and considered to have a very low risk of recurrence, or • History of localized prostate cancer and receiving androgen deprivation therapy and considered to have a very low risk of recurrence.
- Breast cancer adequately treated lobular carcinoma in situ or ductal carcinoma in situ, or history of localized breast cancer and receiving antihormonal agents and considered to have a very low risk of recurrence.
- the ORR is 100% with 42% achieving a CR, 25% VGPR, 33% PR.
- Four patients with high-risk FISH receiving TEC have achieved a CR within 5 cycles.
- the ORR is 66% without any complete responses to date.
- the MRD negative rate at 10‘ 6 is 100%, including 2 patients with VGPR-MRD negative disease.
- Average time to MRD negativity observed among evaluable patients was 4.25 cycles. No patients have progressed on treatment. Stem cell collection was successful in all eligible patients with an average stem cell yield of 9.06 x 10 6 CD34+ cells/kg.
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Immunology (AREA)
- Organic Chemistry (AREA)
- Life Sciences & Earth Sciences (AREA)
- Medicinal Chemistry (AREA)
- General Health & Medical Sciences (AREA)
- Biophysics (AREA)
- Molecular Biology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Genetics & Genomics (AREA)
- Biochemistry (AREA)
- Veterinary Medicine (AREA)
- General Chemical & Material Sciences (AREA)
- Public Health (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Medicines Containing Antibodies Or Antigens For Use As Internal Diagnostic Agents (AREA)
- Peptides Or Proteins (AREA)
Abstract
Embodiments relate to methods of treating high-risk smoldering multiple myeloma in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
Description
METHODS FOR TREATING HIGH-RISK SMOLDERING MULTIPLE MYELOMA
CROSS-REFERENCE TO RELATED APPLICATIONS
[0001] This application claims priority to United States Provisional Application Serial Number 63/594,977, filed November 1, 2023, the entire contents of which are incorporated herein by reference in their entirety.
REFERENCE TO SEQUENCE LISTING SUBMITTED ELECTRONICALLY
[0002] This application contains a sequence listing, which is submitted electronically in XML format and is hereby incorporated by reference in its entirety. Said XML copy, created on October 3, 2024, is named “258199061802 (JBI6854WOPCT1) Sequence Listing.xml” and is 26,334 bytes in size.
FIELD
[0003] Methods of treating high-risk smoldering multiple myeloma are disclosed.
BACKGROUND
[0004] Smoldering multiple myeloma (SMM) is a precursor disease state that precedes the development of symptomatic multiple myeloma, which is a cancer of the plasma cells. Patients with SMM usually do not have symptoms but are at risk for progressing to active multiple myeloma (MM). Treatment options for multiple myeloma have improved overtime; however, despite recent therapeutic achievements, multiple myeloma remains an incurable malignancy with significant morbidity and mortality. There are currently no approved therapies for SMM, and there remains a need for safe and effective treatment options, in particular for patients with high-risk smoldering multiple myeloma (HR-SMM), who are at high risk of developing active multiple myeloma.
SUMMARY
[0005] There is provided a method of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody (e.g., teclistamab).
[0006] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
[0007] In certain embodiments, the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 11, and the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
[0008] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype.
[0009] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype.
[0010] In certain embodiments, the BCMAxCD3 bispecific antibody comprises one or more substitutions in its Fc region.
[0011] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region (according to EU index numbering).
[0012] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region (according to EU index numbering).
[0013] In certain embodiments, the Fc region of the BCMA binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively (according to EU index numbering).
[0014] In certain embodiments, the Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions (according to EU index numbering).
[0015] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain
(LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
[0016] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
[0017] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
[0018] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
[0019] In certain embodiments, the BCMAxCD3 bispecific antibody is teclistamab.
[0020] In certain embodiments, the subject has not received prior SMM directed therapy.
[0021] In certain embodiments, the BCMAxCD3 bispecific antibody is administered as a monotherapy (i.e., without another concurrent SMM directed therapy).
[0022] In certain embodiments, the method comprises subcutaneously administering each dose of the BCMAxCD3 bispecific antibody.
[0023] In certain embodiments, the method comprises treating the subject according to a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles.
[0024] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles,
wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg (e.g., on Day 1), a second step-up dose of 0.3 mg/kg (e.g., on Day 3), and then weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
[0025] In certain embodiments, the method achieves a clinical response in the subject that is a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as defined by IMWG (2016) response criteria.
[0026] In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 70% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR- SMM of 75% or higher. In certain embodiments, the method comprises the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 80% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 85% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 90% or higher. In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 95% or higher. In certain embodiments, the method achieves an overall response rate (ORR) of 100% in a population of subjects with HR-SMM.
[0027] In certain embodiments, the method achieves a CR in at least 25% of a population of subjects with HR-SMM. In certain embodiments, the method achieves a CR in at least 30% of a population of subjects with HR-SMM. In certain embodiments, the method achieves a CR in at least 35% of a population of subjects with HR-SMM. In certain embodiments, the method achieves a CR in at least 40% of a population of subjects with HR-SMM.
[0028] In certain embodiments, the method achieves MRD-negative disease in the subject.
[0029] In certain embodiments, after the subject has received at least four 28-day cycles of treatment with the BCMAxCD3 bispecific antibody, the subject’s HR-SMM does not progress.
[0030] In certain embodiments, administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twenty-four (24) 28-day treatment cycles prevents the subject from developing multiple myeloma.
[0031] In certain embodiments, administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twelve (12) 28-day treatment cycles prevents the subject from developing multiple myeloma.
[0032] In certain embodiments, the method cures the HR-SMM and prevents the subject from developing MM.
[0033] In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM that is greater than an ORR achieved in a reference population of subjects with HR-SMM, said reference population having been administered lenalidomide and dexamethasone but not the BCMAxCD3 bispecific antibody.
[0034] In certain embodiments, the method achieves a percentage of complete responses (CRs) in a population of subjects with HR-SMM that is greater than a percentage of CRs achieved in a reference population of subjects with HR-SMM, said reference population having been administered lenalidomide and dexamethasone but not the BCMAxCD3 bispecific antibody.
[0035] All methods described herein, however expressed, may be described as corresponding uses, in particular medical uses.
DETAILED DESCRIPTION
[0036] The disclosed methods can be understood more readily by reference to the following detailed description. It is to be understood that the disclosed methods are not limited to the specific methods described and/or shown herein, and that the terminology used herein is for the purpose of describing particular embodiments by way of example only and is not intended to be limiting of the claimed methods. All patents, published patent applications and publications cited herein are incorporated by reference as if set fourth fully herein.
[0037] As used herein, the singular forms “a,” “an,” and “the” include the plural.
[0038] Various terms relating to aspects of the description are used throughout the specification and claims. Such terms are to be given their ordinary meaning in the art unless otherwise indicated. Other specifically defined terms are to be construed in a manner consistent with the definitions provided herein.
[0039] “About’’ when used in reference to numerical ranges, cutoffs, or specific values means within an acceptable error range for the particular value as determined by one of ordinary skill in the art, which will depend in part on how the value is measured or determined, i.e., the limitations of the measurement system. Unless explicitly stated otherwise within the Examples or elsewhere in the Specification in the context of an assay, result or embodiment, “about” means within one standard deviation per the practice in the art, or a range of up to 5%, whichever is larger.
[0040] “Antibodies” is meant in a broad sense and includes immunoglobulin molecules including monoclonal antibodies including murine, human, humanized and chimeric monoclonal antibodies, antigen binding fragments, multispecific antibodies, such as bispecific, trispecific, tetraspecific etc., dimeric, tetrameric or multimeric antibodies, single chain antibodies, domain antibodies and any other modified configuration of the immunoglobulin molecule that comprises an antigen binding site of the required specificity. “Full length antibodies” are comprised of two heavy chains (HC) and two light chains (LC) inter-connected by disulfide bonds as well as multimers thereof (e.g. IgM). Each heavy chain is comprised of a heavy chain variable region (VH) and a heavy chain constant region (comprised of domains CHI, hinge, CH2 and CH3). Each light chain is comprised of a light chain variable region (VL) and a light chain constant region (CL). The VH and the VL regions can be further subdivided into regions of hypervariability, termed complementarity determining regions (CDR), interspersed with framework regions (FR). Each VH and VL is composed of three CDRs and four FR segments, arranged from amino-to-carboxy-terminus in the following order: FR1, CDR1, FR2, CDR2, FR3, CDR3 and FR4. Immunoglobulins can be assigned to five major classes, IgA, IgD, IgE, IgG and IgM, depending on the heavy chain constant domain amino acid sequence. IgA and IgG are further sub-classified as the isotypes IgAl, IgA2, IgGl, IgG2, IgG3 and IgG4. Antibody light chains of any vertebrate species can be assigned to one of two clearly distinct types, namely kappa (K) and lambda (X), based on the amino acid sequences of their constant domains.
[0041] “Antigen binding fragment” or “antigen binding domain” refers to a portion of an immunoglobulin molecule that binds an antigen. Antigen binding fragments can be synthetic, enzymatically obtainable or genetically engineered polypeptides and include the VH, the VL, the VH and the VL, Fab, F(ab')2, Fd and Fv fragments, domain antibodies (dAb) consisting of one VH domain or one VL domain, shark variable IgNAR domains, camelized VH domains, minimal recognition units consisting of the amino acid residues that mimic the CDRs of an antibody, such as FR3- CDR3-FR4 portions, the HCDR1, the HCDR2 and/or the HCDR3 and the LCDR1, the LCDR2 and/or the LCDR3. VH and VL domains can be linked together via a synthetic linker to form various types of single chain antibody designs where the VH/VL domains can pair intramolecularly, or intermolecularly in those cases when the VH and VL domains are expressed by separate single chain antibody constructs, to form a monovalent antigen binding site, such as single chain Fv (scFv) or diabody; described for example in Int. Patent Publ. Nos. W01998/44001, WO1988/01649, WO1994/13804 and WO 1992/01047.
[0042] BCMA refers to human B-cell maturation antigen, also known as CD269 or TNFRSF17 (UniProt Q02223). The extracellular domain of BCMA encompasses residues 1-54 of Q02223. Human BCMA comprises the amino acid sequence of SEQ ID NO: 1
SEQ ID NO: 1
MLQMAGQCSQNEYFDSLLHACIPCQLRCSSNTPPLTCQRYCNASVTNSV KGTNAILWTCLGLSLIISLAVFVLMFLLRKINSEPLKDEFKNTGSGLLGMA NIDLEKSRTGDEIILPRGLEYTVEECTCEDCIKSKPKVDSDHCFPLPAMEE GATILVTTKTNDYCKSLPAALSATEIEKSISAR
[0043] “Bispecific antibody” as used herein refers to an antibody that specifically binds two distinct antigens. The bispecific antibody can have cross-reactivity to other related antigens, for example to the same antigen from other species (homologs), such as human or monkey, for example Maccicci cynomolgus (cynomolgus, cyno) or Pan troglodytes, or can bind an epitope that is shared between two or more distinct antigens. [0044] “BCMAxCD3 bispecific antibody” refers to a bispecific antibody that specifically binds BCMA and CD3.
[0045] “Cancer” refers to a broad group of various diseases characterized by the uncontrolled growth of abnormal cells in the body. Unregulated cell division and growth
results in the formation of malignant tumors that invade neighboring tissues and can also metastasize to distant parts of the body through the lymphatic system or bloodstream. A “cancer” or “cancer tissue” can include a tumor.
[0046] CD3 refers to a human antigen which is expressed on T cells as part of the multimolecular T cell receptor (TCR) complex and which consists of a homodimer or heterodimer formed from the association of two or four receptor chains: CD3 epsilon, CD3 delta, CD3 zeta and CD3 gamma. Human CD3 epsilon comprises the amino acid sequence of SEQ ID NO: 2. SEQ ID NO: 3 shows the extracellular domain of CD3 epsilon.
SEQ ID NO: 2
MQSGTHWRVLGLCLLSVGVWGQDGNEEMGGITQTPYKVSISGTTVILTC PQYPGSEILWQHNDKNIGGDEDDKNIGSDEDHLSLKEFSELEQSGYYVCY PRGSKPEDANFYLYLRARVCENCMEMDVMSVATIVIVDICITGGLLLLVY YWSKNRKAKAKPVTRGAGAGGRQRGQNKERPPPVPNPDYEPIRKGQRD LYSGLNQRRI
SEQ ID NO: 3
DGNEEMGGITQTPYKVSISGTTVILTCPQYPGSEILWQHNDKNIGGDEDD KNIGSDEDHLSLKEFSELEQSGYYVCYPRGSKPEDANFYLYLRARVCENC MEMD
[0047] “CH3 region” or “CH3 domain” refers to the CH3 region of an immunoglobulin. The CH3 region of human IgGl antibody corresponds to amino acid residues 341-446. However, the CH3 region can also be any of the other antibody isotypes as described herein.
[0048] “Complementarity determining regions” (CDR) are antibody regions that bind an antigen. CDRs can be defined using various delineations such as Kabat (Wu et al. J Exp Med 132: 211-50, 1970) (Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, Md., 1991), Chothia (Chothia et al. J Mol Biol 196: 901-17, 1987), IMGT (Lefranc et al. Dev Comp Immunol 27: 55-77, 2003) and AbM (Martin and Thornton J Bmol Biol 263: 800- 15, 1996). The correspondence between the various delineations and variable region numbering are described (see e.g. Lefranc et al. Dev Comp Immunol 27: 55-77, 2003; Honegger and Pluckthun, J Mol Biol 309:657-70, 2001; International ImMunoGeneTics (IMGT) database; Web resources, http://www_imgt_org). Available programs such as
abYsis by UCL Business PLC can be used to delineate CDRs. The term “CDR”, “HCDR1”, “HCDR2”, “HCDR3”, “LCDR1”, “LCDR2” and “LCDR3” as used herein includes CDRs defined by any of the methods described supra, Kabat, Chothia, IMGT or AbM, unless otherwise explicitly stated in the specification. Preferably, the term “CDR”, “HCDR1”, “HCDR2”, “HCDR3”, “LCDR1”, “LCDR2” and “LCDR3” as used herein includes CDRs defined by the method of Kabat.
[0049] “Comprising” is intended to include examples encompassed by the terms “consisting essentially of’ and “consisting of’; similarly, the term “consisting essentially of’ is intended to include examples encompassed by the term “consisting of.” Unless the context clearly requires otherwise, throughout the description and the claims, the words “comprise”, “comprising”, and the like are to be construed in an inclusive sense as opposed to an exclusive or exhaustive sense; that is to say, in the sense of “including, but not limited to”.
[0050] “Fc gamma receptor” (FcyR) refers to well-known FcyRI, FcyRIIa, FcyRIIb or FcyRIII. Activating FcyR includes FcyRI, FcyRIIa and FcyRIII.
[0051] “Human antibody” refers to an antibody that is optimized to have minimal immune response when administered to a human subject. Variable regions of human antibody are derived from human immunoglobulin sequences. If human antibody contains a constant region or a portion of the constant region, the constant region is also derived from human immunoglobulin sequences. Human antibody comprises heavy and light chain variable regions that are “derived from” sequences of human origin if the variable regions of the human antibody are obtained from a system that uses human germline immunoglobulin or rearranged immunoglobulin genes. Such exemplary systems are human immunoglobulin gene libraries displayed on phage, and transgenic non-human animals such as mice or rats carrying human immunoglobulin loci. “Human antibody” typically contains amino acid differences when compared to the immunoglobulins expressed in humans due to differences between the systems used to obtain the human antibody and human immunoglobulin loci, introduction of somatic mutations or intentional introduction of substitutions into the frameworks or CDRs, or both. Typically, “human antibody” is at least about 80%, 81%, 82%, 83%, 84%, 85%, 86%, 87%, 88%, 89%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% or 99% identical in amino acid sequence to an amino acid sequence encoded by human germline immunoglobulin or rearranged immunoglobulin genes. In some cases, “human antibody”
can contain consensus framework sequences derived from human framework sequence analyses, for example as described in Knappik et al., (2000) J Mol Biol 296:57-86, or synthetic HCDR3 incorporated into human immunoglobulin gene libraries displayed on phage, for example as described in Shi et al., (2010) J Mol Biol 397:385-96, and in Int. Patent Publ. No. W02009/085462. Antibodies in which at least one CDR is derived from a non-human species are not included in the definition of “human antibody”.
[0052] “Humanized antibody” refers to an antibody in which at least one CDR is derived from non-human species and at least one framework is derived from human immunoglobulin sequences. Humanized antibody can include substitutions in the frameworks so that the frameworks can not be exact copies of expressed human immunoglobulin or human immunoglobulin germline gene sequences.
[0053] “Identity” refers to a relationship between the sequences of two or more polypeptide molecules or two or more nucleic acid molecules, as determined by aligning and comparing the sequences. “Percent (%) sequence identity” with respect to a reference polypeptide sequence is defined as the percentage of amino acid residues in a candidate sequence that are identical with the amino acid residues in the reference polypeptide sequence, after aligning the sequences and introducing gaps, if necessary, to achieve the maximum percent sequence identity, and not considering any conservative substitutions as part of the sequence identity. Alignment for purposes of determining percent amino acid sequence identity can be achieved in various ways that are within the skill in the art, for instance, using publicly available computer software such as BLAST, BLAST-2, ALIGN, or MEGALIGN (DNAStar, Inc.) software. Those skilled in the art can determine appropriate parameters for aligning sequences, including any algorithms needed to achieve maximal alignment over the full length of the sequences being compared.
[0054] “Isolated” refers to a homogenous population of molecules (such as synthetic polynucleotides or a protein such as an antibody) which have been substantially separated and/or purified away from other components of the system the molecules are produced in, such as a recombinant cell, as well as a protein that has been subjected to at least one purification or isolation step. “Isolated antibody” refers to an antibody that is substantially free of other cellular material and/or chemicals and encompasses antibodies that are isolated to a higher purity, such as to 80%, 81%, 82%, 83%, 84%, 85%, 86%,
87%, 88%, 89%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 99% or 100% purity.
[0055] “Monoclonal antibody” refers to an antibody obtained from a substantially homogenous population of antibody molecules, i.e., the individual antibodies comprising the population are identical except for possible well-known alterations such as removal of C-terminal lysine from the antibody heavy chain or post-translational modifications such as amino acid isomerization or deamidation, methionine oxidation or asparagine or glutamine deamidation. Monoclonal antibodies typically bind one antigenic epitope. A bispecific monoclonal antibody binds two distinct antigenic epitopes. Monoclonal antibodies can have heterogeneous glycosylation within the antibody population. Monoclonal antibody can be monospecific or multispecific such as bispecific, monovalent, bivalent or multivalent.
[0056] “Mutation” refers to an engineered or naturally occurring alteration in a polypeptide or polynucleotide sequence when compared to a reference sequence. The alteration can be a substitution, insertion or deletion of one or more amino acids or polynucleotides.
[0057] “Negative minimal residual disease status” or “negative MRD status” or “MRD negative” refers to the PerMillionCount (i.e., a point estimate of malignant myeloma cells per million nucleated cells) in a patients on-study bone marrow sample relative to their reference bone marrow sample (i.e., Teclistamab treatment naive bone marrow sample). Based on this PerMillionCount, each sample is determined to be positive or negative. Samples are positive if the PerMillionCount is greater than or equal to the limit of sensitivity, otherwise they are negative. Negative minimal residual disease status can be determined at a sensitivity of 0.01% (IO-4), 0.001% (10-5) or 0.0001% (10‘ 6). Negative minimal residual disease status can be determined using next generation sequencing (NGS).
[0058] “Pharmaceutical composition” refers to composition that comprises an active ingredient and a pharmaceutically acceptable carrier.
[0059] “Pharmaceutically acceptable carrier” or “excipient” refers to an ingredient in a pharmaceutical composition, other than the active ingredient, which is nontoxic to a subject.
[0060] “Recombinant” refers to DNA, antibodies and other proteins that are prepared, expressed, created or isolated by recombinant means when segments from different sources are joined to produce recombinant DNA, antibodies or proteins.
[0061] “Refractory” multiple myeloma refers to disease that is non-responsive to therapy or stops responding to therapy.
[0062] “Relapsed” multiple myeloma refers to disease that responded to prior treatment but then progressed and requires new therapy.
[0063] “Step-up dose” refers to a dose of an active agent that is administered to a subject prior to a treatment dose. A step-up dose is lower than the treatment dose. To prevent or lessen certain toxicities, such as cytokine release syndrome (CRS), a “priming” dose strategy may include one or more lower step-up dose(s) followed by the higher treatment doses. A “step-up phase” refers to an initial phase of a therapeutically effective regimen in which at least one step-up dose of a therapeutic is administered to the subject. A step-up phase may also include one or more treatment doses, z.e., a step- up phase may include one or more step-up doses followed by one or more treatment doses; for example, a step-up phase may include two step-up doses followed by two treatment doses. In particular embodiments, the step-up phase is 28 days, z.e., the step- up phase is a 28-day cycle of a therapeutically effective regimen.
[0064] “Subject” as used herein refers to a human subject. Except when noted, the terms “patient” or “subject” are used interchangeably.
[0065] “T cell redirecting therapeutic” refers to a molecule containing two or more binding regions, wherein one of the binding regions specifically binds a cell surface antigen on a target cell or tissue and wherein a second binding region of the molecule specifically binds a T cell antigen. Examples of cell surface antigen include a tumor associated antigen, such as BCMA. Examples of T cell antigen include, e.g., CD3. This dual/multi-target binding ability recruits T cells to the target cell or tissue leading to the eradication of the target cell or tissue.
[0066] “Therapeutically effective amount” refers to an amount effective, at doses and for periods of time necessary, to achieve a desired therapeutic result. A therapeutically effective amount can vary depending on factors such as the disease state, age, sex, and weight of the individual, and the ability of a therapeutic or a combination of therapeutics to elicit a desired response in the individual. Exemplary indicators of an
effective therapeutic or combination of therapeutics that include, for example, improved well-being of the patient.
[0067] “Treat” or “treatment” refers to both therapeutic treatment and prophylactic or preventative measures, wherein the object is to prevent or slow down (lessen) an undesired physiological change or disorder. Beneficial or desired clinical results include alleviation of symptoms, diminishment of extent of disease, stabilized (i.e., not worsening) state of disease, delay or slowing of disease progression, amelioration or palliation of the disease state, and remission (whether partial or total), whether detectable or undetectable. “Treatment” can also mean prolonging survival as compared to expected survival if a subject was not receiving treatment. Those in need of treatment include those already with the condition or disorder as well as those prone to have the condition or disorder or those in which the condition or disorder is to be prevented.
[0068] “Treatment dose” refers to a dose of the active agent that is administered to a subject to treat a disease. A treatment dose may be administered at a regular dosing interval on a repetitive basis (e.g., weekly, biweekly, monthly). A treatment dose may be preceded by one or more step-up doses.
[0069] A patient that is “triple-class exposed” refers to a multiple myeloma patient that has previously been treated with (at a minimum) a proteasome inhibitor, an immunomodulatory agent and an anti-CD38 monoclonal antibody.
[0070] “Tumor cell” or a “cancer cell” refers to a cancerous, pre-cancerous or transformed cell, either in vivo, ex vivo, or in tissue culture, that has spontaneous or induced phenotypic changes. These changes do not necessarily involve the uptake of new genetic material. Although transformation can arise from infection with a transforming virus and incorporation of new genomic nucleic acid, uptake of exogenous nucleic acid or it can also arise spontaneously or following exposure to a carcinogen, thereby mutating an endogenous gene. Transformation/cancer is exemplified by morphological changes, immortalization of cells, aberrant growth control, foci formation, proliferation, malignancy, modulation of tumor specific marker levels, invasiveness, tumor growth in suitable animal hosts such as nude mice, and the like, in vitro, in vivo, and ex vivo.
[0071] The numbering of amino acid residues in the antibody constant region throughout the specification is according to the EU index as described in Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service,
National Institutes ofHealth, Bethesda, MD. (1991), unless otherwise explicitly stated. Antibody constant chain numbering can be found for example at ImMunoGeneTics website, at IMGT Web resources at IMGT Scientific charts.
[0072] Conventional one and three-letter amino acid codes are used herein as shown in Table 1.
Table 1.

BCMAxCD3 bispecific antibodies for the treatment of HR-SMM
[0073] Although the last decade has seen the development of effective target therapies for participants with multiple myeloma (MM), the clinical utility of targeted therapies has been hampered by the development of drug resistance, clonal evolution and disease progression making the quest for cure ever more elusive for MM. Even with the best combinations of agents that are currently available; cure is not achieved for most participants with MM. Therefore, the treatment of the precursor smoldering multiple myeloma (SMM) states of MM may lead to the ultimate prevention of progression and cure in MM. Without being bound by theory, it is believed that early intervention in high-risk SMM provides an opportunity to prevent or delay progression, or even cure the
disease, by aggressively targeting the tumor cells before clonal heterogeneity occurs and before immune dysfunction and microenvironmental dysregulation occurs.
[0074] The goal of therapy in high-risk SMM should be to deliver as highly effective therapy as possible to ultimately achieve cure or significant delay in progression-free survival (PFS) without compromising safety. The present inventors have developed novel methods for treating high-risk SMM using BCMAxCD3 bispecific antibodies, which provide significant efficacy compared to patients with relapsed/refractory multiple myeloma that receive the same therapy.
[0075] Teclistamab (marketed as TECVAYLI®) is the first BCMA-directed bispecific antibody approved for the treatment of patients with relapsed or refractory multiple myeloma. Teclistamab is a bispecific B-cell maturation antigen (BCMA)- directed CD3 T-cell engager indicated for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least three or four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent and an anti- CD38 monoclonal antibody. The efficacy of teclistamab is continuing to be evaluated in patients with relapsed or refractory multiple myeloma in a multi-center clinical study (MajesTEC-1, NCT03145181 [Phase 1] and NCT04557098 [Phase 2]). The study has included patients who previously received at least three prior therapies, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody. In the MajesTEC-1 study, at 14. 1-month median follow-up, teclistamab demonstrated rapid, deep and durable responses, with an overall response rate (ORR) of 63% and median progression-free survival (mPFS) of 11.3 months. The most common grade 3/4 hematologic adverse events (AEs) were neutropenia (64.2 percent); anemia (37 percent); lymphopenia (32.7 percent) and thrombocytopenia (21.2 percent). Infections occurred in 76.4 percent of patients (44.8 percent grade 3/4). The most common nonhematologic AE was cytokine release syndrome (CRS), all of which were grade 1/2 except for 1 transient grade 3 CRS (72.1 percent all grade). See, e.g., Usmani SZ, et al. Lancet 2021;398:665-674, and Moreau P, et al. New Engl J Med 2022; 387: 495-505, which are incorporated by reference herein.
Antibodies
[0076] Any suitable BCMAxCD3 bispecific antibody known to those skilled in the art in view of the present disclosure can be used.
[0077] Various bispecific antibody formats include formats described herein and recombinant IgG-like dual targeting molecules, wherein the two sides of the molecule each contain the Fab fragment or part of the Fab fragment of at least two different antibodies; IgG fusion molecules, wherein full length IgG antibodies are fused to an extra Fab fragment or parts of Fab fragment; Fc fusion molecules, wherein single chain Fv molecules or stabilized diabodies are fused to heavy-chain constant-domains, Fc- regions or parts thereof; Fab fusion molecules, wherein different Fab-fragments are fused together; ScFv- and diabody-based and heavy chain antibodies (e.g., domain antibodies, nanobodies) wherein different single chain Fv molecules or different diabodies or different heavy-chain antibodies (e.g. domain antibodies, nanobodies) are fused to each other or to another protein or carrier molecule, or bispecific antibodies generated by arm exchange. Exemplary bispecific formats include dual targeting molecules include Dual Targeting (DT)-Ig (GSK/Domantis), Two-in-one Antibody (Genentech) and mAb2 (F- Star), Dual Variable Domain (DVD)-Ig (Abbott), DuoBody (Genmab), Ts2Ab (Medlmmune/AZ) and BsAb (Zymogenetics), HERCULES (Biogen Idee) and TvAb (Roche), ScFv/Fc Fusions (Academic Institution), SCORPION (Emergent BioSolutions/Trubion, Zymogenetics/BMS) and Dual Affinity Retargeting Technology (Fc-DART) (MacroGenics), F(ab)2 (Medarex/AMGEN), Dual-Action or Bis-Fab (Genentech), Dock-and-Lock (DNL) (ImmunoMedics), Bivalent Bispecific (Biotecnol) and Fab-Fv (UCB-Celltech), Bispecific T Cell Engager (BITE) (Micromet), Tandem Diabody (Tandab) (Affimed), Dual Affinity Retargeting Technology (DART) (MacroGenics), Single-chain Diabody (Academic), TCR-like Antibodies (AIT, ReceptorLogics), Human Serum Albumin ScFv Fusion (Merrimack) and COMBODY (Epigen Biotech), dual targeting nanobodies (Ablynx), dual targeting heavy chain only domain antibodies. Various formats of bispecific antibodies have been described, for example in Chames and Baty (2009) Curr Opin Drug Disc Dev 12: 276 and in Nunez- Prado et al., (2015) Drug Discovery Today 20(5):588-594.
[0078] In some embodiments, the BCMAxCD3 bispecific antibody comprises any one of the BCMA binding domains described in W02017/031104, the entire content of which is incorporated herein by reference. In some embodiments, the BCMAxCD3 bispecific antibody comprises any one of the CD3 binding domains described in W02017/031104. In some embodiments, the BCMAxCD3 bispecific antibody comprises any one of the BCMAxCD3 bispecific antibodies described in W02017/031104.
[0079] In some embodiments, the BCMAxCD3 bispecific antibody is chimeric, humanized or human.
[0080] In some embodiments, the bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype. In preferred embodiments, the bispecific antibody is an IgG4 isotype. An exemplary wild-type IgG4 comprises an amino acid sequence of SEQ ID NO: 34.
SEQ ID NO: 34:
ASTKGPSVFPLAPCSRSTSESTAALGCLVKDYFPEPVTVSWNSGALTSGV HTFPAVLQSSGLYSLSSVVTVPSSSLGTKTYTCNVDHKPSNTKVDKRVES KYGPPCPSCPAPEFLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSQEDP EVQFNWYVDGVEVHNAKTKPREEQFNSTYRVVSVLTVLHQDWLNGKE YKCKVSNKGLPSSIEKTISKAKGQPREPQVYTLPPSQEEMTKNQVSLTCL VKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSRLTVDKSRW QEGNVFSCSVMHEALHNHYTQKSLSLSLGK
[0081] The bispecific antibody can be of any allotype. It is expected that allotype has no influence on properties of the bispecific antibodies, such as binding or Fc-mediated effector functions. Immunogenicity of therapeutic antibodies is associated with increased risk of infusion reactions and decreased duration of therapeutic response (Baert et al., (2003) N Engl J Med 348:602-08). The extent to which therapeutic antibodies induce an immune response in the host can be determined in part by the allotype of the antibody (Stickler et al., (2011) Genes and Immunity 12:213-21). Antibody allotype is related to amino acid sequence variations at specific locations in the constant region sequences of the antibody. Table 2 shows select IgGl, IgG2 and IgG4 allotypes.
Table 2.
 [0082] In some embodiments, the bispecific antibody comprises one or more Fc substitutions that reduces binding of the bispecific antibody to a Fey receptor (FcyR) and/or reduces Fc effector functions such as Clq binding, complement dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC) or phagocytosis (ADCP). The specific substitutions can be made in comparison to the wildtype IgG4 of SEQ ID NO: 34.
[0082] In some embodiments, the bispecific antibody comprises one or more Fc substitutions that reduces binding of the bispecific antibody to a Fey receptor (FcyR) and/or reduces Fc effector functions such as Clq binding, complement dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC) or phagocytosis (ADCP). The specific substitutions can be made in comparison to the wildtype IgG4 of SEQ ID NO: 34.
[0083] Fc positions that can be substituted to reduce binding of the Fc to the activating FcyR and subsequently to reduce effector function are substitutions L234A/L235A on IgGl, V234A/G237A/P238S/H268A/V309L/A330S/P331S on IgG2, F234A/L235A on IgG4, S228P/F234A/ L235A on IgG4, N297A on all Ig isotypes, V234A/G237A on IgG2, K214T/E233P/ L234V/L235A/G236- deleted/A327G/P331A/D365E/L358M on IgGl, H268Q/V309L/ A330S/P331S on IgG2, S267E/L328F on IgGl, L234F/L235E/D265A on IgGl, L234A/L235A/G237A/P238S/H268A/A330S/P331S on IgGl, S228P/F234A/L235A/G237A/P238S on IgG4, and S228P/F234A/L235A/G236- deleted/G237A/P238S on IgG4, wherein residue numbering is according to the EU index.
[0084] Fc substitutions that can be used to reduce CDC are a K322A substitution. [0085] Well-known S228P substitution can further be made in IgG4 antibodies to enhance IgG4 stability.
[0086] In some embodiments, the bispecific antibody comprises one or more asymmetric substitutions in a first CH3 domain or in a second CH3 domain, or in both the first CH3 domain and the second CH3 domain.
[0087] In some embodiments, the one or more asymmetric substitutions is selected from the group consisting of F405L/K409R, wild-type/F405L_R409K, T366Y/F405A, T366W/F405W, F405W/Y407A, T394W/Y407T, T394S/Y407A, T366W/T394S, F405W/T394S and T366W/T366S_L368A_Y407V, L351Y_F405A_Y407V/T394W, T366I_K392M_T394W/F405A_Y407V, T366L_K392M_T394W/F405A_Y407V, L351Y_Y4O7A/T366A_K4O9F, L351Y_Y4O7A/T366V_K4O9F, Y407A/T366A_K409F and T350V_L35 lY_F405A_Y407V/T350V_T366L_K392L_T394W.
[0088] In some embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises phenylalanine at position 405 and arginine at position 409 in a first heavy
chain (HC1) and leucine at position 405 and lysine at position 409 in a second heavy chain (HC2), wherein residue numbering is according to the EU Index.
[0089] In some embodiments, the BCMAxCD3 bispecific antibody comprises proline at position 228, alanine at position 234 and alanine at position 235 in both the HC1 and the HC2.
[0090] Tables 3 and 4 provide sequences of an exemplary embodiment of a BCMAxCD3 bispecific antibody, according to the Kabat numbering system.
Table 3. Exemplary sequences of a BCMA binding arm


Table 4. Exemplary sequences of a CD3 binding arm


[0091] In some embodiments, the BCMAxCD3 bispecific antibody is CC-93269, BI 836909, JNJ-64007957 (teclistamab), or PF-06863135. In preferred embodiments, the BCMAxCD3 bispecific antibody is teclistamab (also referred to herein as Tec), which has the sequences described in Tables 3 and 4.
[0092] Teclistamab and its methods of use are described, for example, in WO 2017/031104, WO 2019/220369 and WO 2021/228783, which are incorporated by reference herein. According to particular embodiments, the BCMAxCD3 bispecific antibody has an amino acid sequence with at least 80%, at least 85%, at least 90%, at
least 95%, at least 98%, or at least 99% sequence identity to the amino acid sequence of teclistamab.
[0093] Additional embodiments of BCMAxCD3 bispecific antibodies that may be used in accordance with the methods are described below.
[0094] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
[0095] In certain embodiments, the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 11, and the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
[0096] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype.
[0097] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype.
[0098] In certain embodiments, the BCMAxCD3 bispecific antibody comprises one or more substitutions in its Fc region.
[0099] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region (according to EU index numbering).
[0100] In certain embodiments, the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region (according to EU index numbering).
[0101] In certain embodiments, the Fc region of the BCMA binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively (according to EU index numbering).
[0102] In certain embodiments, the Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions (according to EU index numbering).
[0103] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
[0104] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
[0105] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
[0106] In certain embodiments, the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
[0107] In certain embodiments, the BCMAxCD3 bispecific antibody is teclistamab.
Patient populations with high-risk smoldering multiple myeloma
[0108] The inventors have developed novel methods of treating human subjects that have been diagnosed with high-risk smoldering multiple myeloma (HR-SMM). BCMAxCD3 bispecific antibodies disclosed herein are safe and highly effective in treating HR-SMM.
[0109] The diagnosis of smoldering (asymptomatic) multiple myeloma (SMM) is based on the demonstration of M-protein in serum (>3 gm/dL) or urine and/or the presence of 10-60% clonal bone marrow plasma cells (BMPC). Patients with SMM generally have an annual risk of progression of 10% for the first 5 years. As such, SMM is thought to comprise a mixture of high-risk patients, who may benefit from early therapeutic intervention before irreversible organ damage and symptoms appear. These high-risk SMM patients are defined as having a 50% progression rate within 2 years. The rationale is that early therapeutic interception of disease progression in these high-risk individuals will prevent/delay end-organ damage with all of its morbidities. In addition, early intervention before clonal evolution with secondary acquisition of mutations along with immune-suppressive deregulation of the microenvironment may lead to a significant improvement in disease response, progression-free survival, and overall survival.
[0110] It is recognized in the art that a patient with high-risk smoldering multiple myeloma generally meets either the Mayo 2018 Criteria (“20-2-20” critieria) or the International Myeloma Working Group Scoring System for SMM (see, e.g., Lakshman A, et al. Risk stratification of smoldering multiple myeloma incorporating revised IMWG diagnostic criteria. Blood Cancer J 2018;8:59; and Mateos MV, et al. International Myeloma Working Group risk stratification model for smoldering multiple myeloma. Blood Cancer J 2020; 10: 102, which are incorporated by reference herein). Thus, a patient with high-risk smoldering multiple myeloma generally meets one of the following two diagnostic criteria (i.e., either Diagnostic Criteria #1 or Diagnostic Criteria #2 below) as shown in Table 7:
Table 7. HR-SMM Diagnostic Criteria


[0111] Embodiments provide methods of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody. In preferred embodiments, the subject has not received prior SMM directed therapy. In preferred embodiments, the BCMAxCD3 bispecific antibody is administered as a monotherapy (i.e., without another concurrent SMM directed therapy).
[0112] In certain embodiments, there are provided methods of preventing or inhibiting development of HR-SMM into symptomatic multiple myeloma (MM) in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody. In certain embodiments, there are provided methods of curing HR-SMM in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody. In certain embodiments, there are provided methods of achieving a complete response (CR)
in a subject diagnosed with HR-SMM, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody. In certain embodiments, there are provided methods of achieving an overall response rate (ORR) of 100% in a population of subjects diagnosed with HR-SMM, comprising administering to each of the subjects a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
Dosing regimens for the treatment of HR-SMM
[0113] The inventors have developed novel dosing regimens for the treatment of HR- SMM that achieve deep and durable clinical responses.
[0114] As used herein, “weight-based” refers to administration of a dose amount that is based on the subject’s specific body weight; for example, 3 mg/kg refers to a dose of 3 milligrams of antibody per kilogram of the subject’s body weight. Unless otherwise specified herein, when a dose is described in a unit of “mg/kg” or “pg/kg,” weight-based dosing is being employed.
[0115] Unless otherwise specified herein, a BCMAxCD3 bispecific antibody, such as teclistamab, is administered on a dosing schedule based on sequential 28-day cycles, for example, Cycle 1 starts on Day 1 of Cycle 1 and ends on Day 28 of Cycle 1, and then Day 1 of Cycle 2 starts the day after Day 28 of Cycle 1 and ends on Day 28 of Cycle 2, and then Day 1 of Cycle 3 starts the day after Day 28 of Cycle 2 and ends on Day 28 of Cycle 3, and so on. As used herein with respect to treatment cycles, “Cl” refers to Cycle 1, “C2” refers to Cycle 2, “C3” refers to Cycle 3, and so on. Multiple cycles may also be described, e.g., “C3-6” refers to Cycles 3-6 (Cycles 3, 4, 5 and 6). A cycle number with a “+” symbol refers to that cycle and all subsequent cycles, e.g., “C3+” refers to from Cycle 3 and all subsequent cycles (i.e., C3, C4, C5, C6, C7, and so on).
[0116] As used herein “Q4W” means once every four weeks, “Q2W” (also referred to as “bi-weekly” or “biweekly”) means once every two weeks, and “QW” (also referred to as “weekly”) means once weekly. Q4W is sometimes referred to herein as “monthly” but technically refers to once every 4 weeks or once every 28 days (e.g., in 28-day cycles, a first treatment dose occurs on Day 1 of Cycle 1, a second treatment dose occurs on Day 1 of Cycle 2, etc.). Administration of a treatment dose once weekly (QW) is also referred to herein as a weekly dosing schedule; for example, a 28-day treatment cycle may have a weekly dosing schedule that comprises four doses one week apart from each
other (e.g., on Days 1, 8, 15 and 22), or three doses one week apart from each other (e.g., on Days 8, 15 and 22), or two doses one week apart from each other (e.g., on Days 8 and 15). Administration of a treatment dose once every two weeks (Q2W) is also referred to herein as a bi-weekly dosing schedule. Administration of a treatment dose once every four weeks (Q4W) is also referred to herein as a monthly dosing schedule. Dosing regimens may be described herein in terms of the dose amount and frequency; for example, “Cl: 1.5 mg/kg QW” refers to administration of 1.5 mg/kg once per week in Cycle 1 of a therapeutically effective regimen, “C3-6: 3 mg/kg Q2W” refers to administration of 3 mg/kg once every two weeks from Cycle 3 through Cycle 6, “C7+: 3 mg/kg Q4W” refers to administration of 3 mg/kg once every four weeks starting in Cycle 7, etc.
[0117] As used herein, a “BCMAxCD3 treatment cycle” refers to each treatment cycle in a therapeutically effective regimen in which at least one treatment dose of a BCMAxCD3 bispecific antibody is administered to the subject. In preferred embodiments, the first BCMAxCD3 treatment cycle in a therapeutically effective regimen is preceded by a step-up phase.
[0118] Additional abbreviations used herein include the following: CR, complete response; PR, partial response; Q2W, once every 2 weeks; Q4W, once every 4 weeks; QW, once weekly; RP2D, recommended phase 2 dose; SUD, step-up dose.
[0119] According to embodiments, methods of treating HR-SMM are effective in eliciting a clinical response in a subject as determined by International Myeloma Working Group (IMWG) 2016 response criteria. According to particular embodiments, the methods of treatment are effective in eliciting a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as determined by IMWG 2016 response criteria. As used herein, overall response rate (ORR) refers to the percentage of patients in a population that achieve a partial response (PR) or better, i.e., a partial response, very good partial response, complete response or stringent complete response. Unless indicated otherwise herein, PR, VGPR, CR and sCR are as defined by the IMWG (2016) criteria. IMWG (2016) response criteria are known in the art, and provided in Table A below.
Table 8.

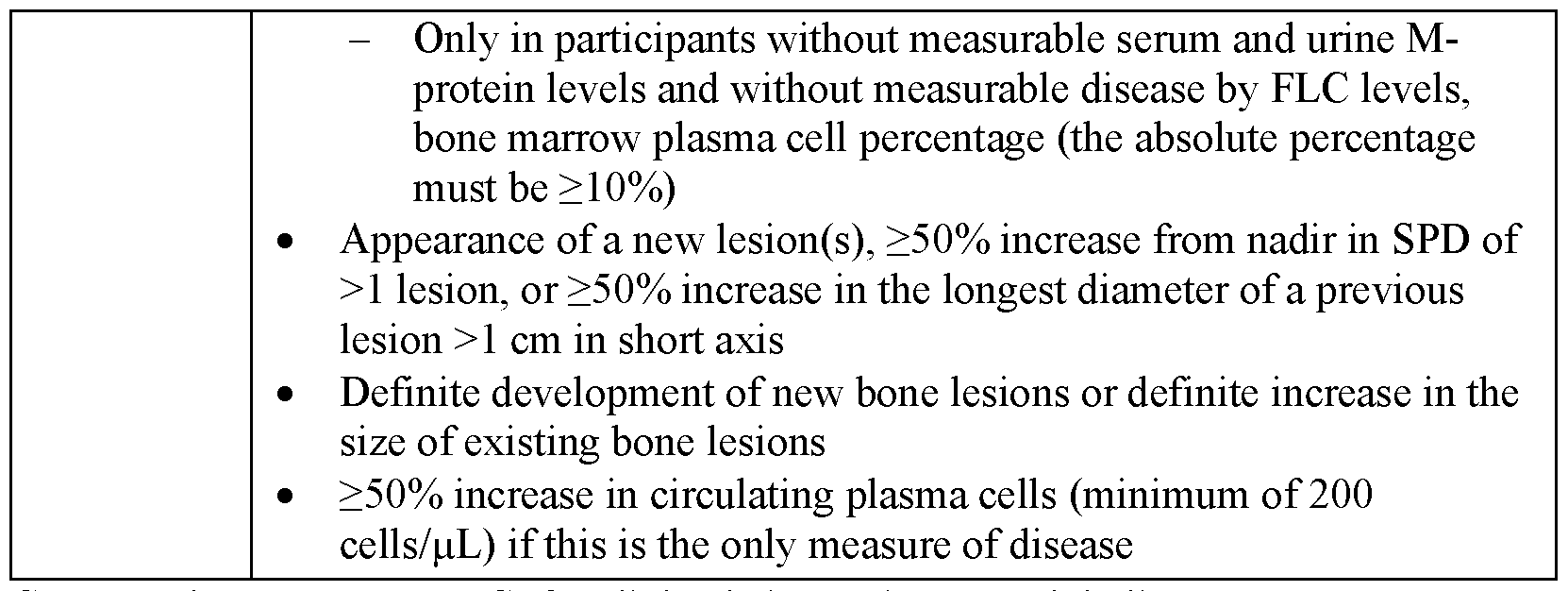
CR=complete response; FLC=free light chain; Ig=immunoglobulin; M- protein=monoclonal protein; PC=plasma cell; PR=partial response; sCR=stringent complete response; SPD=sum of the products of the maximal perpendicular diameters of measured lesions; VGPR=very good partial response. a. Clarifications to the criteria for coding CR and VGPR in participants in whom the only measurable disease is by serum FLC levels: CR in such participants indicates a normal FLC ratio of 0.26 to 1.65 (or reference range for sponsor central laboratory for this study: 0.22 to 1.52) in addition to CR criteria listed above. VGPR in such participants requires a >90% decrease in the difference between involved and uninvolved FLC levels. b. In some cases, it is possible that the original M-protein light chain isotype is still detected on immunofixation, but the accompanying heavy-chain component has disappeared; this would not be considered as a CR even though the heavy -chain component is not detectable, because it is possible that the clone evolved to one that secreted only light chains. Thus, if a participant has IgA lambda myeloma, then to qualify as CR there should be no IgA detectable on serum or urine immunofixation; if free lambda is detected without IgA, then it must be accompanied by a different heavy-chain isotype (IgG, IgM, etc.). c. Clarifications to the criteria for coding progressive disease: bone marrow criteria for progressive disease are to be used only in participants without measurable disease by M-protein and by FLC levels; “25% increase” refers to M-protein, and FLC, and does not refer to bone lesions, or soft-tissue plasmacytomas and the “lowest response value” does not need to be a confirmed value.
[0120] IMWG criteria for response to Multiple Myeloma treatment are also described, for example, in Durie et al., Kumar et al. and Rajkumar et al., which are incorporated by reference herein: Durie BG, Harousseau JL, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9): 1467-1473; Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328-346; Rajkumar SV, Harousseau JL, Durie B, et al. Consensus
recommendations for the uniform reporting of clinical Trials: report of the International Myeloma Workshop Consensus Panel 1. Blood. 2011; 117(18):4691-4695.
[0121] Embodiments provide methods of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising treating the subject according to a therapeutically effective regimen that comprises sequential BCMAxCD3 treatment cycles. In preferred embodiments, each sequential BCMAxCD3 treatment cycle is 28 days.
[0122] In certain embodiments, the method comprises administering each dose of the BCMAxCD3 bispecific antibody subcutaneously.
[0123] In certain embodiments, one or more step-up doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during a step-up phase (e.g., wherein the step-up phase is Cycle 1 of a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles). In preferred embodiments, the step-up phase is 28 days.
[0124] In certain embodiments, 1-3 step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase. For example, in certain embodiments, two step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
[0125] In certain embodiments, the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody. For example, in certain embodiments, the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody and a second step-up dose of 0.3 mg/kg of the BCMAxCD3 bispecific antibody.
[0126] In certain embodiments, one or more treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses. For example, in certain embodiments, two or three treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, after the one or more step-up doses have been administered. In certain embodiments, each of the treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase is 0.72 mg/kg or 1.5 mg/kg or 3.0 mg/kg. In preferred embodiments, each of the one or more treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase is administered in an amount of 1.5 mg/kg.
[0127] In certain embodiments, the step-up phase comprises subcutaneously administering two step-up doses and three treatment doses of the BCMAxCD3 bispecific antibody. In other embodiments, the step-up phase comprises subcutaneously administering two step-up doses and two treatment doses of the BCMAxCD3 bispecific antibody. In preferred embodiments, two or three treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
[0128] In certain embodiments, the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg and a second treatment dose of 1 .5 mg/kg. [0129] In certain embodiments, the second step-up dose is administered 2-4 days after first step-up dose. In certain embodiments, the second step-up dose is administered 2 days after first step-up dose. In certain embodiments, the first treatment dose is administered 4-7 days after the second step-up dose. In certain embodiments, the first treatment dose is administered 5 days after the second step-up dose. In certain embodiments, the second treatment dose is administered 5-9 days after the first treatment dose. In certain embodiments, the second treatment dose is administered 7 days after the first treatment dose.
[0130] In certain embodiments, the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg, a second treatment dose of 1.5 mg/kg and a third treatment dose of 1.5 mg/kg. In certain embodiments, the third treatment dose is administered 5-9 days after the second treatment dose. In certain embodiments, the third treatment dose is administered 7 days after the second treatment dose.
[0131] In certain embodiments, the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step- up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8 and a second treatment dose of 1.5 mg/kg on Day 15. In certain embodiments, the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8, a second treatment dose of 1 .5 mg/kg on Day 15 and a third treatment dose of 1.5 mg/kg on Day 22.
[0132] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses.
[0133] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses.
[0134] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., six, twelve or eighteen BCMAxCD3 treatment cycles), subcutaneously administering monthly (Q4W) treatment doses.
[0135] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, in Cycle 2, subcutaneously administering weekly (QW) treatment doses, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses; and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses.
[0136] In certain embodiments, each treatment dose of the BCMAxCD3 bispecific antibody is administered to the subject in an amount of 1.5 mg/kg or 3 mg/kg. In preferred embodiments, each weekly (QW) treatment dose is 1.5 mg/kg, each bi-weekly (Q2W) treatment dose is 3.0 mg/kg, and each monthly (Q4W) treatment dose is 3.0 mg/kg.
[0137] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg.
[0138] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg.
[0139] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
[0140] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, in Cycle
2, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg; and [0141] starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
[0142] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering biweekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
[0143] In certain embodiments, the method comprises administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg (e.g., on Day 1), a second step-up dose of 0.3 mg/kg (e.g., on Day 3), and then weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
[0144] An exemplary embodiment of a dosing regimen is provided below:
1. Cycle 1: Dose is administered on Days 1, 3, 8, 15 and 22 of a 28-day treatment cycle. Step-up doses are given on Days 1 and 3 of Cycle 1; treatment doses are given on Days 8, 15 and 22 of Cycle 1.
2. Cycle 2 (28-day cycle): Dose is administered on Days 1, 8, 15 and 22.
3. Cycles 3-6 (28-day cycles): treatment is administered on Days 1 and 15.
4. Cycles 7-24 (28-day cycles): treatment is administered on Day 1.
An exemplary embodiment of a dosing regimen is also provided in Table 9 (Cycle 1) and Table 10 (Cycles 2-24).
Table 9. Treatment Cycle 1 (step-up phase) of an exemplary dosing regimen

*Weight based dosing calculation based on institutional standard
Table 10. Cycles 2-24 of an exemplary dosing regimen

*Weight based dosing calculation based on institutional standard
[0145] Another exemplary embodiment of a dosing regimen is provided in Table 11 (Cycle 1) and Table 12 (Cycles 2-12).
Table 11. Treatment Cycle 1 (step-up phase) of an exemplary dosing regimen

*Weight based dosing calculation based on institutional standard
Table 12. Cycles 2-12 of an exemplary dosing regimen

*Weight based dosing calculation based on institutional standard
[0146] According to certain embodiments, one or more pretreatment medications are administered to the subject prior to administration of a dose of the BCMAxCD3 bispecific antibody. According to certain embodiments, one or more pretreatment medications are administered to the subject during Cycle 1 (step-up phase). According to certain embodiments, one or more pretreatment medications are administered to the subject during Cycle 1 (step-up phase) and Cycle 2. According to certain embodiments, one or more pretreatment medications are selected from the group consisting of dexamethasone, diphenhydramine, acetaminophen, and any combination thereof. According to an exemplary embodiment, pretreatment medications are administered to the subject as shown in Table 13, in which “x” signifies administration of the pretreatment medication for the indicated day.
Table 13. Pretreatment medications

[0147] In certain embodiments, the methods achieve a clinical response in the subject that is a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as defined by IMWG (2016) response criteria.
[0148] In certain embodiments, the methods achieve a CR, VGPR, or PR in the subject, as defined by IMWG (2016) response criteria.
[0149] In certain embodiments, the methods achieve a VGPR or PR in the subject, as defined by IMWG (2016) response criteria.
[0150] In certain embodiments, the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 70% or higher.
[0151] In certain embodiments, the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 75% or higher.
[0152] In certain embodiments, the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 80% or higher.
[0153] In certain embodiments, the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 85% or higher.
[0154] In certain embodiments, the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 90% or higher.
[0155] In certain embodiments, the methods achieve an overall response rate (ORR) in a population of subjects with HR-SMM of 95% or higher.
[0156] In certain embodiments, the methods achieve an overall response rate (ORR) of 100% in a population of subjects with HR-SMM.
[0157] In certain embodiments, the methods achieve a CR in at least 25% of a population of subjects with HR-SMM.
[0158] In certain embodiments, the methods achieve a CR in at least 30% of a population of subjects with HR-SMM.
[0159] In certain embodiments, the methods achieve a CR in at least 35% of a population of subjects with HR-SMM.
[0160] In certain embodiments, the methods achieve a CR in at least 40% of a population of subjects with HR-SMM.
[0161] In certain embodiments, the methods achieve MRD-negative disease in the subject.
[0162] In certain embodiments, after the subject has received at least four 28 -day cycles of treatment with the BCMAxCD3 bispecific antibody, the subject’s HR-SMM does not progress. In certain embodiments, administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twenty-four (24) 28-day treatment cycles prevents the subject from developing multiple myeloma.
[0163] In certain embodiments, administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twelve (12) 28-day treatment cycles prevents the subject from developing multiple myeloma. In certain embodiments, the method cures the HR- SMM and prevents the subject from developing MM.
[0164] In certain embodiments, the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM that is greater than an ORR achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
[0165] In certain embodiments, the method achieves a percentage of complete responses (CRs) in a population of subjects with HR-SMM that is greater than a percentage of CRs achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
EXEMPLARY EMBODIMENTS
[0166] Provided below are enumerated embodiments. These embodiments are illustrative only and do not limit the scope of the present disclosure or of the claims attached hereto.
1. A method of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
2. The method of embodiment 1, wherein the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
3. The method of embodiment 1 or 2, wherein the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 11, and the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
4. The method of any of embodiments 1-3, wherein the BCMAxCD3 bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype.
5. The method of any of embodiments 1-4, wherein the BCMAxCD3 bispecific antibody is an IgG4 isotype.
6. The method of any of embodiments 1-5, wherein the BCMAxCD3 bispecific antibody comprises one or more substitutions in its Fc region.
7. The method of any of embodiments 1-6, wherein the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region (according to EU index numbering).
8. The method of any of embodiments 1-7, wherein the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region (according to EU index numbering).
9. The method of any of embodiments 1-8, wherein the Fc region of the BCMA binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively (according to EU index numbering).
10. The method of any of embodiments 1-9, wherein the Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions (according to EU index numbering).
11. The method of any of embodiments 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
12. The method of any of embodiments 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
13. The method of any of embodiments 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2)
having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
14. The method of any of embodiments 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
15. The method of any of embodiments 1-10, wherein the BCMAxCD3 bispecific antibody is teclistamab.
16. The method of any of embodiments 1-15, wherein the subject has not received prior SMM directed therapy.
17. The method of any of embodiments 1-16, wherein the subject does not have symptomatic multiple myeloma.
18. The method of any of embodiments 1-17, wherein the BCMAxCD3 bispecific antibody is administered as a monotherapy (i.e., without another concurrent SMM directed therapy).
19. The method of any of embodiments 1-18, comprising subcutaneously administering each dose of the BCMAxCD3 bispecific antibody.
20. The method of any of embodiments 1-19, comprising treating the subject according to a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles.
21. The method of any of embodiments 1-20, wherein one or more step-up doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during a step-up phase (e.g., wherein the step-up phase is Cycle 1 of a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles).
22. The method of embodiment 21, wherein the step-up phase is 28 days.
23. The method of any embodiment 21 or 22, wherein 1-3 step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
24. The method of any of embodiments 21-23, wherein two step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
25. The method of any of embodiments 21-24, wherein the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody.
26. The method of any of embodiments 21-25, wherein the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody and a second step-up dose of 0.3 mg/kg of the BCMAxCD3 bispecific antibody.
27. The method of any of embodiments 21-26, wherein one or more treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
28. The method of any of embodiments 21-27, wherein two treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
29. The method of any of embodiments 21-28, wherein three treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
30. The method of any of embodiments 21-29, wherein the step-up phase comprises subcutaneously administering two step-up doses and two treatment doses of the BCMAxCD3 bispecific antibody.
31. The method of any of embodiments 21-29, wherein the step-up phase comprises subcutaneously administering two step-up doses and three treatment doses of the BCMAxCD3 bispecific antibody.
32. The method of any of embodiments 27-31, wherein the one or more treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase are administered in an amount of 0.72 mg/kg or 1.5 mg/kg or 3.0 mg/kg.
33. The method of any of embodiments 27-31, wherein each of the one or more treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase is administered in an amount of 1.5 mg/kg.
34. The method of any of embodiments 27-33, wherein two or three treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
35. The method of any of embodiments 27-33, wherein two treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
36. The method of any of embodiments 27-33, wherein three treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
37. The method of any of embodiments 21-29, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg and a second treatment dose of 1.5 mg/kg.
38. The method of embodiment 37, wherein the second step-up dose is administered 2-4 days after first step-up dose.
39. The method of embodiment 37, wherein the second step-up dose is administered 2 days after first step-up dose.
40. The method of any of embodiments 37-39, wherein the first treatment dose is administered 4-7 days after the second step-up dose.
41. The method of any of embodiments 37-39, wherein the first treatment dose is administered 5 days after the second step-up dose.
42. The method of any of embodiments 37-41, wherein the second treatment dose is administered 5-9 days after the first treatment dose.
43. The method of any of embodiments 37-41, wherein the second treatment dose is administered 7 days after the first treatment dose.
44. The method of any of embodiments 21-43, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8 and a second treatment dose of 1.5 mg/kg on Day 15.
45. The method of any of embodiments 37-44, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg, a second treatment dose of 1.5 mg/kg and a third treatment dose of 1.5 mg/kg.
46. The method of embodiment 45, wherein the third treatment dose is administered 5-9 days after the second treatment dose.
47. The method of embodiment 45, wherein the third treatment dose is administered 7 days after the second treatment dose.
48. The method of any of embodiments 21-47, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8, a second treatment dose of 1.5 mg/kg on Day 15 and a third treatment dose of 1.5 mg/kg on Day 22.
49. The method of any of embodiments 1-48, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses.
50. The method of any of embodiments 1-48, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses.
51. The method of any of embodiments 1-48, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles (e.g., one BCMAxCD3 treatment cycle), subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles (e.g., four BCMAxCD3 treatment cycles) subcutaneously administering bi-weekly (Q2W) treatment doses, and then
in one or more subsequent BCMAxCD3 treatment cycles (e.g., six, twelve or eighteen BCMAxCD3 treatment cycles), subcutaneously administering monthly (Q4W) treatment doses.
52. The method of any of embodiments 1-48, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, in Cycle 2, subcutaneously administering weekly (QW) treatment doses, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses; and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses.
53. The method of any of embodiments 1-52, wherein each treatment dose of the BCMAxCD3 bispecific antibody is administered to the subject in an amount of 1.5 mg/kg or 3 mg/kg (e.g., wherein each weekly treatment dose is 1.5 mg/kg, each biweekly treatment dose is 3.0 mg/kg, and each monthly treatment dose is 3.0 mg/kg).
54. The method of any of embodiments 1-53, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg.
55. The method of any of embodiments 1-54, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg.
56. The method of any of embodiments 1-55, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
57. The method of any of embodiments 1-56, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, in Cycle 2, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg; and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
58. The method of any of embodiments 1-57, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
59. The method of any of embodiments 1-58, comprising administering the BCMAxCD3 bispecific antibody (e.g., teclistamab) according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg (e.g., on Day 1), a second step-up dose of 0.3 mg/kg (e.g., on Day 3), and then weekly (QW) treatment doses of 1.5 mg/kg (e.g., on Days 8, 15 and 22), in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg (e.g., on Days 1, 8, 15 and 22), in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg (e.g., on Days 1 and 15); and starting in Cycle 7 (e.g., in Cycles 7-12 or Cycles 7-24), subcutaneously administering monthly (Q4W) doses of 3 mg/kg (e.g., on Day 1 of each cycle).
60. The method of any of embodiments 1-59, wherein the wherein the method achieves a clinical response in the subject that is a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as defined by IMWG (2016) response criteria.
61. The method of any of embodiments 1-59, wherein the method achieves a CR, VGPR, or PR in the subject, as defined by IMWG (2016) response criteria.
62. The method of any of embodiments 1-59, wherein the method achieves a VGPR or PR in the subject, as defined by IMWG (2016) response criteria.
63. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 70% or higher.
64. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 75% or higher.
65. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 80% or higher.
66. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 85% or higher.
67. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 90% or higher.
68. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 95% or higher.
69. The method of any of embodiments 1-62, wherein the method achieves an overall response rate (ORR) of 100% in a population of subjects with HR-SMM.
70. The method of any of embodiments 1-69, wherein the method achieves a CR in at least 25% of a population of subjects with HR-SMM.
71. The method of any of embodiments 1-69, wherein the method achieves a CR in at least 30% of a population of subjects with HR-SMM.
72. The method of any of embodiments 1-69, wherein the method achieves a CR in at least 35% of a population of subjects with HR-SMM.
73. The method of any of embodiments 1-69, wherein the method achieves a CR in at least 40% of a population of subjects with HR-SMM.
74. The method of any of embodiments 1-73, wherein the method achieves MRD-negative disease in the subject.
75. The method of any of embodiments 1-74, wherein, after the subject has received at least four 28-day cycles of treatment with the BCMAxCD3 bispecific antibody, the subject’s HR-SMM does not progress.
76. The method of any of embodiments 1-75, wherein administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twenty-four (24) 28- day treatment cycles prevents the subject from developing multiple myeloma.
77. The method of any of embodiments 1-75, wherein administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twelve (12) 28-day treatment cycles prevents the subject from developing multiple myeloma.
78. The method of any of embodiments 1-77, wherein the method cures the HR- SMM and prevents the subject from developing MM.
79. The method of any of embodiments 1-78, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM that is greater than an ORR achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
80. The method of any of embodiments 1-79, wherein the method achieves a percentage of complete responses (CRs) in a population of subjects with HR-SMM that is greater than a percentage of CRs achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
[0167] Those skilled in the art will appreciate that numerous changes and modifications can be made to the preferred embodiments and that such changes and modifications can be made without departing from the spirit of the invention. It is, therefore, intended that the appended claims cover all such equivalent variations.
[0168] The disclosures of each patent, patent application, and publication cited or described in this document are hereby incorporated herein by reference, in its entirety.
EXAMPLES
[0169] The following examples are provided to further describe some of the embodiments disclosed herein. The examples are intended to illustrate, not to limit, the disclosed embodiments.
Example 1: A Randomized Phase II Platform Study of Bispecific Antibodies in High-Risk Smoldering Myeloma (Immuno-PRISM)
Antibodies
[0170] Anti-BCMA/anti-CD3 antibody teclistamab (also called Tec) (e.g., described in W02017031104A1, the content of which is incorporated herein by reference in its entirety) was made by Janssen Pharmaceuticals. Teclistamab comprises a BCMA binding arm BCMB69 and a CD3 binding arm CD3B219, the amino acid sequences of which are shown in Table 5 and Table 6, respectively.
Table 5. Sequences of BCMA binding arm of Teclistamab

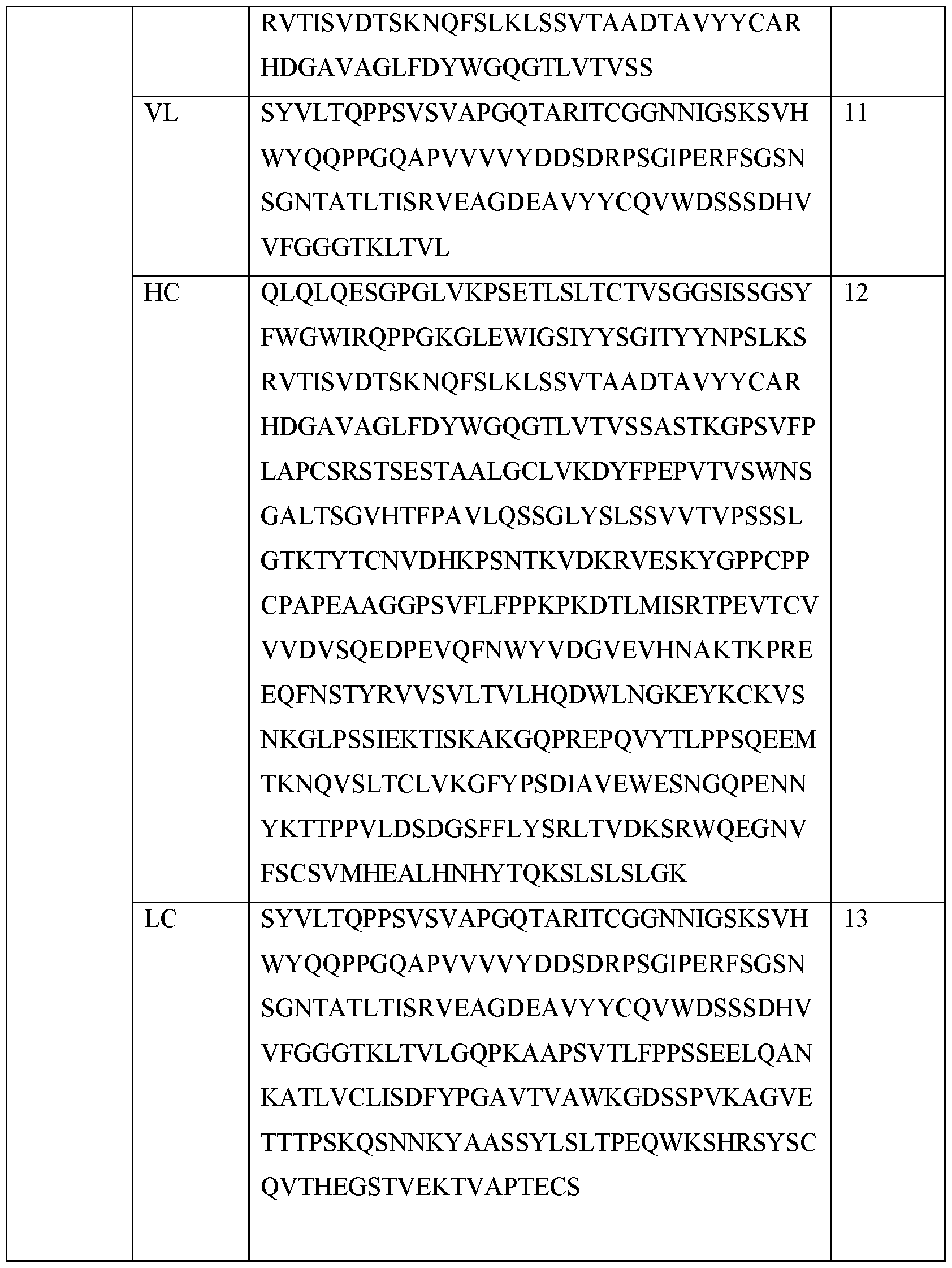
Table 6. Sequences of CD3 binding arm of Teclistamab



Aims:
[0171] To evaluate the anti-cancer activity of bispecific antibodies, including teclistamab (also referred to as “TEC” or “Tec”), against a control arm of lenalidomide and dexamethasone, for the treatment of high-risk smoldering multiple myeloma (HR- SMM).
Methods:
[0172] This is a multiple arm, randomized, phase II, platform study evaluating TEC vs lenalidomide and dexamethasone in HR-SMM. Eligibility criteria included HR-SMM per Mayo 2018 “20-2-20” model, total IMWG risk score of 9 or greater, and other previously established high-risk criteria including PETHEMA criteria, evolving-type SMM, and high-risk FISH abnormalities.
[0173] This study has an initial, safety run-in cohort of 6 patients treated with TEC. All patients receive 2 step-up doses of subcutaneous TEC. In the safety run-in, patients receive a dose lower than the recommended phase 2 dose (RP2D) of TEC. If no dose limiting toxicities (DLTs) are observed, the next cohort receives the RP2D of TEC. Once safety run-in is complete, the randomized trial begins with 2: 1 randomization to TEC (30 patients) vs control arm of lenalidomide and dexamethasone (15 patients). Treatment duration is for 24 cycles. TEC is given at a dose of 1.5 mg/kg weekly for cycles 1 and 2 followed by 3 mg/kg on days 1 and 15 for cycles 3 to 6, and monthly starting with cycle 7 for a total of 24 cycles (2 years). For the control arm, lenalidomide is given at a dose of 25 mg orally on days 1-21 and dexamethasone 40mg is given weekly during the 28-day cycle for 24 cycles. All eligible patients undergo stem cell collection after 4 cycles of therapy.
[0174] The primary objective is complete response rate. Secondary objectives include PFS, ORR, MRD negativity rates, pharmacokinetics of TEC, and safety. Exploratory objectives include mass spectrometry quantification of M protein, molecular evolution of tumor cells, and immune biomarkers of response.
Eligibility Criteria:
[0175] Inclusion Criteria
- Age > 18 years.
- High risk SMM defined as having 1 of the following 2 criteria:
1) High risk per "20-2-20" Criteria defined as presence of any two of the following:
• Serum M-spike > 2 gm/dL
• Involved to uninvolved free light chain (FLC) ratio> 20
• Bone Marrow Plasma Cell (BMPC) % > 20%
OR total score of 9 using the following scoring system:
• Free Light Chain (FLC) Ratio o >10-25 = 2 o >25-40 = 3 o > 40 = 5
• Serum M-Protein (g/dL) o >1.5-3 = 3 o >3 = 4
• Bone Marrow Plasma Cell (BMPC) % o >15-20 = 2 o >20-30 = 3 o >30-40 = 5 o >40 = 6
• Fluorescence In Situ Hybridization (FISH) abnormality (t(4, 14), t(14, 16), Iq gain, or dell3q = 2)
2) Presence of >10% BMPC and at least one of the following:
• Evolving pattern: o Evolving M-Protein (eMP: >10% increase in Serum Mi- Protein) over a 6 month period OR; o Evolving change in hemoglobin (eHb) > 0.5 g/dl decrease over a 12 month period OR;
o Progressive Involved light chain increase > 10% over a 6 month period along with a light chain ratio > 8
• Abnormal PC immunophenotype (> 95% of BMPCs are clonal) and reduction of >1 uninvolved immunoglobulin isotype. (Only IgG; IgA and IgM will be considered)
• High risk cytogenetics defined as presence of t(4; 14), t( 14; 16), t(14;20), 17p deletion, TP53 mutation, Iq gain
• Monoclonal light chain excretion of > 200mg/24 hours for those with monoclonal light chain smoldering multiple myeloma.
No evidence of CRAB criteria* or new criteria of active MM (SLIM-CRAB) which include the following:
1) Increased calcium levels: Corrected serum calcium >0.25 mmol/L (>lmg/dL) above the upper limit of normal or >2.75 mmol/L (>1 Img/dL);
2) Renal insufficiency (attributable to myeloma);
3) Anemia (Hgb 2g/dL below the lower limit of normal or <10g/dL);
4) Bone lesions (lytic lesions or generalized osteoporosis with compression fractures)
5) No evidence of the following new criteria for active MM including the following:
6) Bone marrow plasma cells >60%
7) Serum involved/uninvolved FLC ratio >100
8) Serum involved/uninvolved FLC ratio >100 is not considered a MDE if urinary monoclonal protein is <200mg/24 hours.82
9) MRI with more than one focal lesion
* Participants with CRAB criteria that are attributable to conditions other than the disease under study may be eligible after discussion with the Sponsor Investigator.
ECOG Performance Status (PS) 0, 1, or 2
The following laboratory values obtained <28 days prior to registration:
• ANC >1000/mL
• PLT >75,000/mL
• Total bilirubin < 2.0 mg/dL (If total is elevated check direct and if normal patient is eligible.)
• AST <2.5 x institutional upper limit of normal (ULN)
• ALT <2.5 x institutional upper limit of normal (ULN)
• Estimated creatinine clearance CLcr >60 mL/min (Cockcroft Gault equation).
- All female participants of child-bearing potential must have a negative pregnancy test before enrollment.
[0176] Exclusion Criteria
Prior SMM directed therapy administered within 6 months of beginning treatment on study. To avoid including primary refractory cases to the lenalidomide arm, participants who received a prior lenalidomide-based therapy should have had at least an MR to be considered on this trial.
Symptomatic Multiple Myeloma or any evidence of CRAB criteria, including presence of myeloma defining events (MDE). Any prior therapy for active Myeloma should also be excluded. Prior therapy for smoldering myeloma is not an exclusion criterion. Bisphosphonates are not excluded.
Other concurrent chemotherapy, immunotherapy, radiotherapy, or any ancillary therapy considered investigational. Prior therapy with bisphosphonate is allowed. Prior radiation therapy to a solitary plasmacytoma is allowed but had to be at least 6 months prior to enrollment on the trial. Prior clinical trials or therapy for smoldering MM or MGUS are allowed per exclusion criteria described above. Serious medical or psychiatric illness likely to interfere with participation in this clinical study.
Diagnosed or treated for another malignancy within 2 years of enrollment. Uncontrolled intercurrent illness including, but not limited to, ongoing or active infection, symptomatic congestive heart failure, unstable angina pectoris, cardiac arrhythmia, or psychiatric illness/social situations that would limit compliance with study requirements.
Plans to father a child while enrolled in this study or within 90 days after receiving the last dose of study drug.
Pregnant or breast-feeding or planning to become pregnant while enrolled in this study or within 90 days after receiving the last dose of study drug.
Known seropositive for or active viral infection with human immunodeficiency virus (HIV), hepatitis B virus (HBV) or hepatitis C virus (HCV)
Participants who are seropositive because of hepatitis B virus vaccine are eligible.
Participants who are positive for HIV 1 and 2 antibody, hepatitis B core antibody or hepatitis B surface antigen must have a negative polymerase chain reaction (PCR) result before enrollment. Those who are PCR positive will be excluded. Contraindications or life-threatening allergies, hypersensitivity, or intolerance to any study drug or its excipients (refer to the teclistamab Investigator’s Brochure and appropriate package inserts).
Prior or concurrent exposure to any of the following:
• Investigational vaccine within 4 weeks
• Live, attenuated vaccine within 4 weeks before randomization.
• Monoclonal antibody therapy within 21 days
• Cytotoxic therapy within 14 days
• PI therapy within 14 days
• IMiD agent therapy within 14 days
• Radiotherapy within 14 days or focal radiation within 7 days
- A maximum cumulative dose of corticosteroids of >140 mg of prednisone or equivalent within 14-day period before the first dose of study drug (does not include pretreatment medications) (Appendix 10)
Known active CNS involvement or exhibits clinical signs of meningeal involvement of multiple myeloma. If either is suspected, negative whole brain MRI and lumbar cytology are required.
Myelodysplastic syndrome or active malignancies (i.e., progressing or requiring treatment change in the last 24 months). The only allowed exceptions are:
• Non-muscle invasive bladder cancer treated within the last 24 months that is considered completely cured
• Skin cancer (non-melanoma or melanoma) treated within the last 24 months that is considered completely cured.
• Noninvasive cervical cancer treated within the last 24 months that is considered completely cured
• Localized prostate cancer (N0M0): o With a Gleason score of <6, treated within the last 24 months, or untreated and under surveillance o With a Gleason score of 3+4 that has been treated >6 months prior to full study screening and considered to have a very low risk of recurrence, or
• History of localized prostate cancer and receiving androgen deprivation therapy and considered to have a very low risk of recurrence.
• Breast cancer: adequately treated lobular carcinoma in situ or ductal carcinoma in situ, or history of localized breast cancer and receiving antihormonal agents and considered to have a very low risk of recurrence.
• Other malignancy that is considered cured with minimal risk of recurrence. Stroke or seizure within 6 months prior to signing ICF
Presence of the following cardiac conditions:
• New York Heart Association stage III or IV congestive heart failure
• Myocardial infarction or coronary artery bypass graft <6 months prior to randomization
• History of clinically significant ventricular arrhythmia or unexplained syncope, not believed to be vasovagal in nature or due to dehydration
• History of severe non-ischemic cardiomyopathy
Major surgery within 2 weeks prior to the start of administration of study treatment, or will not have fully recovered from surgery, or has major surgery planned during the time the participant is expected to be treated in the study or within 2 weeks after administration of the last dose of study treatment.
NOTE: Participants with planned surgical procedures to be conducted under local anesthesia may participate. Kyphoplasty or vertebroplasty are not considered major surgery. If there is a question whether a procedure is considered a major surgery, the investigator must consult with the appropriate sponsor representative and resolve any issues before enrolling a participant in the study.
Concurrent medical or psychiatric condition or disease that is likely to interfere with study procedures or results, or that in the opinion of the investigator would constitute a hazard for participating in this study, such as:
• Uncontrolled diabetes defined by Hemoglobin A1C > 8.5
• Acute diffuse infiltrative pulmonary disease
• Evidence of active systemic viral, fungal, or bacterial infection, requiring systemic antimicrobial therapy
• History of autoimmune disease with the exception of vitiligo, type I diabetes, and prior autoimmune thyroiditis that is currently euthyroid based on clinical symptoms and laboratory testing
• Disabling psychiatric conditions (e.g., alcohol or drug abuse), severe dementia, or altered mental status
• Any other issue that would impair the ability of the participant to receive or tolerate the planned treatment at the investigational site, to understand informed consent or any condition for which, in the opinion of the investigator, participation would not be in the best interest of the participant (e.g., compromise the well-being) or that could prevent, limit, or confound the protocol-specified assessments
• History of non-compliance with recommended medical treatments
[0177] Results: At the time of data cut off, 19 patients have been enrolled in the study with median follow up of 6 months. The median age is 59 years old (range 35-73) with 9 females (47%) and 10 males (53%). Sixty-four percent of patients that had evaluable FISH results had high-risk abnormalities as follows: Iq gain (7 patients), t(4; 14) 1 patient.
[0178] No DLTs were observed in the safety run-in cohort and patients are now enrolling into the randomized portion of trial. In the TEC cohort (12 patients), grade 3 or greater hematologic toxicities were neutropenia (4 patients, resolved) and thrombocytopenia (1 patient, resolved). Grade 3 or greater non-hematologic toxicities were ALT increased in 3 patients (grade 3, resolved) and pancreatitis in 1 patient (grade 3, resolved). Infections occurred in 9 patients but only 1 patient had grade 3 infection (sinusitis). Remainder of the infections were low grade and were mostly upper respiratory infections (6 patients). One patient had grade 2 uveitis. CRS occurred in 75% of patients (all grade 1 except 2 patients with grade 2 CRS requiring tocilizumab, all resolved). No patients experienced ICANS with no delayed neurotoxicity observed. All patients treated with TEC are receiving IVIG with mean IgG level at start of IVIG treatment of 418 mg/dL, with 64% of patients achieving normalization of IgG values within two IVIG doses.
[0179] In the TEC- treated cohorts (12 patients), the ORR is 100% with 42% achieving a CR, 25% VGPR, 33% PR. Four patients with high-risk FISH receiving TEC have achieved a CR within 5 cycles. In control arm of lenalidomide and dexamethasone (3 patients), the ORR is 66% without any complete responses to date. Of the 8 evaluable patients treated with TEC, the MRD negative rate at 10‘6 is 100%, including 2 patients
with VGPR-MRD negative disease. Average time to MRD negativity observed among evaluable patients was 4.25 cycles. No patients have progressed on treatment. Stem cell collection was successful in all eligible patients with an average stem cell yield of 9.06 x 106 CD34+ cells/kg.
[0180] Conclusions: Teclistamab in HR-SMM demonstrates significant activity with 100% ORR, with MRD-negative disease in 100% of evaluable patients to date, and overall significantly improved safety profile compared to RRMM.
Claims
1. A method of treating high-risk smoldering multiple myeloma (HR-SMM) in a subject in need thereof, comprising administering to the subject a therapeutically effective amount of a BCMAxCD3 bispecific antibody.
2. The method of claim 1, wherein the BCMAxCD3 bispecific antibody comprises a BCMA binding domain comprising the HCDR1 of SEQ ID NO: 4, the HCDR2 of SEQ ID NO: 5, the HCDR3 of SEQ ID NO: 6, the LCDR1 of SEQ ID NO: 7, the LCDR2 of SEQ ID NO: 8 and the LCDR3 of SEQ ID NO: 9, and a CD3 binding domain comprising the HCDR1 of SEQ ID NO: 14, the HCDR2 of SEQ ID NO: 15, the HCDR3 of SEQ ID NO: 16, the LCDR1 of SEQ ID NO: 17, the LCDR2 of SEQ ID NO: 18 and the LCDR3 of SEQ ID NO: 19.
3. The method of claim 1 or 2, wherein the BCMA binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 10 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO:
11, and the CD3 binding domain comprises a heavy chain variable region (VH) having the amino acid sequence of SEQ ID NO: 20 and a light chain variable region (VL) having the amino acid sequence of SEQ ID NO: 21.
4. The method of any of claims 1-3, wherein the BCMAxCD3 bispecific antibody is an IgGl, an IgG2, an IgG3 or an IgG4 isotype.
5. The method of any of claims 1-4, wherein the BCMAxCD3 bispecific antibody is an IgG4 isotype.
6. The method of any of claims 1-5, wherein the BCMAxCD3 bispecific antibody comprises one or more substitutions in its Fc region.
7. The method of any of claims 1-6, wherein the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in its Fc region.
8. The method of any of claims 1-7, wherein the BCMAxCD3 bispecific antibody is an IgG4 isotype and comprises F405L and R409K substitutions in its Fc region.
9. The method of any of claims 1-8, wherein the Fc region of the BCMA binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively .
10. The method of any of claims 1-9, wherein the Fc region of the CD3 binding arm comprises Proline/Alanine/Alanine substitutions at amino acid positions 228/234/235, respectively, in addition to F405L and R409K substitutions.
11. The method of any of claims 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having the amino acid sequence of SEQ ID NO: 23.
12. The method of any of claims 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 90% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 90% identity to the amino acid sequence of SEQ ID NO: 23.
13. The method of any of claims 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 95% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 95% identity to the amino acid sequence of SEQ ID NO: 23.
14. The method of any of claims 1-10, wherein the BCMAxCD3 bispecific antibody comprises a first heavy chain (HC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 12, a first light chain (LC1) having at least 98% identity to the amino acid sequence of SEQ ID NO: 13, a second heavy chain (HC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 22 and a second light chain (LC2) having at least 98% identity to the amino acid sequence of SEQ ID NO: 23.
15. The method of any of claims 1-10, wherein the BCMAxCD3 bispecific antibody is teclistamab.
16. The method of any of claims 1-15, wherein the subject has not received prior SMM directed therapy.
17. The method of any of claims 1-16, wherein the subject does not have symptomatic multiple myeloma.
18. The method of any of claims 1-17, wherein the BCMAxCD3 bispecific antibody is administered as a monotherapy (i.e., without another concurrent SMM directed therapy).
19. The method of any of claims 1-18, comprising subcutaneously administering each dose of the BCMAxCD3 bispecific antibody.
20. The method of any of claims 1-19, comprising treating the subject according to a therapeutically effective regimen that comprises sequential 28-day BCMAxCD3 treatment cycles.
21. The method of any of claims 1-20, wherein one or more step-up doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during a step-up phase.
22. The method of claim 21, wherein the step-up phase is 28 days.
23. The method of any claim 21 or 22, wherein 1-3 step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
24. The method of any of claims 21-23, wherein two step-up doses of the BCMAxCD3 bispecific antibody are administered to the subject during the step-up phase.
25. The method of any of claims 21-24, wherein the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody.
26. The method of any of claims 21-25, wherein the step-up phase comprises a first step-up dose of 0.06 mg/kg of the BCMAxCD3 bispecific antibody and a second step-up dose of 0.3 mg/kg of the BCMAxCD3 bispecific antibody.
27. The method of any of claims 21-26, wherein one or more treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
28. The method of any of claims 21-27, wherein two treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
29. The method of any of claims 21-28, wherein three treatment doses of the BCMAxCD3 bispecific antibody are subcutaneously administered to the subject during the step-up phase, in addition to the one or more step-up doses.
30. The method of any of claims 21-29, wherein the step-up phase comprises subcutaneously administering two step-up doses and two treatment doses of the BCMAxCD3 bispecific antibody.
31. The method of any of claims 21 -29, wherein the step-up phase comprises subcutaneously administering two step-up doses and three treatment doses of the BCMAxCD3 bispecific antibody.
32. The method of any of claims 27-31, wherein the one or more treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase are administered in an amount of 0.72 mg/kg or 1.5 mg/kg or 3.0 mg/kg.
33. The method of any of claims 27-31, wherein each of the one or more treatment doses of the BCMAxCD3 bispecific antibody administered during the step-up phase are administered in an amount of 1.5 mg/kg.
34. The method of any of claims 27-33, wherein two or three treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
35. The method of any of claims 27-33, wherein two treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
36. The method of any of claims 27-33, wherein three treatment doses of the BCMAxCD3 bispecific antibody are administered during the step-up phase on a weekly dosing schedule (QW).
37. The method of any of claims 21-29, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg and a second treatment dose of 1.5 mg/kg.
38. The method of claim 37, wherein the second step-up dose is administered 2-4 days after first step-up dose.
39. The method of claim 37, wherein the second step-up dose is administered 2 days after first step-up dose.
40. The method of any of claims 37-39, wherein the first treatment dose is administered 4-7 days after the second step-up dose.
41. The method of any of claims 37-39, wherein the first treatment dose is administered 5 days after the second step-up dose.
42. The method of any of claims 37-41, wherein the second treatment dose is administered 5-9 days after the first treatment dose.
43. The method of any of claims 37-41, wherein the second treatment dose is administered 7 days after the first treatment dose.
44. The method of any of claims 21-43, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8 and a second treatment dose of 1.5 mg/kg on Day 15.
45. The method of any of claims 37-44, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, a first treatment dose of 1.5 mg/kg, a second treatment dose of 1.5 mg/kg and a third treatment dose of 1.5 mg/kg.
46. The method of claim 45, wherein the third treatment dose is administered 5-9 days after the second treatment dose.
47. The method of claim 45, wherein the third treatment dose is administered 7 days after the second treatment dose.
48. The method of any of claims 21-47, wherein the step-up phase comprises subcutaneously administering to the subject a first step-up dose of 0.06 mg/kg on Day 1, a second step-up dose of 0.3 mg/kg on Day 3, a first treatment dose of 1.5 mg/kg on Day 8, a second treatment dose of 1.5 mg/kg on Day 15 and a third treatment dose of 1.5 mg/kg on Day 22.
49. The method of any of claims 1-48, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses.
50. The method of any of claims 1-48, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and
in one or more subsequent BCMAxCD3 treatment, subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles subcutaneously administering bi-weekly (Q2W) treatment doses.
51. The method of any of claims 1-48, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles subcutaneously administering bi-weekly (Q2W) treatment doses, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering monthly (Q4W) treatment doses.
52. The method of any of claims 1-48, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses, in Cycle 2, subcutaneously administering weekly (QW) treatment doses, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses; and starting in Cycle 7, subcutaneously administering monthly (Q4W) treatment doses.
53. The method of any of claims 1-52, wherein each treatment dose of the BCMAxCD3 bispecific antibody is administered to the subject in an amount of 1.5 mg/kg or 3 mg/kg.
54. The method of any of claims 1-53, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and
in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg.
55. The method of any of claims 1-54, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg.
56. The method of any of claims 1-55, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, and in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg, and then in one or more subsequent BCMAxCD3 treatment cycles, subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
57. The method of any of claims 1-56, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses and then two or more weekly (QW) treatment doses of 1.5 mg/kg, in Cycle 2, subcutaneously administering weekly (QW) treatment doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) treatment doses of 3.0 mg/kg; and starting in Cycle 7, subcutaneously administering monthly (Q4W) treatment doses of 3.0 mg/kg.
58. The method of any of claims 1-57, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering one or more step-up doses, and then two or more weekly (QW) treatment doses of 1.5 mg/kg, in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg; and starting in Cycle 7, subcutaneously administering monthly (Q4W) doses of 3 mg/kg.
59. The method of any of claims 1-58, comprising administering the BCMAxCD3 bispecific antibody according to a regimen comprising 28-day cycles, wherein the regimen comprises: in Cycle 1, subcutaneously administering a first step-up dose of 0.06 mg/kg, a second step-up dose of 0.3 mg/kg, and then weekly (QW) treatment doses of 1.5 mg/kg, in Cycle 2, subcutaneously administering weekly (QW) doses of 1.5 mg/kg, in Cycles 3-6, subcutaneously administering bi-weekly (Q2W) doses of 3 mg/kg; and starting in Cycle 7, subcutaneously administering monthly (Q4W) doses of 3 mg/kg.
60. The method of any of claims 1-59, wherein the wherein the method achieves a clinical response in the subject that is a partial response (PR), a very good partial response (VGPR), a complete response (CR) or a stringent complete response (sCR), as defined by IMWG (2016) response criteria.
61. The method of any of claims 1-59, wherein the method achieves a CR, VGPR, or PR in the subject, as defined by IMWG (2016) response criteria.
62. The method of any of claims 1-59, wherein the method achieves a VGPR or PR in the subject, as defined by IMWG (2016) response criteria.
63. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 70% or higher.
64. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 75% or higher.
65. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 80% or higher.
66. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 85% or higher.
67. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 90% or higher.
68. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM of 95% or higher.
69. The method of any of claims 1-62, wherein the method achieves an overall response rate (ORR) of 100% in a population of subjects with HR-SMM.
70. The method of any of claims 1-69, wherein the method achieves a CR in at least 25% of a population of subjects with HR-SMM.
71. The method of any of claims 1-69, wherein the method achieves a CR in at least 30% of a population of subjects with HR-SMM.
72. The method of any of claims 1-69, wherein the method achieves a CR in at least 35% of a population of subjects with HR-SMM.
73. The method of any of claims 1-69, wherein the method achieves a CR in at least 40% of a population of subjects with HR-SMM.
74. The method of any of claims 1-73, wherein the method achieves MRD- negative disease in the subject.
75. The method of any of claims 1-74, wherein, after the subject has received at least four 28-day cycles of treatment with the BCMAxCD3 bispecific antibody, the subject’s HR-SMM does not progress.
76. The method of any of claims 1-75, wherein administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twenty-four (24) 28- day treatment cycles prevents the subject from developing multiple myeloma.
77. The method of any of claims 1-75, wherein administration of the BCMAxCD3 bispecific antibody to the subject for a maximum of twelve (12) 28-day treatment cycles prevents the subject from developing multiple myeloma.
78. The method of any of claims 1-77, wherein the method cures the HR-SMM and prevents the subject from developing MM.
79. The method of any of claims 1-78, wherein the method achieves an overall response rate (ORR) in a population of subjects with HR-SMM that is greater than an
ORR achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
80. The method of any of claims 1-79, wherein the method achieves a percentage of complete responses (CRs) in a population of subjects with HR-SMM that is greater than a percentage of CRs achieved in a reference population of subjects with HR-SMM, said reference population having been administered Lenalidomide and Dexamethasone but not the BCMAxCD3 bispecific antibody.
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202363594977P | 2023-11-01 | 2023-11-01 | |
| US63/594,977 | 2023-11-01 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2025094107A1 true WO2025094107A1 (en) | 2025-05-08 |
Family
ID=93590887
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/IB2024/060769 Pending WO2025094107A1 (en) | 2023-11-01 | 2024-10-31 | Methods for treating high-risk smoldering multiple myeloma |
Country Status (1)
| Country | Link |
|---|---|
| WO (1) | WO2025094107A1 (en) |
Citations (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO1988001649A1 (en) | 1986-09-02 | 1988-03-10 | Genex Corporation | Single polypeptide chain binding molecules |
| WO1992001047A1 (en) | 1990-07-10 | 1992-01-23 | Cambridge Antibody Technology Limited | Methods for producing members of specific binding pairs |
| WO1994013804A1 (en) | 1992-12-04 | 1994-06-23 | Medical Research Council | Multivalent and multispecific binding proteins, their manufacture and use |
| WO1998044001A1 (en) | 1997-03-27 | 1998-10-08 | Commonwealth Scientific And Industrial Research Organisation | High avidity polyvalent and polyspecific reagents |
| WO2009085462A1 (en) | 2007-12-19 | 2009-07-09 | Centocor, Inc. | Design and generation of human de novo pix phage display libraries via fusion to pix or pvii, vectors, antibodies and methods |
| WO2017031104A1 (en) | 2015-08-17 | 2017-02-23 | Janssen Pharmaceutica Nv | Anti-bcma antibodies, bispecific antigen binding molecules that bind bcma and cd3, and uses thereof |
| WO2019220369A2 (en) | 2018-05-16 | 2019-11-21 | Janssen Biotech, Inc. | Methods of treating cancers and enhancing efficacy of t cell redirecting therapeutics |
| WO2021228783A1 (en) | 2020-05-11 | 2021-11-18 | Janssen Pharmaceutica Nv | Methods for treating multiple myeloma |
| WO2023019204A2 (en) * | 2021-08-11 | 2023-02-16 | Dana-Farber Cancer Institute, Inc. | Compositions and methods for treating and/or characterizing hematological malignancies and precursor conditions |
| WO2023081705A1 (en) * | 2021-11-03 | 2023-05-11 | Janssen Biotech, Inc. | Methods of treating cancers and enhancing efficacy of bcmaxcd3 bispecific antibodies |
-
2024
- 2024-10-31 WO PCT/IB2024/060769 patent/WO2025094107A1/en active Pending
Patent Citations (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO1988001649A1 (en) | 1986-09-02 | 1988-03-10 | Genex Corporation | Single polypeptide chain binding molecules |
| WO1992001047A1 (en) | 1990-07-10 | 1992-01-23 | Cambridge Antibody Technology Limited | Methods for producing members of specific binding pairs |
| WO1994013804A1 (en) | 1992-12-04 | 1994-06-23 | Medical Research Council | Multivalent and multispecific binding proteins, their manufacture and use |
| WO1998044001A1 (en) | 1997-03-27 | 1998-10-08 | Commonwealth Scientific And Industrial Research Organisation | High avidity polyvalent and polyspecific reagents |
| WO2009085462A1 (en) | 2007-12-19 | 2009-07-09 | Centocor, Inc. | Design and generation of human de novo pix phage display libraries via fusion to pix or pvii, vectors, antibodies and methods |
| WO2017031104A1 (en) | 2015-08-17 | 2017-02-23 | Janssen Pharmaceutica Nv | Anti-bcma antibodies, bispecific antigen binding molecules that bind bcma and cd3, and uses thereof |
| WO2019220369A2 (en) | 2018-05-16 | 2019-11-21 | Janssen Biotech, Inc. | Methods of treating cancers and enhancing efficacy of t cell redirecting therapeutics |
| WO2021228783A1 (en) | 2020-05-11 | 2021-11-18 | Janssen Pharmaceutica Nv | Methods for treating multiple myeloma |
| WO2023019204A2 (en) * | 2021-08-11 | 2023-02-16 | Dana-Farber Cancer Institute, Inc. | Compositions and methods for treating and/or characterizing hematological malignancies and precursor conditions |
| WO2023081705A1 (en) * | 2021-11-03 | 2023-05-11 | Janssen Biotech, Inc. | Methods of treating cancers and enhancing efficacy of bcmaxcd3 bispecific antibodies |
Non-Patent Citations (23)
| Title |
|---|
| "UniProt", Database accession no. Q02223 |
| ANONYMOUS CLINICALTRIALS ET AL: "Record History | ver. 2: 2022-08-11 | NCT05469893 | ClinicalTrials.gov", 11 August 2022 (2022-08-11), pages 1 - 21, XP093244512, Retrieved from the Internet <URL:https://clinicaltrials.gov/study/NCT05469893?tab=history&a=2#version-content-panel> * |
| ANONYMOUS CLINICALTRIALS: "NCT05955508 | ClinicalTrials.gov Record History | ver. 1: 2023-07-13 |", 13 July 2023 (2023-07-13), pages 1 - 12, XP093244942, Retrieved from the Internet <URL:https://clinicaltrials.gov/study/NCT05955508?cond=Smoldering%20Multiple%20Myeloma&term=SMM&intr=Linvoseltamab&rank=1&tab=history&a=1#version-content-panel> * |
| BAERT ET AL., N ENGL J MED, vol. 348, 2003, pages 602 - 08 |
| CHOTHIA ET AL., J MOL BIOL, vol. 196, 1987, pages 901 - 17 |
| DURIE BGHAROUSSEAU JLMIGUEL JS ET AL.: "International uniform response criteria for multiple myeloma", LEUKEMIA, vol. 20, no. 9, 2006, pages 1467 - 1473, XP037780658, DOI: 10.1038/sj.leu.2404284 |
| HONEGGERPLUCKTHUN, J MOL BIOL, vol. 309, 2001, pages 657 - 70 |
| JANSSEN EMEA: "Janssen veröffentlicht Langzeitdaten zu TECVAYLI -", 8 June 2023 (2023-06-08), pages 1 - 13, XP093245036, Retrieved from the Internet <URL:https://www.globenewswire.com/news-release/2023/06/08/2684981/0/de/Janssen-veröffentlicht-Langzeitdaten-zu-TECVAYLI-Teclistamab-die-eine-Dauer-des-Ansprechens-von-22-Monaten-bei-Patienten-mit-rezidiviertem-oder-refraktärem-multiplem-Myelom-zeigen.html> * |
| KABAT ET AL.: "Sequences of Proteins of Immunological Interest", 1991, PUBLIC HEALTH SERVICE, NATIONAL INSTITUTES OF HEALTH |
| KNAPPIK ET AL., J MOL BIOL, vol. 296, 2000, pages 57 - 86 |
| KUMAR SPAIVA BANDERSON KC ET AL.: "International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma", LANCET ONCOL., vol. 17, no. 8, 2016, pages e328 - 346, XP029663519, DOI: 10.1016/S1470-2045(16)30206-6 |
| LAKSHMAN A ET AL.: "Risk stratification of smoldering multiple myeloma incorporating revised IMWG diagnostic criteria", BLOOD CANCER J, vol. 8, 2018, pages 59 |
| LEFRANC ET AL., DEV COMP IMMUNOL, vol. 27, 2003, pages 55 - 77 |
| MARTINTHORNTON, J BMOL BIOL, vol. 263, 1996, pages 800 - 15 |
| MATEOS MV ET AL.: "International Myeloma Working Group risk stratification model for smoldering multiple myeloma", BLOOD CANCER J, vol. 10, 2020, pages 102 |
| MOREAU P ET AL., NEW ENGL J MED, vol. 387, 2022, pages 495 - 505 |
| MOREAU PHILIPPE ET AL: "Teclistamab in Relapsed or Refractory Multiple Myeloma", THE NEW ENGLAND JOURNAL OF MEDICINE, vol. 387, no. 6, 11 August 2022 (2022-08-11), US, pages 495 - 505, XP093105585, ISSN: 0028-4793, DOI: 10.1056/NEJMoa2203478 * |
| NUNEZ-PRADO ET AL., DRUG DISCOVERY TODAY, vol. 20, no. 5, 2015, pages 588 - 594 |
| RAJKUMAR SVHAROUSSEAU JLDURIE B ET AL.: "Consensus recommendations for the uniform reporting of clinical Trials: report of the International Myeloma Workshop Consensus Panel 1", BLOOD, vol. 117, no. 18, 2011, pages 4691 - 4695 |
| SHI ET AL., J MOL BIOL, vol. 397, 2010, pages 385 - 96 |
| STICKLER ET AL., GENES AND IMMUNITY, vol. 12, 2011, pages 213 - 21 |
| USMANI SZ ET AL., LANCET, vol. 398, 2021, pages 665 - 674 |
| WU ET AL., J EXP MED, vol. 132, 1970, pages 211 - 50 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| EP4249515B1 (en) | Humanized or chimeric cd3 antibodies | |
| US12098210B2 (en) | Methods of treating cancers and enhancing efficacy of BCMAxCD3 bispecific antibodies | |
| KR20230009450A (en) | Methods for Treating Multiple Myeloma | |
| JP7754506B2 (en) | Antibodies to the poliovirus receptor (PVR) and uses thereof | |
| US20250064928A1 (en) | Methods for treating multiple myeloma | |
| KR20240005691A (en) | Dosage for combination therapy with anti-CD20/anti-CD3 bispecific antibody and anti-CD79B antibody drug conjugate | |
| AU2023375177A1 (en) | Methods of treating cancers | |
| IL323989A (en) | Methods of treating multiple myeloma | |
| WO2025094107A1 (en) | Methods for treating high-risk smoldering multiple myeloma | |
| WO2025096717A1 (en) | Methods for treating multiple myeloma | |
| CA3212336A1 (en) | Methods for treating multiple myeloma | |
| US20260041768A1 (en) | Methods for treating multiple myeloma with car-t cells and bispecific antibodies | |
| US20230295292A1 (en) | Methods of treating cancers and enhancing efficacy of gprc5dxcd3 bispecific antibodies | |
| WO2024246856A1 (en) | Methods for treating multiple myeloma | |
| WO2025243241A1 (en) | Methods for treating multiple myeloma | |
| KR20260020402A (en) | Treatment methods for multiple myeloma | |
| WO2025019733A2 (en) | Methods for treating multiple myeloma | |
| WO2025094085A1 (en) | Combination regimens for treating multiple myeloma | |
| US20240409641A1 (en) | Dual acting cd1d immunoglobulin for treatment of myelodysplastic syndromes | |
| WO2025231408A2 (en) | Methods for treating multiple myeloma with car-t cells and bispecific antibodies | |
| JP2026505164A (en) | Anti-CMET antibodies and methods of use thereof | |
| HK40092168A (en) | Humanized or chimeric cd3 antibodies | |
| HK40092168B (en) | Humanized or chimeric cd3 antibodies | |
| WO2025231372A2 (en) | Methods for treating multiple myeloma with car-t cells and bispecific antibodies |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 24809431 Country of ref document: EP Kind code of ref document: A1 |