WO2024200862A1 - Dpp3 inhibitor for myocardial protection and prevention of myocardial injury in critically ill patients with blood pressure decline - Google Patents
Dpp3 inhibitor for myocardial protection and prevention of myocardial injury in critically ill patients with blood pressure decline Download PDFInfo
- Publication number
- WO2024200862A1 WO2024200862A1 PCT/EP2024/058887 EP2024058887W WO2024200862A1 WO 2024200862 A1 WO2024200862 A1 WO 2024200862A1 EP 2024058887 W EP2024058887 W EP 2024058887W WO 2024200862 A1 WO2024200862 A1 WO 2024200862A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- dpp3
- antibody
- inhibitor
- activity
- blood pressure
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/04—Peptides having up to 20 amino acids in a fully defined sequence; Derivatives thereof
- A61K38/08—Peptides having 5 to 11 amino acids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/335—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin
- A61K31/336—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin having three-membered rings, e.g. oxirane, fumagillin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/41—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having five-membered rings with two or more ring hetero atoms, at least one of which being nitrogen, e.g. tetrazole
- A61K31/4164—1,3-Diazoles
- A61K31/4184—1,3-Diazoles condensed with carbocyclic rings, e.g. benzimidazoles
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/55—Protease inhibitors
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/40—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against enzymes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/20—Immunoglobulins specific features characterized by taxonomic origin
- C07K2317/24—Immunoglobulins specific features characterized by taxonomic origin containing regions, domains or residues from different species, e.g. chimeric, humanized or veneered
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/30—Immunoglobulins specific features characterized by aspects of specificity or valency
- C07K2317/34—Identification of a linear epitope shorter than 20 amino acid residues or of a conformational epitope defined by amino acid residues
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/70—Immunoglobulins specific features characterized by effect upon binding to a cell or to an antigen
- C07K2317/76—Antagonist effect on antigen, e.g. neutralization or inhibition of binding
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/90—Immunoglobulins specific features characterized by (pharmaco)kinetic aspects or by stability of the immunoglobulin
- C07K2317/92—Affinity (KD), association rate (Ka), dissociation rate (Kd) or EC50 value
Definitions
- Subject matter of the present invention is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure for myocardial protection and/ or prevention of myocardial injury.
- Dipeptidyl peptidase 3 also known as Dipeptidyl aminopeptidase III, Dipeptidyl arylamidase III, Dipeptidyl peptidase III, Enkephalinase B or red cell angiotensinase; short name: DPP3, DPPIII - is a metallopeptidase that removes dipeptides from physiologically active peptides, such as enkephalins and angiotensins. DPP3 was identified and its activity measured in extracts of purified bovine anterior pituitary by Ellis & Nuenke 1967.
- the enzyme which is listed as EC 3.4.14.4, has a molecular mass of about 83 kDa and is highly conserved in procaryotes and eucaryotes (Prajapati & Chauhan 2011).
- the amino acid sequence of the human variant is depicted in SEQ ID NO. 1.
- DPP3 is a mainly cytosolic peptidase which is ubiquitously expressed. Despite lacking a signal sequence, a few studies reported membranous activity (Lee & Snyder 1982).
- DPP3 is a zinc-depending exo-peptidase belonging to the peptidase family M49. It has a broad substrate specificity for oligopeptides from three/ four to ten amino acids of various compositions and is also capable of cleaving after proline. DPP3 is known to hydrolyze dipeptides from the N-terminus of its substrates, including angiotensin II, III and IV; Leu- and Met-enkephalin; endomorphin 1 and 2. The metallopeptidase DPP3 has its activity optimum at pH 8.0-9.0 and can be activated by addition of divalent metal ions, such as Co2+ and Mg2+.
- divalent metal ions such as Co2+ and Mg2+.
- the most prominent substrate of DPP3 is angiotensin II (Ang II), the main effector of the reninangiotensin system (RAS).
- Ang II angiotensin II
- RAS reninangiotensin system
- the RAS is activated in cardiovascular diseases (Dostal et al. 1997. J Mol Cell Cardiol;29: 2893-902; Roks et al. 1997. Heart Vessels. Suppl 12: 119-24), sepsis, and septic shock (Correa et al. 2015. Crit Care 19: 98).
- Aug II in particular, has been shown to modulate many cardiovascular functions including the control of blood pressure and cardiac remodeling.
- Circulating DPP3 levels were shown to be increased in septic, cardiogenic and vasodilatory shock patients (Rehfeld et al. 2019. JALM 3(6): 943-953). Moreover, it was associated with an increased risk of short-term mortality and severe organ dysfunction in patients with cardiogenic shock (Deaniau et al. 2020. Eur J Heart Fail. 22(2):290-299). Moreover, in patients with severe sepsis or septic shock showed that the higher the initial cDPP3 was, the greater the need for organ support and vasopressors upon admission and the longer the need for vasopressor(s), mechanical ventilation or renal replacement therapy (RRT) and the higher the need for fluid load (Blet et al. 2021. Crit Care 25: 61).
- WO2017/182561 describes methods for determining the total amount or active DPP3 in a sample of a patient for the diagnosis of a disease related to necrotic processes. It further describes a method of treatment of necrosis-related diseases by antibodies directed to DPP3.
- WO2019/081595 describes DPP3 binder directed to and binding to specific DPP3 epitopes and its use in the prevention or treatment of diseases that are associated with oxidative stress.
- WO2021/185786 describes methods for determining DPP3 in a sample of a patient for the diagnosis, risk prediction, prognosis and monitoring in a patient infected with a coronavirus. It further describes an inhibitor of the activity of DPP3 for use in therapy or intervention in a patient infected.
- Procizumab a humanized monoclonal IgGl antibody specifically binding circulating DPP3, targets and modulates DPP3 activity, an essential regulator of cardiovascular function. Its mode of action is relevant in acute diseases that are associated with massive cell death and uncontrolled release of intracellular DPP3 into the bloodstream. Translocated DPP3 remains active in the circulation where it cleaves bioactive peptides in an uncontrolled maimer. Procizumab is able to block circulating DPP3, inhibiting bioactive peptide degradation in the bloodstream. This blockade results in stabilization of cardiovascular and renal function and reduction of short-term mortality. Preclinical studies of Procizumab in animal models of cardiovascular failure showed impressive and instant efficacy.
- Procizumab has shown to normalize ejection fraction and kidney function and reduces mortality.
- the examples in the description of the present invention show that Procizumab injection in pigs with septic shock prevented myocardial injury (given by increases of myocardial IL-6 and troponin, respectively).
- DPP3 was significantly elevated in patients with decline of blood pressure, especially in shock (e.g., septic shock, cardiogenic shock) and acute coronary syndrome (ACS). Therefore, it is plausible that an inhibitor of DPP3, especially Procizumab, is able to prevent myocardial injury in patients with decline of blood pressure, irrespective of the indication.
- an inhibitor of DPP3 activity is suitable for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury.
- Subject matter of the present invention is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure for myocardial protection and/ or prevention of myocardial injury.
- Subject matter of the present invention is an inhibitor of the activity of DPP3 for use as therapy or intervention in a critically ill patient with a reduction in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said patient is having a level of DPP3 above a predetermined threshold.
- either the level of DPP3 protein and/or the level of active DPP3 is determined and compared to a predetermined threshold level.
- Subject-matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a reduction in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said patient has a level of DPP3 in a sample of bodily fluid of said subject that is above a pre-determined threshold when determined by different methods, e.g., immunoassays, activity assays, mass spectrometric methods etc.
- DPP3 activity can be measured by detection of cleavage products of DPP3 specific substrates.
- Known peptide hormone substrates include Leu-enkephalin, Met-enkephalin, endomorphin 1 and 2, valorphin, P-casomorphin, dynorphin, proctolin, ACTH (Adrenocorticotropic hormone) and MSH (melanocytestimulating hormone; Abramic et al. 2000, Barsun et al. 2007, Dhanda et al. 2008 ⁇ .
- the cleavage of mentioned peptide hormones as well as other untagged oligopeptides e.g., Ala-Ala-Ala-Ala, Dhanda et al.
- Detection methods include, but are not limited to, HPLC analysis (e.g., Lee & Snyder 1982 ⁇ , mass spectrometry (e.g., Abramic et al. 2000), Hl-NMR analysis (e.g., Vandenberg et al. 1985 , capillary zone electrophoresis (CE; e.g., Barsun et al. 2007), thin layer chromatography (e.g., Dhanda et al. 2008) or reversed phase chromatography (e.g., Mazocco et al. 2006).
- HPLC analysis e.g., Lee & Snyder 1982 ⁇
- mass spectrometry e.g., Abramic et al. 2000
- Hl-NMR analysis e.g., Vandenberg et al. 1985
- CE capillary zone electrophoresis
- thin layer chromatography e.g., Dhanda et al. 2008
- reversed phase chromatography e.g.,
- Detection of fluorescence due to hydrolysis of fluorogenic substrates by DPP3 is a standard procedure to monitor DPP3 activity.
- Those substrates are specific di- or tripeptides (Arg-Arg, Ala-Ala, Ala- Arg, Ala-Phe, Asp-Arg, Gly-Ala, Gly-Arg, Gly-Phe, Leu-Ala, Leu-Gly, Lys-Ala, Phe-Arg, Suc-Ala-Ala- Phe) coupled to a fluorophore.
- Fluorophores include but are not limited to 0-naphtylamide (2- naphtylamide, 0NA, 2NA), 4-methoxy-0-naphtylamide (4-methoxy-2-naphtylamide) and 7-amido-4- methylcoumarin (AMC, MCA; Abramic et al. 2000, Ohkubo et al. 1999). Cleavage of these fluorogenic substrates leads to the release of fluorescent 0-naphtylamine or 7-amino-4-methylcoumarin respectively.
- DPP3 carrying samples can be immobilized and divided on a gel by electrophoresis, gels stained with fluorogenic substrate (e.g., Arg-Arg-0NA) and Fast Garnet GBC and fluorescent protein bands detected by a fluorescence reader (Ohkubo et al. 1999).
- fluorogenic substrate e.g., Arg-Arg-0NA
- the same peptides can be coupled to chromophores, such as p-nitroanilide diacetate. Detection of color change due to hydrolysis of chromogenic substrates can be used to monitor DPP3 activity.
- DPP3 activity is a Protease-GioTM Assay (commercially available at Promega).
- DPP3 specific di- or tripeptides (Arg- Arg, Ala-Ala, Ala- Arg, Ala-Phe, Asp-Arg, Gly-Ala, Gly-Arg, Gly-Phe, Leu-Ala, Leu-Gly, Lys-Ala, Phe-Arg, Suc-Ala- Ala-Phe) are coupled to aminoluciferin.
- aminoluciferin Upon cleavage by DPP3, aminoluciferin is released and serves as a substrate for a coupled luciferase reaction that emits detectable luminescence.
- DPP3 activity is measured by addition of the fluorogenic substrate Arg-Arg- 0NA and monitoring fluorescence in real time.
- the level of DPP3 is determined by contacting said sample of bodily fluid with a capture binder that binds specifically to DPP3.
- said capture binder for determining the level of DPP3 may be selected from the group of antibody, antibody fragment or non-IgG scaffold.
- said capture binder for determining the level of DPP3 is an antibody.
- Another specific embodiment of the invention comprises the use of a capture-binder that binds specifically to full-length DPP3.
- said capture-binder is immobilized on a solid phase.
- test sample is passed over the immobilized binder, and DPP3, if present in the sample, binds to the binder and is itself immobilized for detection.
- a substrate may then be added, and the reaction product may be detected to indicate the presence or amount of DPP3 in the test sample.
- the DPP3 bound to said capture molecule on a solid phase is detected with a second capture molecule specifically binding to DPP3.
- solid phase may be used to include any material or vessel in which or on which the assay may be performed and includes, but is not limited to porous materials, nonporous materials, test tubes, wells, slides, agarose resins (e.g., Sepharose from GE Healthcare Life Sciences), magnetic particals (e.g., DynabeadsTM or PierceTM magnetic beads from Thermo Fisher Scientific), etc.
- agarose resins e.g., Sepharose from GE Healthcare Life Sciences
- magnetic particals e.g., DynabeadsTM or PierceTM magnetic beads from Thermo Fisher Scientific
- the method for determining DPP3 activity in a bodily fluid sample of said subject comprises the steps:
- said separation step is a washing step that removes ingredients of the sample that are not bound to said capture-binder from the captured DPP3.
- the DPP3 substrate conversion is detected by a method selected from the group comprising: fluorescence of fluorogenic substrates (e.g. Arg-Arg-0NA, Arg-Arg-AMC), color change of chromogenic substrates, luminescence of substrates coupled to aminoluciferin, mass spectrometry, HPLC/ FPLC (reversed phase chromatography, size exclusion chromatography), thin layer chromatography, capillary zone electrophoresis, gel electrophoresis followed by activity staining (immobilized, active DPP3) or western blot (cleavage products).
- fluorescence of fluorogenic substrates e.g. Arg-Arg-0NA, Arg-Arg-AMC
- color change of chromogenic substrates e.g. chromogenic substrates
- luminescence of substrates coupled to aminoluciferin e.g. Arg-Arg-0NA, Arg-Arg-AMC
- luminescence of substrates coupled to aminoluciferin e.g.
- said substrate may be selected from the group comprising: angiotensin II, III and IV, Leu-enkephalin, Met-enkephalin, endomorphin 1 and 2, valorphin, 0- casomorphin, dynorphin, proctolin, ACTH and MSH, or di-peptides coupled to a fluorophore, a chromophore or aminoluciferin wherein the di-peptide is Arg- Arg.
- said substrate may be selected from the group comprising: A di-peptide coupled to a fluorophore, a chromophore or aminoluciferin wherein the dipeptide is Arg-Arg.
- said binder exhibits a binding affinity to DPP3 of at least 107 M-l, preferred 108 M-l, more preferred affinity is greater than 109 M-l, most preferred greater than 1010 M-l.
- such assay for determining the level of DPP3 is a sandwich immunoassay using any kind of detection technology including but not restricted to enzyme label, chemiluminescence label, electrochemiluminescence label, preferably a fully automated assay.
- a fully automated assay such an assay is an enzyme labeled sandwich assay.
- automated or fully automated assay comprise assays that may be used for one of the following systems: Roche Elecsys®, Abbott Architect®, Siemens Centauer®, Brahms Kryptor®, BiomerieuxVidas®, Alere Triage®.
- immunoassays are known and may be used for the assays and methods of the present invention, these include: mass spectrometry (MS), luminescence immunoassay (LIA), radioimmunoassays ("RIA”), homogeneous enzyme-multiplied immunoassays ("EMIT”), enzyme linked immunoadsorbent assays (“ELISA”), apoenzyme reactivation immunoassay (“ARIS”), luminescence-based bead arrays, magnetic beads based arrays, protein microarray assays, rapid test formats such as for instance dipstick immunoassays, immuno-chromatographic strip tests, rare cryptate assay and automated systems/ analysers.
- MS mass spectrometry
- LIA luminescence immunoassay
- RIA radioimmunoassays
- EMIT homogeneous enzyme-multiplied immunoassays
- ELISA enzyme linked immunoadsorbent assays
- ARIS apoenzyme reactivation immunoassay
- it may be a so-called POC-test (point-of-care) that is a test technology, which allows performing the test within less than 1 hour near the patient without the requirement of a fully automated assay system.
- POC-test point-of-care
- a test technology which allows performing the test within less than 1 hour near the patient without the requirement of a fully automated assay system.
- immunochromatographic test technology e.g., a microfluidic device.
- At least one of said two binders is labeled in said sandwich immunoassay in order to be detected.
- said label is selected from the group comprising chemiluminescent label, enzyme label, fluorescence label, radioiodine label.
- the assays can be homogenous or heterogeneous assays, competitive and non-competitive assays.
- the assay is in the form of a sandwich assay, which is a non-competitive immunoassay, wherein the molecule to be detected and/or quantified is bound to a first antibody and to a second antibody.
- the first antibody may be bound to a solid phase, e.g. a bead, a surface of a well or other container, a chip or a strip
- the second antibody is an antibody which is labeled, e.g. with a dye, with a radioisotope, or a reactive or catalytically active moiety.
- the amount of labeled antibody bound to the analyte is then measured by an appropriate method.
- the general composition and procedures involved with “sandwich assays” are well-established and known to the skilled person (The Immunoassay Handbook, Ed. David Wild, Elsevier LTD, Oxford; 3rd ed. (May 2005), ISBN-13: 978-0080445267; Hultschis C et al., Curr Opin Chem Biol. 2006 Feb;10(l):4-10. PMID: 16376134).
- the assay comprises two capture molecules, preferably antibodies which are both present as dispersions in a liquid reaction mixture, wherein a first labelling component is attached to the first capture molecule, wherein said first labelling component is part of a labelling system based on fluorescence- or chemiluminescence-quenching or amplification, and a second labelling component of said marking system is attached to the second capture molecule, so that upon binding of both capture molecules to the analyte a measurable signal is generated that allows for the detection of the formed sandwich complexes in the solution comprising the sample.
- said labeling system comprises rare earth cryptates or rare earth chelates in combination with fluorescence dye or chemiluminescence dye, in particular a dye of the cyanine type.
- fluorescence-based assays comprise the use of dyes, which may for instance be selected from the group comprising FAM (5-or 6-carboxyfluorescein), VIC, NED, Fluorescein, Fluoresceinisothiocyanate (F1TC), 1RD-700/800, Cyanine dyes, such as CY3, CY5, CY3.5, CY5.5, Cy7, Xanthen, 6-Carboxy-2’,4’,7’,4,7-hexachlorofluorescein (HEX), TET, 6-Carboxy- 4 ’ ,5 ’ -dichloro-2 ’ ,7 ’ -dimethodyfluorescein (JOE), N,N,N’ ,N’ -T etramethyl-6-carboxyrhodamine (TAMRA), 6-Carboxy-X-rhodamine (ROX), 5-Carboxyrhodamine-6G (R6G5), 6-carboxyrh
- chemiluminescence based assays comprise the use of dyes, based on the physical principles described for chemiluminescent materials in (Kirk-Othmer, Encyclopedia of chemical technology, 4th ed., executive editor, J. I. Kroschwitz; editor, M. Howe-Grant, John Wiley & Sons, 1993, vol.15, p. 518-562, incorporated herein by reference, including citations on pages 551-562).
- Preferred chemiluminescent dyes are acridiniumesters.
- an “assay” or “diagnostic assay” can be of any type applied in the field of diagnostics. Such an assay may be based on the binding of an analyte to be detected to one or more capture probes with a certain affinity. Concerning the interaction between capture molecules and target molecules or molecules of interest, the affinity constant is preferably greater than 108 M-l.
- Subject matter of the present invention is an inhibitor of the activity of DPP3 for use as therapy or intervention in a critically ill patient with a reduction in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said pre-determined threshold of the level of DPP3 in a sample of bodily fluid of said subject is between 20 and 120 ng/mL, more preferred between 30 and 80 ng/mL, even more preferred between 40 and 60 ng/mL, most preferred said threshold is 50 ng/mL.
- an assay is used for determining the level of DPP3, wherein the assay sensitivity of said assay is able to quantify the DPP3 of healthy subjects and is ⁇ 20 ng/ml, preferably ⁇ 30 ng/ml and more preferably ⁇ 40 ng/ml.
- a bodily fluid according to the present invention is in one particular embodiment a blood sample.
- a blood sample may be selected from the group comprising whole blood, serum and plasma.
- said sample is selected from the group comprising human citrate plasma, heparin plasma and EDTA plasma.
- said level of DPP3 is determined in different samples taken from said patient at different time-points.
- the difference between said level of DPP3 in different samples taken from said patient at different time-points is determined.
- the difference may be determined as absolute or relative difference.
- said level of DPP3 is determined at least twice.
- a therapy is initiated when said relative difference between said level of DPP3 in different samples taken from said patient at different timepoints is 100% or above, more preferred 75% or above, even more preferred 50% or above, most preferred 25% or above.
- said at least second determination of the level of DPP3 is conducted within 2 hours, preferably within 4 hours, more preferred within 6 hours, even more preferred within 12 hours, even more preferred within 24 hours, most preferred within 48 hours.
- the level of DPP3 as amount of DPP3 protein and/ or DPP3 activity in a sample of bodily fluid of said subject may be determined for example by one of the following methods:
- Luminescence immunoassay for the quantification of DPP3 protein concentrations (LIA) (Rehfeld etal., 2019 JALM 3(6): 943-953 ⁇ .
- the LIA is a one-step chemiluminescence sandwich immunoassay that uses white high-binding polystyrene microtiter plates as solid phase. These plates are coated with monoclonal anti-DPP3 antibody AK2555 (capture antibody).
- the tracer anti-DPP3 antibody AK2553 is labeled with MA70- acridinium-NHS-ester and used at a concentration of 20 ng per well.
- samples e.g., serum, heparin-plasma, citrate-plasma or EDTA-plasma derived from patients’ blood
- calibrators are pipetted into coated white microtiter plates. After adding the tracer antibody AK2553, the microtiter plates are incubated for 3 h at room temperature and 600 rpm. Unbound tracer is then removed by 4 washing steps (350 pL per well). Remaining chemiluminescence is measured for Is per well by using a microtiter plate luminometer. The concentration of DPP3 is determined with a 6-point calibration curve. Calibrators and samples are preferably run in duplicate.
- Enzyme capture activity assay for the quantification of DPP3 activity (ECA) (Rehfeld et al., 2019 JALM 3(6): 943-953 ⁇ .
- the ECA is a DPP3-specific activity assay that uses black high-binding polystyrene microtiter plates as solid phase. These plates are coated with monoclonal anti-DPP3 antibody AK2555 (capture antibody). Twenty microliters of samples (e.g., serum, heparin-plasma, citrate-plasma, EDTA-plasma, cerebrospinal fluid and urine) and calibrators are pipetted into coated black microtiter plates. After adding assay buffer (200 pL), the microtiter plates are incubated for 2 h at 22°C and 600 rpm. DPP3 present in the samples is immobilized by binding to the capture antibody. Unbound sample components are removed by 4 washing steps (350 pL per well).
- samples e.g., serum, heparin-plasma, citrate-plasma, EDTA-plasma, cerebrospinal fluid and urine
- calibrators are pipetted into coated black microtiter plates. After adding assay buffer (
- the specific activity of immobilized DPP3 is measured by the addition of the fluorogenic substrate, Arg-Arg-0-Naphthylamide (Arg2-0NA), in reaction buffer followed by incubation at 37 °C for 1 h. DPP3 specifically cleaves Arg2-0NA into Arg- Arg dipeptide and fluorescent 0-naphthylamine. Fluorescence is measured with a fluorometer using an excitation wavelength of 340 nm and emission is detected at 410 nm. The activity of DPP3 is determined with a 6-point calibration curve. Calibrators and samples are preferably run in duplicates.
- LAA DPP3 activity
- samples e.g., serum, heparin-plasma, citrate-plasma
- calibrators are pipetted into non-binding black microtiter plates.
- fluorogenic substrate, Arg2-0NA in assay buffer (200 pL)
- the activity of DPP3 is determined with a 6-point calibration curve. Calibrators and samples are preferably run in duplicates.
- the DPP3 levels of the present invention have been determined with the described DPP3 -assays as outlined in the examples (Rehfeld et al. 2019. JALM 3(6): 943-953).
- the mentioned threshold values above might be different in other assays, if these have been calibrated differently from the assay systems used in the present invention. Therefore, the mentioned cut-off values above shall apply for such differently calibrated assays accordingly, taking into account the differences in calibration.
- One possibility of quantifying the difference in calibration is a method comparison analysis (correlation) of the assay in question with the respective biomarker assay used in the present invention by measuring the respective biomarker (e.g. , DPP3) in samples using both methods.
- Another possibility is to determine with the assay in question, given this test has sufficient analytical sensitivity, the median biomarker level of a representative normal population, compare results with the median biomarker levels as described in the literature and recalculate the calibration based on the difference obtained by this comparison.
- Threshold levels can be obtained for instance from a Kaplan-Meier analysis, where the occurrence of a disease is correlated with the quartiles of the biomarker in the population. According to this analysis, subjects with biomarker levels above the 75th percentile have a significantly increased risk for getting the diseases according to the invention. This result is further supported by Cox regression analysis with full adjustment for classical risk factors: The highest quartile versus all other subjects is highly significantly associated with increased risk for getting a disease according to the invention.
- cut-off values are for instance the 90th, 95th or 99th percentile of a normal population.
- a higher percentile than the 75th percentile one reduces the number of false positive subjects identified, but one might miss to identify subjects, who are at moderate, albeit still increased risk.
- patient refers to a living human or non-human organism that is receiving medical care or that should receive medical care due to a disease. This includes persons with no defined illness who are being investigated for signs of pathology. Thus, the methods and assays described herein are applicable to both, human and veterinary disease.
- Myocardial injury is defined by an elevation of cardiac troponin values above the 99th percentile upper reference limit.
- myocardial injury is a structural injury of myocardial cells and tissue (e.g. cardiomyocytes cardiofibroblasts, smooth muscle cells or endothelial cells). It is considered a prerequisite for the diagnosis of myocardial infarction but also an entity in itself and can arise from non-ischemic or non-cardiac conditions (Thygesen et al. 2018. Fourth Universal Definition of Myocardial Infarction (2016). Eur Heart J. 40(3): 237-69; Chapman et al. 2016. Assessment and Classification of Patients with Myocardial Injury and Infarction in Clinical Practice. Heart 103(1): 10-8).
- myocardial injury might be used in the setting of direct cardiac damage such as cardiac contusion, but it might also occur in diverse other clinical scenarios such as myocardial infarction, myocardial inflammation, sepsis, and iatrogenic injury.
- myocardial injury can have the following causes: primary myocardial ischemia I myocardial infarction (atherosclerotic plaque rupture with thrombosis), mismatch in myocardial oxygen supply and demand (coronary vasospasm, microvascular dysfunction, coronary embolism I microembolism / dissection, sustained bradyarrhythmias/ tachyarrhythmias, hypovolemic shock, respiratory failure / severe anemia, left ventricular hypertrophy / hypertrophic cardiomyopathy, severe hypertension), non-ischemic myocardial injury (heart failure, myocardial inflammation / myocarditis, cardiomyopathies / Tako-tsubo cardiomyopathy, cardiac contusion, iatrogenic (revascularization, cardiac surgery, ablation, pacing, cardioversion, defibrillation), rhabdomyolysis multifactorial and systemic causes (sepsis I critical illness, cardiotoxicity (drugs), infiltrative disease (cardia), cardio
- Presumed mechanisms of myocardial injury include direct cardiac damage with cardiomyocyte injury, myocardial strain as a result of excessive wall stress and myocardial ischemia due to myocardial oxygen supply and demand mismatch.
- Myocardial injury might be irreversible and is often associated with myocardial necrosis or apoptosis (Parket al. 2017. Cardiac Troponins: From Myocardial Infarction to Chronic Disease. Cardiovasc Res. 113 (14): 1708-18).
- blood pressure means mean arterial pressure (MAP), which is the average arterial pressure throughout one cardiac cycle, systole, and diastole.
- MAP is influenced by cardiac output and systemic vascular resistance, each of which is influenced by several variables.
- MAP is a major determinant of the perfusion pressure seen by organs in the body.
- Current guidelines recommend targeting a MAP goal of 65 mm Hg or more in critically ill medical patients (Dellinger et al. 2012.
- Surviving sepsis campaign international guidelines for management of severe sepsis and septic shock. Crit Care Med. 2013:41(2):580-637; Peberdy et al. 2010.
- blood pressure decline is a MAP ⁇ 65 mmHg, more preferred ⁇ 60 mmHg, even more preferred ⁇ 55 mmHg, most preferred ⁇ 50 mmHg.
- said blood pressure decline is a reduction in MAP of at least 5 mmHg, more preferred of at least 10 mmHg, even more preferred of at least 15 mmHg, most preferred of at least 20 mmHg.
- Interleukin-6 is an important inflammatory mediator that is secreted to the circulatory system in response to infections and tissue injuries in the acute phases. IL-6 expression is tightly regulated, with low levels of expression in healthy individuals. Cardiomyocytes produce IL-6 under hypoxic and ischemic stress (Fuchs et al. 2003. FASEB J. 17 (14): 2118-2120). This activates the JAK/STAT cascade in these cells to exert negative inotropic and cytotoxicity.
- the inflammatory reaction mediates neutrophil infiltration and activation, triggering the release of further cytokines into the blood, costimulating vascular endothelium and inducing cardiomyocytes to express ICAM-1 to lead to myocardial fibrosis and ischemia/reperfusion injury (Gwechenberger et al. 1999. Circulation 99 (4): 546-551), which, as a consequence, accelerates myocardial damage and dysfunction (Halawa et al. 1999. Pol. Arch. Med. Wewn 101 (3): 197-203).
- Troponins are structural proteins found in the troponin complex within skeletal and cardiac muscle thin filaments.
- the troponin complex consists of three subunits (I, T, and C) and along with calcium ions plays an important role in the regulation of muscle contraction (Kozinski et al. 2017. Critical Reviews in Clinical Laboratory Sciences 54 (3): 143-172).
- Each molecule has a specific role in the muscle contraction process: troponin T attaches the troponin complex to the actin filament, troponin C acts as the calcium binding site, and troponin I inhibits interaction with myosin heads in the absence of sufficient calcium ions (Garget al. 2017. Internal and Emergency Medicine 12 (2): 147-155).
- Troponin T and I are mainly localised in the myocardium, thus being referred to as cardiac troponin (cTnl and cTnT). It is generally accepted that these biomarkers possess the greatest specificity in identifying myocardial injury (Chaulin 2021. Vascular Health and Risk Management 17: 299-316). Myocardial injury is ascertained if detectable cardiac troponin concentrations are found above the 99th percentile of the upper reference limit (URL) (Thygesen et al. 2019. Eur. Heart J. 40: 237-269).
- URL 99th percentile of the upper reference limit
- Myocardial protection means the prevention of myocardial injury.
- prevention of myocardial injury is defined as a prevention of an increase of cardiac troponins in the circulation.
- prevention of myocardial injury is defined as a prevention of structural injury of myocardial cells and tissue (e.g. cardiomyocytes cardiofibroblasts, smooth muscle cells or endothelial cells) defined as an increase of cardiac troponins in the circulation.
- myocardial injury is characterized by blood levels of cardial troponin above a threshold, increased myocardial expression of pro-inflammatory interleukin-6 (IL-6) and/ or need of vasopressor (to maintain blood pressure and cardiac output).
- IL-6 pro-inflammatory interleukin-6
- Said cardial troponin is selected from the group comprising cardial troponin T (cTnT) and cardial troponin I (cTnl).
- Troponins may be measured with high-sensitive troponin (hs-Tn) assays. Thresholds of cardiac troponin concentrations are for example above the 99th percentile of the upper reference limit (URL) (Thygesen et al. 2019. Eur. Heart J. 40: 237-269).
- the elevation of cardiac troponin values is further defined as rising of cardiac high-sensitive Troponin I (hs-cTnl) or cTnT values with at least one value above the 99th percentile of the upper reference limit.
- Reference limits are sex-dependent (with higher values in men compared to women). Moreover, the reference values depend on the assay used (Sandoval et al. 2022 Circulation 146: 569-581) - see Table 1 below.
- Vasopressors increase vasoconstriction, which leads to increased systemic vascular resistance (SVR). Increasing the SVR leads to increased mean arterial pressure (MAP) and increased perfusion to organs.
- Vasopressors are selected from the group comprising isoproterenol, dobutamine, dopamine, phenylephrine, norepinephrine, epinephrine, vasopressin or terlipressin.
- “Critically ill” means that said patient is suffering from an acute disease or acute condition which is lifethreatening and in which death is possible or imminent.
- said critically ill patient is an ICU patient.
- Said infectious disease may be of bacterial, viral, fungal or parasitic origin.
- Said viral infection may be selected from infection caused by influenza virus or coronavirus.
- Said coronavirus is selected from the group comprising SARS-CoV-1, SARS-CoV-2, MERS-CoV, in particular SARS-CoV-2.
- Coronaviruses cause diseases in mammals and birds. In humans, the viruses cause respiratory infections, including the common cold, which are typically mild, though rarer forms such as SARS, MERS and COVID-19 can be lethal.
- SARS-CoV-1 or -2 infection may present with mild, moderate, or severe illness; the latter includes severe pneumonia, acute respiratory distress syndrome (ARDS), sepsis and septic shock.
- ARDS acute respiratory distress syndrome
- Acute respiratory distress syndrome is a type of respiratory failure characterized by rapid onset of widespread inflammation in the lungs. Symptoms include shortness of breath, rapid breathing, and bluish skin coloration. For those who survive, a decreased quality of life is common. Causes may include sepsis, pancreatitis, trauma, pneumonia, and aspiration.
- the underlying mechanism involves diffuse injury to cells which form the barrier of the microscopic air sacs of the lungs, surfactant dysfunction, activation of the immune system, and dysfunction of the body's regulation of blood clotting. In effect, ARDS impairs the lungs' ability to exchange oxygen and carbon dioxide.
- Diagnosis is based on a PaCh/FiCh ratio (ratio of partial pressure arterial oxygen and fraction of inspired oxygen) of less than 300 mm Hg despite a positive end-expiratory pressure (PEEP) of more than 5 cm H2O.
- the primary treatment involves mechanical ventilation together with treatments directed at the underlying cause. Ventilation strategies include using low volumes and low pressures. If oxygenation remains insufficient, lung recruitment maneuvers and neuromuscular blockers may be used. If this is insufficient, extracorporeal membrane oxygenation (ECMO) may be an option.
- the syndrome is associated with a death rate between 35 and 50%.
- Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection (see Singer et al. 2016. JAMA 315(8): 801-810). Organ dysfunction can be identified as an acute change in total SOFA score >2 points consequent to the infection. The baseline SOFA score can be assumed to be zero in patients not known to have preexisting organ dysfunction. A SOFA score >2 reflects an overall mortality risk of approximately 10% in a general hospital population with suspected infection. Even patients presenting with modest dysfunction can deteriorate further, emphasizing the seriousness of this condition and the need for prompt and appropriate intervention, if not already being instituted. Sepsis is a life-threatening condition that arises when the body’s response to an infection injures its own tissues and organs.
- Shock is characterized by decreased oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization leading to cellular and tissue hypoxia. It is a life-threatening condition of circulatory failure and most commonly manifested as hypotension (systolic blood pressure less than 90 mm Hg or MAP less than 65 mmHg). Shock is divided into four main types based on the underlying cause: hypovolemic, cardiogenic, obstructive, and distributive shock (Vincent and De Backer 2014. N. Engl. J. Med. 370(6): 583).
- Septic shock is a potentially fatal medical condition that occurs when sepsis, which is organ injury or damage in response to infection, leads to dangerously low blood pressure and abnormalities in cellular metabolism.
- the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) defines septic shock as a subset of sepsis in which particularly profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone.
- Patients with septic shock can be clinically identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and serum lactate level greater than 2 mmol/L (>18 mg/dL) in the absence of hypovolemia.
- the primary infection is most commonly caused by bacteria, but also may be by fungi, viruses or parasites. It may be located in any part of the body, but most commonly in the lungs, brain, urinary tract, skin or abdominal organs. It can cause multiple organ dysfunction syndrome (formerly known as multiple organ failure) and death. Frequently, people with septic shock are cared for in intensive care units. It most commonly affects children, immunocompromised individuals, and the elderly, as their immune systems cannot deal with infection as effectively as those of healthy adults. The mortality rate from septic shock is approximately 25-50%.
- Cardiogenic shock is defined as a state of critical endorgan hypoperfusion due to reduced cardiac output. Notably, CS forms a spectrum that ranges from mild hypoperfusion to profound shock.
- Established criteria for the diagnosis of CS are: (i) systolic blood pressure, ⁇ 90 mmHg for >30 min or vasopressors required to achieve a blood pressure >90 mmHg; (ii) pulmonary congestion or elevated left- ventricular filling pressures; (iii) signs of impaired organ perfusion with at least one of the following criteria: (a) altered mental status; (b) cold, clammy skin; (c) oliguria ( ⁇ 0.5 mL/kg/h or ⁇ 30 mL/h); (d) increased serum-lactate (Reynolds and Hochman 2008.
- Acute myocardial infarction (AMI) with subsequent ventricular dysfunction is the most frequent cause of CS accounting for approximately 80% of cases. Mechanical complications such as ventricular septal (4%) or free wall rupture (2%), and acute severe mitral regurgitation (7%) are less frequent causes of CS after AML (Hochman et al. 2000. J Am Coll Cardiol 36: 1063-1070).
- Non-AMI-related CS may be caused by decompensated valvular heart disease, acute myocarditis, arrhythmias, etc. with heterogeneous treatment options. This translates in 40 000 to 50 000 patients per year in the USA and 60000 to 70 000 in Europe.
- Acute coronary syndrome refers to a group of diseases in which blood flow to the heart is decreased and includes ST-elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), and unstable angina. It is a type of coronary heart disease (CHD), which is responsible for one-third of total deaths in people older than 35 years of age. Some forms of CHD can be asymptomatic, but ACS is always symptomatic.
- acute myocardial infarction is defined as follows:
- the term acute myocardial infarction should be used when there is acute myocardial injury with clinical evidence of acute myocardial ischaemia and with detection of a rise and/or fall of cardiac troponin (cTn) values with at least one value above the 99th percentile upper reference level (URL) and at least one of symptoms of myocardial ischaemia, new ischaemic ECG changes, development of pathological Q waves, imaging evidence of new loss of viable myocardium or new regional wall motion abnormality in a pattern consistent with an ischaemic aetiology or identification of a coronary thrombus by angiography or autopsy (Thygesen et al. 2018.
- PCI percutaneous coronary intervention
- CABG coronary artery bypass grafting
- Inhibitors are molecules that preferably significantly inhibit DPP3 activity. Those molecules can be peptides and small molecules, antibodies, antibody fragments or non-Ig scaffolds.
- Significantly inhibiting means inhibiting the activity of DPP3 more than 60%, preferably more than 70%, more preferably more than 80 %, preferably more than 90 %, more preferably almost or actually 100% inhibition.
- DPP3 can be inhibited unspecifically by different general protease inhibitors (e.g., PMSF, TPCK), sulfhydryl reagents (e.g., pHMB, DTNB) and metal chelators (EDTA, o-phenantroline) (Abramic et al. 2000. Biological Chemistry, 381: 1233-1243; EP 2949332).
- general protease inhibitors e.g., PMSF, TPCK
- sulfhydryl reagents e.g., pHMB, DTNB
- EDTA metal chelators
- DPP3 activity can be further inhibited specifically by different kinds of compounds: an endogenous DPP3 -inhibitor is the peptide spinorphin.
- a synthetic derivatives of spinorphin e.g., tynorphin
- Other published peptide inhibitors of DPP3 are propioxatin A and B (US 4804676) and propioxatin A analogues (Inaoka et al. 1988. J. Biochem 104 (5): 706-711).
- a derivative or analogue 44 is a chemical compound that is derived from a parent compound by a chemical reaction with the replacement of one atom or substitution of a group of atoms by a functional group. Parent and derivative compounds have similar chemical structures.
- DPP3 can also be inhibited by small molecules such as fluostatins and benzimidazol derivatives.
- Fluostatins A and B are antibiotics produced in Streptomyces sp. TA-3391 that are non-toxic and strongly inhibit DPP3 activity. So far, 20 different derivatives of benzimidazol have been synthesized and published Chimica Slovenica 62: 867-878), of which the two compounds 1 ’ and 4’ show the strongest inhibitory effect (Agic et al. 2007. Bioorganic Chemistry 35 (2): 153-169). Several dipeptidyl hydroxamic acids have been shown to inhibit DPP3 activity as well (Cvitesic et al., 2016. J Enzyme Inhib Med Chem 31(sup2):40-45).
- a “small molecule” is in particular a low molecular weight (more particularly ⁇ 1000 daltons) organic compound. Such small molecules may in particular regulate a biological process, e.g. bind a specific biological macromolecule, in the present invention in particular DPP3, and act as an effector, in particular an inhibitor, altering the activity or function of the biological macromolecule. Small molecules can be of natural origin or artificial.
- Subject-mater of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein the inhibitor of the activity of DPP3 is selected from the group comprising small molecules, anti-DPP3 antibody, anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold.
- Subject mater of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein the inhibitor of the activity of DPP3 is a small molecule selected from the group comprising spinorphin, tynorphin, propioxatin A and B, fluostatin A and B, enzimidazole or derivatives or analogues thereof.
- Subject mater of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said inhibitor is an anti-DPP3 antibody, anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that exhibits a minimum binding affinity to DPP3 of equal or less than 10' 7 M.
- Subject mater of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said antibody is a monoclonal antibody or monoclonal antibody fragment.
- antibody generally comprises monoclonal and polyclonal antibodies and binding fragments thereof, in particular Fc-fragments as well as so called “single-chain-antibodies” (Bird et al. 1988), chimeric, humanized, in particular CDR-grafted antibodies, and dia or tetrabodies (Holliser et al. 1993).
- immunoglobulin-like proteins that are selected through techniques including, for example, phage display to specifically bind to the molecule of interest contained in a sample.
- specific binding refers to antibodies raised against the molecule of interest or a fragment thereof.
- An antibody is considered to be specific, if its affinity towards the molecule of interest or the aforementioned fragment thereof is at least preferably 50-fold higher, more preferably 100-fold higher, most preferably at least 1000-fold higher than towards other molecules comprised in a sample containing the molecule of interest. It is well known in the art how to make antibodies and to select antibodies with a given specificity.
- the anti-DPP3 antibody or anti-DPP3 antibody fragment or anti- DPP3 non-Ig scaffold is monospecific.
- Monospecific anti-DPP3 antibody or monospecific anti-DPP3 antibody fragment or monospecific anti- DPP3 non-Ig scaffold means that said antibody or antibody fragment or non-Ig scaffold binds to one specific region encompassing at least 5 amino acids within the target DPP3 (SEQ ID No. 1).
- Monospecific anti-DPP3 antibody or monospecific anti-DPP3 antibody fragment or monospecific anti- DPP3 non-Ig scaffold are anti-DPP3 antibodies or anti-DPP3 antibody fragments or anti-DPP3 non-Ig scaffolds that all have affinity for the same antigen.
- Monoclonal antibodies are monospecific, but monospecific antibodies may also be produced by other means than producing them from a common germ cell.
- said anti-DPP3 antibody, anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold is an inhibiting antibody, fragment or non-Ig scaffold.
- Said anti-DPP3 antibody, anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold is inhibiting the activity of DPP3 more than 50%, preferably more than 60%, preferably more than 70%, more preferably more than 80 %, preferably more than 90 %, even more preferred more than 95%, preferably almost or actually 100%.
- An antibody or fragment according to the present invention is a protein including one or more polypeptides substantially encoded by immunoglobulin genes that specifically binds an antigen.
- the recognized immunoglobulin genes include the kappa, lambda, alpha (IgA), gamma (IgGi, IgGz, IgGs, IgG 4 ), delta (IgD), epsilon (IgE) and mu (IgM) constant region genes, as well as the myriad immunoglobulin variable region genes.
- Full-length immunoglobulin light chains are generally about 25 Kd or 214 amino acids in length.
- Full-length immunoglobulin heavy chains are generally about 50 Kd or 446 amino acids in length.
- Light chains are encoded by a variable region gene at the NH2- terminus (about 110 amino acids in length) and a kappa or lambda constant region gene at the COOH-terminus.
- Heavy chains are similarly encoded by a variable region gene (about 116 amino acids in length) and one of the other constant region genes.
- the basic structural unit of an antibody is generally a tetramer that consists of two identical pairs of immunoglobulin chains, each pair having one light and one heavy chain. In each pair, the light and heavy chain variable regions bind to an antigen, and the constant regions mediate effector functions.
- Immunoglobulins also exist in a variety of other forms including, for example, Fv, Fab, and (Fab')2, as well as bifunctional hybrid antibodies and single chains (e.g. , Lanzavecchia etal. 1987. Eur. J. Immunol. 1 7: 105; Huston et al. 1988. Proc. Natl. Acad. Sci. U.S.A., 8 5: 5879-5883; Bird et al. 1988.
- An immunoglobulin light or heavy chain variable region includes a framework region interrupted by three hypervariable regions, also called complementarity determining regions (CDR's) (see, Sequences of Proteins of Immunological Interest, E. Kabat et al. 1983, U.S. Department of Health and Human Services' ⁇ . As noted above, the CDRs are primarily responsible for binding to an epitope of an antigen.
- An immune complex is an antibody, such as a monoclonal antibody, chimeric antibody, humanized antibody or human antibody, or functional antibody fragment, specifically bound to the antigen.
- Chimeric antibodies are antibodies whose light and heavy chain genes have been constructed, typically by genetic engineering, from immunoglobulin variable and constant region genes belonging to different species.
- the variable segments of the genes from a mouse monoclonal antibody can be joined to human constant segments, such as kappa and gamma 1 or gamma 3.
- a therapeutic chimeric antibody is thus a hybrid protein composed of the variable or antigen-binding domain from a mouse antibody and the constant or effector domain from a human antibody, although other mammalian species can be used, or the variable region can be produced by molecular techniques. Methods of making chimeric antibodies are well known in the art, e.g., see U.S. Patent No. 5,807,715.
- a “humanized” immunoglobulin is an immunoglobulin including a human framework region and one or more CDRs from a non-human (such as a mouse, rat, or synthetic) immunoglobulin.
- the non-human immunoglobulin providing the CDRs is termed a "donor” and the human immunoglobulin providing the framework is termed an "acceptor".
- all the CDRs are from the donor immunoglobulin in a humanized immunoglobulin.
- Constant regions need not be present, but if they are, they must be substantially identical to human immunoglobulin constant regions, i.e., at least about 85- 90%, such as about 95% or more identical.
- a humanized antibody is an antibody comprising a humanized light chain and a humanized heavy chain immunoglobulin.
- a humanized antibody binds to the same antigen as the donor antibody that provides the CDR’s.
- the acceptor framework of a humanized immunoglobulin or antibody may have a limited number of substitutions by amino acids taken from the donor framework. Humanized or other monoclonal antibodies can have additional conservative amino acid substitutions, which have substantially no effect on antigen binding or other immunoglobulin functions.
- Humanized immunoglobulins can be constructed by means of genetic engineering (e.g., see U.S. Patent No. 5,585,089).
- a human antibody is an antibody wherein the light and heavy chain genes are of human origin. Human antibodies can be generated using methods known in the art. Human antibodies can be produced by immortalizing a human B cell secreting the antibody of interest.
- Immortalization can be accomplished, for example, by EBV infection or by fusing a human B cell with a myeloma or hybridoma cell to produce a trioma cell.
- Human antibodies can also be produced by phage display methods (see, e.g., WO91/17271; WQ92/001047; WO92/2Q791Y or selected from a human combinatorial monoclonal antibody library (see the Morphosys website). Human antibodies can also be prepared by using transgenic animals carrying a human immunoglobulin gene (for example, see WO93/12227; WO 91/10741 ⁇ .
- the anti-DPP3 antibody may have the formats known in the art.
- examples are human antibodies, monoclonal antibodies, humanized antibodies, chimeric antibodies, CDR-grafted antibodies.
- antibodies according to the present invention are recombinantly produced antibodies as e.g. IgG, a typical full-length immunoglobulin, or antibody fragments containing at least the F-variable domain of heavy and/or light chain as e.g. chemically coupled antibodies (fragment antigen binding) including but not limited to Fab-fragments including Fab minibodies, single chain Fab antibody, monovalent Fab antibody with epitope tags, e.g.
- bivalent Fab-V5Sx2 bivalent Fab (mini-antibody) dimerized with the CH3 domain
- bivalent Fab or multivalent Fab e.g. formed via multimerization with the aid of a heterologous domain, e.g. via dimerization of dHLX domains, e.g. Fab-dHLX-FSx2; F(ab‘)2-fragments, scFv-fragments, multimerized multivalent or/and multi-specific scFv-fragments, bivalent and/or bispecific diabodies, BITE® (bispecific T-cell engager), trifunctional antibodies, polyvalent antibodies, e.g. from a different class than G; single-domain antibodies, e.g. nanobodies derived from camelid or fish immunoglobulins and numerous others.
- the anti-DPP3 antibody format is selected from the group comprising Fv fragment, scFv fragment, Fab fragment, scFab fragment, F(ab) fragment and scFv-Fc Fusion protein.
- the antibody format is selected from the group comprising scFab fragment, Fab fragment, scFv fragment and bioavailability optimized conjugates thereof, such as PEGylated fragments.
- One of the most preferred formats is the scFab format.
- Non-Ig scaffolds may be protein scaffolds and may be used as antibody mimics as they are capable to bind to ligands or antigens.
- non-Ig scaffolds may be selected from the group comprising tetranectin-based non-Ig scaffolds (e.g. described in US 2010/0028995), fibronectin scaffolds (e.g. described in EP 1266025', lipocalin-based scaffolds (e.g. described in WO 2011/154420)', ubiquitin scaffolds (e.g. described in WO 2011/073214), transferrin scaffolds (e.g. described in US 2004/0023334), protein A scaffolds (e.g. described in EP 2 231 860), ankyrin repeat based scaffolds (e.g.
- microproteins preferably microproteins forming a cysteine knot
- microproteins preferably microproteins forming a cysteine knot
- Fyn SH3 domain based scaffolds e.g. described in WO 2011/023685
- EGFR-A-domain based scaffolds e.g. described in WO 2005/040229
- Kunitz domain based scaffolds e.g. described in EP 1 941 867.
- anti-DPP3 antibodies according to the present invention may be produced as outlined in Example 1 by synthesizing fragments of DPP3 as antigens or frill-length DPP3. Thereafter, binder to said fragments are identified using the below described methods or other methods as known in the art.
- Humanization of murine antibodies may be conducted according to the following procedure:
- the antibody sequence is analyzed for the structural interaction of framework regions (FR) with the complementary determining regions (CDR) and the antigen. Based on structural modelling an appropriate FR of human origin is selected and the murine CDR sequences are transplanted into the human FR. Variations in the amino acid sequence of the CDRs or FRs may be introduced to regain structural interactions, which were abolished by the species switch for the FR sequences. This recovery of structural interactions may be achieved by random approach using phage display libraries or via directed approach guided by molecular modelling (Almagro and Fransson 2008. Humanization of antibodies. Front Biosci. 2008 Jan 1:13:1619-33).
- the anti-DPP3 antibody, anti-DPP3 antibody fragment, or anti-DPP3 non-Ig scaffold is a full-length antibody, antibody fragment, or non-Ig scaffold.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein the complementarity determining regions (CDR's) in the heavy chain comprises the sequences:
- SEQ ID NO.: 7, SEQ ID NO.: 8 and/ or SEQ ID NO.: 9 and the complementarity determining regions (CDR's) in the light chain comprises the sequences: SEQ ID NO.: 10, KVS and/or SEQ ID NO.: 11.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said monoclonal antibody or antibody fragment is a humanized monoclonal antibody or humanized monoclonal antibody fragment.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein the heavy chain comprises the sequence: SEQ ID NO.: 12 and wherein the light chain comprises the sequence: SEQ ID NO.: 13.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for cardiac protection and/ or prevention of cardiac damage, wherein said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID No. 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 amino acids in length comprised in SEQ ID No. 1.
- said inhibitor is an anti-DPP3 antibody or anti- DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 5 amino acids in length comprised in SEQ ID No. 1.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID NO.: 2, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 amino acids in length comprised in SEQ ID NO.: 2, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non- Ig scaffold that binds an epitope of at least 5 amino acids in length comprised in SEQ ID NO.: 2, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID NO.: 3, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 amino acids in length comprised in SEQ ID NO.: 3, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non- Ig scaffold that binds an epitope of at least 5 amino acids in length comprised in SEQ ID NO.: 3, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- Subject matter of the present application is an inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID NO.: 4, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 amino acids in length comprised in SEQ ID NO.: 4, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non- Ig scaffold that binds an epitope of at least 5 amino acids in length comprised in SEQ ID NO.: 4, and wherein the epitope is comprised in DPP3 as depicted in SEQ ID NO.: 1.
- An epitope also known as antigenic determinant, is the part of an antigen that is recognized by the immune system, specifically by antibodies.
- the epitope is the specific piece of the antigen to which an antibody binds.
- the part of an antibody that binds to the epitope is called a paratope.
- the epitopes of protein antigens are divided into two categories, conformational epitopes and linear epitopes, based on their structure and interaction with the paratope. Conformational and linear epitopes interact with the paratope based on the 3-D conformation adopted by the epitope, which is determined by the surface features of the involved epitope residues and the shape or tertiary structure of other segments of the antigen.
- a conformational epitope is formed by the 3-D conformation adopted by the interaction of discontiguous amino acid residues.
- a linear or a sequential epitope is an epitope that is recognized by antibodies by its linear sequence of amino acids, or primary structure and is formed by the 3-D conformation adopted by the interaction of contiguous amino acid residues.
- the antibody is a monoclonal antibody or a fragment thereof.
- the anti-DPP3 antibody or the anti-DPP3 antibody fragment is a human or humanized antibody or derived therefrom.
- one or more (murine) CDR’s are grafted into a human antibody or antibody fragment.
- Subject mater of the present invention in one aspect is a human or humanized CDR-grafted antibody or antibody fragment thereof that binds to DPP3, wherein the human or humanized CDR-grafted antibody or antibody fragment thereof comprises an antibody heavy chain (H chain) comprising:
- ARNYSYDY (SEQ ID No.: 9) and/or further comprises an antibody light chain (L chain) comprising:
- subject mater of the present invention is a human or humanized monoclonal antibody that binds to DPP3 or an antibody fragment thereof that binds to DPP3 wherein the heavy chain comprises at least one CDR selected from the group comprising:
- ARNYSYDY (SEQ ID No.: 9) and wherein the light chain comprises at least one CDR selected from the group comprising: RSLVHSIGSTY (SEQ ID No.: 10), KVS (not part of the sequencing listing), SQSTHVPWT (SEQ ID No.: 11).
- the anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold according to the present invention exhibits an affinity towards human DPP3 in such that affinity constant is greater than IO’ 7 M, preferred 10' 8 M, preferred affinity is greater than 10' 9 M, most preferred higher than IO 10 M.
- affinity constants may be determined according to the method as described in Example 1.
- Subject mater of the present invention is a monoclonal antibody or fragment that binds to DPP3 or an antibody fragment for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said antibody or fragment comprises the following sequence as a variable heavy chain:
- Subject matter of the present invention is a human or humanized monoclonal antibody or fragment that binds to DPP3 or an antibody fragment thereof for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury, wherein said antibody or fragment comprises the following sequence as a heavy chain:
- the antibody comprises the following sequence as a heavy chain: SEQ ID NO: 12 or a sequence that is > 95% identical to it, preferably > 98%, preferably > 99% and comprises the following sequence as a light chain: SEQ ID NO: 13 or a sequence that is > 95% identical to it, preferably > 98%, preferably > 99%.
- Identity defines the percentage of amino acids with a direct match in the alignment.
- the treatment with an inhibitor of DPP3 activity is initiated or changed immediately upon provision of the result of the sample analysis indicating the level of DPP3 in the sample.
- the treatment may be initiated within 12 hours, preferably 6, 4, 2, 1, 0.5, 0.25 hours or immediately after receiving the result of the sample analysis.
- the method comprises or consists of a single and/ or multiple measurement of DPP3 in a sample from a patient in a single sample and/or multiple samples obtained at essentially the same time point, in order to guide and/ or monitor and/ or stratify a therapy, wherein said therapy is the administration of an inhibitor of the activity of DPP3.
- pharmaceutical formulation means a pharmaceutical ingredient in combination with at least one pharmaceutically acceptable excipient, which is in such form as to permit the biological activity of a pharmaceutical ingredient contained therein to be effective, and which contains no additional components which are unacceptably toxic to a subject to which the formulation would be administered.
- pharmaceutical ingredient means a therapeutic composition which can be optionally combined with pharmaceutically acceptable excipients to provide a pharmaceutical formulation or dosage form.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury comprising an antibody or fragment or scaffold according to the present invention.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury according to the present invention, wherein said pharmaceutical formulation is a solution, preferably a ready-to-use solution.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury according to the present invention, wherein said pharmaceutical formulation is in a freeze-dried state.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury according to the present invention, wherein said pharmaceutical formulation is administered intra-muscular.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury according to the present invention, wherein said pharmaceutical formulation is administered intra-vascular.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury according to the present invention, wherein said pharmaceutical formulation is administered via infusion.
- Subj ect matter of the present invention is a pharmaceutical formulation for use in therapy or intervention in a critically ill patient with a decline in blood pressure for myocardial protection and/ or prevention of myocardial injury according to the present invention, wherein said pharmaceutical formulation is to be administered systemically.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure for myocardial protection and/ or prevention of myocardial injury.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to embodiment 1, wherein said decline of blood pressure is a mean arterial pressure (MAP) of ⁇ 65 mmHg, more preferred ⁇ 60 mmHg, even more preferred ⁇ 55 mmHg, most preferred ⁇ 50 mmHg.
- MAP mean arterial pressure
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to embodiment 1 and 2, wherein said patient is having a level of DPP3 in a sample of bodily fluid of said patient above a (predetermined) threshold.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to embodiment 3, wherein said predetermined threshold of the level of DPP3 in a sample of bodily fluid of said subject is between 20 and 120 ng/mL, more preferred between 30 and 80 ng/mL, even more preferred between 40 and 60 ng/mL, most preferred said threshold is 50 ng/mL.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 1 to 4, wherein said sample is a bodily fluid sample selected from the group comprising whole blood, plasma or serum.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 1 to 5, wherein said myocardial injury is characterized by blood levels of cardiac troponin (cTn) above a threshold, increased myocardial expression of pro-inflammatory interleukin-6 (IL-6), and/ or need of vasopressors to maintain blood pressure and cardiac output.
- cTn cardiac troponin
- IL-6 pro-inflammatory interleukin-6
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 1-7, wherein said patient suffering severe infectious diseases, sepsis, pulmonary embolism, pulmonary hypertension, acute coronary syndrome (including unstable angina pectoris, ST-elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI)), any type of shock (including cardiogenic shock, septic shock or anaphylactic shock), cardiac arrest, acute liver failure and acute respiratory distress syndrome (ARDS).
- severe infectious diseases, sepsis, pulmonary embolism, pulmonary hypertension, acute coronary syndrome including unstable angina pectoris, ST-elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI)
- any type of shock including cardiogenic shock, septic shock or anaphylactic shock
- cardiac arrest acute liver failure and acute respiratory distress syndrome (ARDS).
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 1-8, wherein the inhibitor of the activity of DPP3 is selected from the group comprising small molecules, anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to embodiment 9, wherein said inhibitor is an anti- DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID No. 1.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to embodiment 9 and 10, wherein said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID No. 2.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to any of embodiments 9 to 11 , wherein said antibody is a monoclonal antibody or monoclonal antibody fragment.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to any of embodiments 9 to 12, wherein said antibody or antibody fragment comprises an antibody heavy chain and an antibody light chain, wherein the complementarity determining regions (CDR's) in the heavy chain comprises the sequences: SEQ ID NO.: 7, SEQ ID NO.: 8 and/ or SEQ ID NO.: 9 and the complementarity determining regions (CDR's) in the light chain comprises the sequences:
- SEQ ID NO.: 10 KVS and/or SEQ ID NO.: 11.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to any of embodiments 9 to 13, wherein said monoclonal antibody or antibody fragment is a humanized monoclonal antibody or humanized monoclonal antibody fragment.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to any of embodiments 9 to 14, wherein said antibody or antibody fragment comprises an antibody heavy chain and an antibody light chain, wherein the heavy chain comprises the sequence: SEQ ID NO.: 12 and wherein the light chain comprises the sequence: SEQ ID NO.: 13.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline in pulmonary function according to embodiment 9, wherein said small molecule is selected from the group comprising spinorphin, tynorphin, propioxatin A and B, fluostatin A and B, benzimidazol or derivatives or analogues thereof.
- embodiments 10a to 16a correspond to the above embodiments 10 to 16, wherein the correct reference to embodiment 9, reading “decline of blood pressure”, is included.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to embodiment 9, wherein said inhibitor is an anti- DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID No. 1.
- I la Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to embodiment 9 and 10, wherein said inhibitor is an anti-DPP3 antibody or anti-DPP3 antibody fragment or anti-DPP3 non-Ig scaffold that binds an epitope of at least 4 or 5 amino acids in length comprised in SEQ ID No. 2. 12a. Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 9 to 11, wherein said antibody is a monoclonal antibody or monoclonal antibody fragment.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 9 to 12, wherein said antibody or antibody fragment comprises an antibody heavy chain and an antibody light chain, wherein the complementarity determining regions (CDR's) in the heavy chain comprises the sequences:
- SEQ ID NO.: 7, SEQ ID NO.: 8 and/ or SEQ ID NO.: 9 and the complementarity determining regions (CDR's) in the light chain comprises the sequences:
- SEQ ID NO.: 10 KVS and/or SEQ ID NO.: 11.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 9 to 13, wherein said monoclonal antibody or antibody fragment is a humanized monoclonal antibody or humanized monoclonal antibody fragment.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of embodiments 9 to 14, wherein said antibody or antibody fragment comprises an antibody heavy chain and an antibody light chain, wherein the heavy chain comprises the sequence: SEQ ID NO.: 12 and wherein the light chain comprises the sequence: SEQ ID NO.: 13.
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to embodiment 9, wherein said small molecule is selected from the group comprising spinorphin, tynorphin, propioxatin A and B, fluostatin A and B, benzimidazol or derivatives or analogues thereof.
- myocardial injury is an elevation of cardiac troponin values above the 99th percentile upper reference limit, wherein more particularly myocardial injury is a structural injury of myocardial cells and tissue (e.g. cardiomyocytes cardiofibroblasts, smooth muscle cells or endothelial cells). 18.
- myocardial injury is an elevation of cardiac troponin values above the 99th percentile upper reference limit, wherein more particularly myocardial injury is a structural injury of myocardial cells and tissue (e.g. cardiomyocytes cardiofibroblasts, smooth muscle cells or endothelial cells).
- Inhibitor of the activity of DPP3 for use in therapy or intervention in a critically ill patient with a decline of blood pressure according to any of the preceding embodiments, wherein the blood level of cTn and/or myocardial expression of IL-6 as determined in a sample obtained from said patient is elevated, in particular above a threshold, more particularly cTn is elevated above a threshold as defined in embodiment 17.
- Figure 1 Kaplan Meyer survival plots in relation to low ( ⁇ 68.6 ng/mL) and high (> 68.6 ng/ml) DPP3 plasma concentrations
- A 7-Day survival of patients with sepsis/septic shock in relation to DPP3 plasma concentration (cut-off 68.6 ng/mL);
- B 7-Day survival of patients with cardiogenic shock in relation to DPP3 plasma concentration (cut-off 68.6 ng/mL);
- C 7-day survival of patients with acute myocardial infarction in relation to DPP3 plasma concentration (cut-off 68.6 ng/mL);
- D 3-month survival of patients with dyspnea in relation to DPP3 plasma concentration;
- E 4-week survival of burned patients in relation to DPP3 plasma concentration.
- F 7-Day survival of patients with septic shock in relation to DPP3 plasma concentration
- Figure 2 SDS-PAGE on a gradient gel (4-20%) of native hDPP3 purified from human erythrocyte lysate. Molecular weight marker is indicated as arrows.
- Figure 3 Experimental design - Effect of native DPP3 in an animal model.
- FIG. 4 (A) DPP3 injection causes shortening fraction reduction and therefore leads to deteriorating heart function. (B) Decreased kidney function is also observed via increased renal resistive index.
- Figure 5 Association and dissociation curve of the AK1967-DPP3 binding analysis using Octet.
- AK1967 loaded biosensors were dipped into a dilution series of recombinant GST-tagged human DPP3 (100, 33.3, 11.1, 3.7 nM) and association and dissociation monitored.
- Figure 6 Western Blot of dilutions of blood cell lysate and detection of DPP3 with AK1967 as primary antibody.
- Figure 7 Inhibition curve of native DPP3 from blood cells with inhibitory antibody AK1967. Inhibition of DPP3 by a specific antibody is concentration dependent, with an IC50 at ⁇ 15 ng/ml when analyzed against 15 ng/ml DPP3.
- Figure 8 Experimental setup - Effect of Procizumab in sepsis-induced heart failure.
- Procizumab drastically improves shortening fraction (A) and mortality rate (B) in sepsis- induced heart failure rats.
- Figure 10 Experimental design - Isoproterenol-induced cardiac stress in mice followed by Procizumab treatment (B) and control (A).
- FIG 11 Procizumab improved shortening fraction (A) and reduced the renal resistive index (B) within 1 hour and 6 hours after administration, respectively, in isoproterenol-induced heart failure mice.
- Figure 13 High cDPP3 plasma levels correlate with organ dysfunction in septic patients. Barplots of SOFA score in AdrenOSS-1 according to the evolution of DPP3 levels during ICU stay. HH: DPP3 above median on admission and at 24h; HL: above median on admission but below median at 24h; LL: below median on admission and at 24h; LH: below median on admission but above median at 24h.
- Figure 14 High concentrations of cDPP3 levels 24 hours after admission of septic patients were associated with worst SOFA scores by organ.
- A cardiac,
- B renal,
- C respiratory,
- D liver,
- E coagulation and
- F central nervous system SOFA scores values according to dynamics levels of cDPP3 between admission and 24h (HH: High/High, HL: High/Low, LH: Low/High, LL: Low/Low).
- Figure 15 High levels of DPP3 at admission to the ICU are associated with worsening kidney function in the following 48h.
- Y axis DPP3 measured at day 1 (ICU admission).
- FIG. 16 Serial measurements of DPP3 during ICU are associated with disease severity in COVID- 19 patients.
- FIG. 17 High DPP3 values during ICU stay are associated with poor outcome in COVID-19 patients.
- DPP3 levels were measured at day 3 of ICU admission and for B, at day 7 of ICU admission.
- Y axis DPP3 measured at day 1 (ICU admission).
- X axis non: no vasopressor treatment or any: vasopressor treatment during ICU stay.
- FIG. 19 Serial measurements of DPP3 during ICU are associated with need of organ support therapy, in particular veno-venous ECMO.
- FIG. 20 Treatment scheme of Procizumab for cardiac protection during septic shock
- Norepinephrine requirement was assessed based on the norepinephrine infusion dose (jig/kg/min) at each timepoint from start of resucittion (Hl) to sacrifice (Hl 2) titrated to maintain mean arterial pressure (MAP) between 65 and 75 mmHg.
- Norepinephrine requirement to achieve target MAP was significantly higher in the standard of care arm in comparison to the Procizumab group (p ⁇ 0.05 from H4 to H9 and p ⁇ 0.005 from H10 to H12).
- FIG. 25 Cardiac output, assessed via a pulmonary artery catheter, was significantly different (p ⁇ 0.05) in timepoints H4, H8 and H12 between the standard of care and Procizumab groups.
- Example 1 Methods for the measurement of DPP 3 protein and DPP3 activity
- DPP3 peptides for immunization were synthesized, see Table 3, (JPT Technologies, Berlin, Germany) with an additional N-terminal cystein (if no cystein is present within the selected DPP3 -sequence) residue for conjugation of the peptides to Bovine Serum Albumin (BSA).
- BSA Bovine Serum Albumin
- the peptides were covalently linked to BSA by using Sulfolink-coupling gel (Perbio-science, Bonn, Germany). The coupling procedure was performed according to the manual of Perbio. Recombinant GST-hDPP3 was produced by USBio (United States Biological, Salem, MA, USA).
- mice were intraperitoneally (i.p.) injected with 84 pg GST-hDPP3 or 100 pg DPP3-peptide-BSA-conjugates at day 0 (emulsified in TiterMax Gold Adjuvant), 84 pg or 100 pg at day 14 (emulsified in complete Freund’s adjuvant) and 42 pg or 50 pg at day 21 and 28 (in incomplete Freund’s adjuvant).
- the animal received an intravenous (i.v.) injection of 42 pg GST-hDPP3 or 50 pg DPP3-peptide-BSA-conjugates dissolved in saline. Three days later the mice were sacrificed, and the immune cell fusion was performed.
- Splenocytes from the immunized mice and cells of the myeloma cell line SP2/0 were fused with 1 ml 50% polyethylene glycol for 30 s at 37°C. After washing, the cells were seeded in 96-well cell culture plates. Hybrid clones were selected by growing in HAT medium [RPMI 1640 culture medium supplemented with 20% fetal calf serum and HAT-Supplement]. After one week, the HAT medium was replaced with HT Medium for three passages followed by returning to the normal cell culture medium.
- the cell culture supernatants were primarily screened for recombinant DPP3 binding IgG antibodies two weeks after fusion. Therefore, recombinant GST-tagged hDPP3 (USBiologicals, Salem, USA) was immobilized in 96-well plates (100 ng/ well) and incubated with 50 pl cell culture supernatant per well for 2 hours at room temperature. After washing of the plate, 50 pl / well POD-rabbit anti mouse IgG was added and incubated for 1 h at RT.
- a chromogen solution (3,7 mM o-phenylen-diamine in citrate/ hydrogen phosphate buffer, 0.012% H2O2) were added to each well, incubated for 15 minutes at RT and the chromogenic reaction stopped by the addition of 50 pl 4N sulfuric acid. Absorption was detected at 490 mm.
- the positive tested microcultures were transferred into 24-well plates for propagation. After retesting the selected cultures were cloned and re-cloned using the limiting-dilution technique and the isotypes were determined.
- Antibodies raised against GST-tagged human DPP3 or DPP3 -peptides were produced via standard antibody production methods (.Marx et al. 1997 ⁇ and purified via Protein A. The antibody purities were > 90% based on SDS gel electrophoresis analysis.
- Recombinant GST-tagged hDPP3 (SEQ ID NO. 1) or a DPP3 peptide (immunization peptide, SEQ ID NO. 2) was immobilized onto a high binding microtiter plate surface (96-Well polystyrene microplates, Greiner Bio-One international AG, Austria, 1 pg/well in coupling buffer [50 mM Tris, 100 mM NaCl, pH7,8], Ih at RT). After blocking with 5% bovine serum albumin, the microplates were vacuum dried.
- T racer T racer
- the purified labeled antibody was diluted in assay buffer (50 mmol/1 potassium phosphate, 100 mmol/1 NaCl, 10 mmol/1 Naz-EDTA, 5 g/1 bovine serum albumin, 1 g/1 murine IgG, 1 g/1 bovine IgG, 50 pmol/1 amastatin, 100 pmol/1 leupeptin, pH 7.4).
- the final concentration was approx. 5-7* 10 6 relative light units (RLU) of labelled compound (approx. 20 ng labeled antibody) per 200 pl.
- acridinium ester chemiluminescence was measured by using a Centro LB 960 luminometer (Berthold Technologies GmbH & Co. KG).
- the plates were filled with 200 pl of labelled and diluted detection antibody (tracer) and incubated for 2-4 h at 2-8 °C. Unbound tracer was removed by washing 4 times with 350 pl washing solution (20 mM PBS, pH 7.4, 0.1 % Triton X-100). Well-bound chemiluminescence was measured by using the Centro LB 960 luminometer (Berthold Technologies GmbH & Co. KG).
- a DPP3 activity assay with known procedure (Jones et al., 1982) was performed.
- Recombinant GST-tagged hDPP3 was diluted in assay buffer (25 ng/ml GST-DPP3 in 50 mM Tris-HCl, pH7,5 and 100 pM ZnCh) and 200 pl of this solution incubated with 10 pg of the respective antibody at room temperature.
- fluorogenic substrate Arg-Arg-0NA (20 pl, 2mM) was added to the solution and the generation of free 0NA over time was monitored using the Twinkle LB 970 microplate fluorometer (Berthold Technologies GmbH & Co.
- the following table represents a selection of obtained antibodies and their binding rate in Relative Light Units (RLU) as well as their relative inhibitory ability (%; Table 3).
- RLU Relative Light Unit
- % relative inhibitory ability
- Table 3 list of antibodies raised against full-length or sequences of hDPP3 and their ability to bind hDPP3 (SEQ ID NO.: 1) or immunization peptide (SEQ ID NO.: 2) in RLU, as well as the maximum inhibition of recombinant GST-hDPP3.
- DPP3-LIA luminescence immunoassay for the quantification of DPP3 protein concentrations
- DPP3- ECA enzyme capture activity assay for the quantification of DPP3 activity
- Example 2 - DPP3 for prognosis of short-term mortality DPP3 concentration in plasma of a variety of diseased patients was determined using a hDPP3 immunoassay (Rehfeld et al. 2019. JALM 3(6): 943-953) and related to the short term-mortality of the patients. Study Cohort - Sepsis and Septic Shock
- AdrenOSS-1 is a prospective, observational, multinational study including 583 patients admitted to the intensive care unit with sepsis or septic shock (Hollinger et al., 2018). 292 patients were diagnosed with septic shock.
- Plasma samples from 108 patients that were diagnosed with cardiogenic shock were screened for DPP3. Blood was drawn within 6 h from detection of cardiogenic shock. Mortality was followed for 7 days.
- Plasma samples from 720 patients with acute coronary syndrome were screened for DPP3. Blood was drawn 24 hours after the onset of ChestPain. Mortality was followed for 7 days.
- Plasma samples from 1440 patients presenting with dyspnea were collected immediately to their entry to the emergency department of Skane University Hospital. Patients with dyspnea may suffer from acute coronary syndrome or congestive heart failure, beside others, and have a high risk for organ failure and short-term mortality. Mortality was followed for 3 months after presentation to the emergency department.
- Plasma samples from 107 patients with severe bums were screened for DPP3. Blood was drawn at admission to the hospital. Mortality was followed for 4 weeks. hDPP3 immunoassay:
- An immune-assay (LIA) or an activity assay (EC A) detecting the amount of human DPP3 (LIA) or the activity of human DPP3 (ECA), respectively, was used for determining the DPP3 level in patient plasma.
- Antibody immobilization, labelling and incubation were performed as described in Rehfeld et al. (Rehfeld et al. 2019. JALM 3(6): 943-953).
- DPP3 was eluted by placing each column in 15-mL falcon tube containing 2 mL of neutralization buffer (IM Tris-HCl, pH 8.0), followed by addition of 10 mL of elution buffer (100 mM Glycine-HCl, 0.1% TritonX-100, pH 3.5) per column and immediate centrifugation for 30 seconds at lOOOxg. The elution step was repeated 3 times in total resulting in 360 mL of combined eluates. The pH of the neutralized eluates was 8.0.
- neutralization buffer IM Tris-HCl, pH 8.0
- the combined eluates were loaded on a 5 mL HiTrap Q-sephare HP column (GE Healthcare) equilibrated with lEX-buffer Al (100 mM Glycine, 150 mM Tris, pH 8.0) using the sample pump of the Akta Start system (GE Healthcare).
- the column was washed with five column volumes of IEX Buffer A2 (12 mM NaHzPC , pH 7.4) to remove unbound protein.
- Elution of DPP3 was achieved by applying a sodium chloride gradient over 10 column volumes (50 mL) in a range of 0 - 1 M NaCl using lEX-buffer B (12 mM NaFhPO ⁇ l M NaCl, pH 7.4).
- the eluates were collected in 2 mL fractions. Buffers used for ion exchange chromatography were sterile filtered using a 0.22 pM bottle-top filter.
- FIG. 4 shows an SDS-PAGE on a gradient gel (4-20%) of native hDPP3 purified from human erythrocyte lysate.
- Table 4 Purification of DPP3 from human erythrocytes a ) Relative DPP3 amount was determined in all fractions using the DPP3-LIA assay. Amount of DPP3 in starting material was set to 100% and remaining DPP3 amount in purification fractions was correlated to the starting material. b ) Total protein amount was determined using the method of Lowry modified by Peterson (Peterson 1977. Analytical Biochemistry 356:346-356 ⁇ . c ) Total Arg2-BNA hydrolyzing activity in pmol of substrate converted per minute was determined using the DPP3-ECA, calibrated via B-naphtylamine (0,05-100 jiM). d ) Purification yield was calculated form total Arg2-BNA hydrolyzing activity. Arg2-BNA hydrolyzing activity in starting material was set to 100%. e ) Specific activity is defined as pmol of substrate converted per minute and mg of total protein.
- the purification factor is the quotient of specific activities after and before each purification step.
- Wild type Black 6 mice (8-12 weeks, group size refer to Table 5) were acclimated during 2 weeks and a baseline echocardiography was done. The mice were randomly allocated to one of the two groups and, subsequently, native DPP3 protein or PBS were injected intravenously via a retro-orbital injection with a dose of 600 pg/kg for DPP3 protein.
- cardiac function was assessed by echocardiography (Gao et al. 2011 and renal function assessed by renal resistive index (Lubas et al., 2014, Dewitte et al, 2012 ⁇ at 15, 60 and 120 minutes (Figure 3).
- mice treated with native DPP3 protein show significantly reduced shortening fraction compared to the control group injected with PBS (Fig 4A).
- the WT+DPP3 group also displays worsening renal function as observed by the renal resistive index increase ( Figure 4B).
- Antibodies raised against SEQ ID No.: 2 were characterized in more detail (epitope mapping, binding affinities, specificity, inhibitory potential). Here the results for clone 1967 of SEQ ID No.: 2 (AK1967; “Procizumab”) are shown as an example.
- peptides & elephants GmbH, Hennigsdorf, Germany were synthesized (peptides & elephants GmbH, Hennigsdorf, Germany). These peptides include the sequence of the full immunization peptide (SEQ ID No. 2) or fragments thereof, with stepwise removal of one amino acid from either C- or N-terminus (see Table 7 for a complete list of peptides).
- Anti-DPP3 antibody AK1967 was labelled with a chemiluminescence label according to Example 1.
- the experiment was performed using Octet Red96 (ForteBio). AK1967 was captured on kinetic grade anti-humanFc (AHC) biosensors. The loaded biosensors were then dipped into a dilution series of recombinant GST-tagged human DPP3 (100, 33.3, 11.1, 3.7 nM). Association was observed for 120 seconds followed by 180 seconds of dissociation. The buffers used for the experiment are depicted in Table 6. Kinetic analysis was performed using a 1: 1 binding model and global fitting.
- Blood cells from human EDTA-blood were washed (3x in PBS), diluted in PBS and lysed by repeated freeze-thaw-cycles.
- the blood cell lysate had a total protein concentration of 250 pg/ml, and a DPP3 concentration of 10 pg/ml.
- Dilutions of blood cell lysate ( 1 :40, 1 : 80, 1 : 160 and 1 :320) and of purified recombinant human His-DPP3 (31.25-500 ng/ml) were subjected to SDS-PAGE and Western Blot.
- the blots were incubated in 1.) blocking buffer (IxPBS-T with 5% skim milk powder), 2.) primary antibody solution (AK1967 1:2.000 in blocking buffer) and 3.) HRP labelled secondary antibody (goat anti mouse IgG, 1:1.000 in blocking buffer). Bound secondary antibody was detected using the Amersham ECL Western Blotting Detection Reagent and the Amersham Imager 600 UV (both from GE Healthcare).
- AK1967 binds with an affinity of 2.2*1 O' 9 M to recombinant GST-hDPP3 (kinetic curves see Figure 5).
- the only protein detected with AK1967 as primary antibody in lysate of blood cells was DPP3 at 80 kDa ( Figure 6).
- the total protein concentration of the lysate was 250 pg/ml whereas the estimated DPP3 concentration is about 10 pg/ml.
- AK1967 binds and detects specifically DPP3 and no other unspecific binding takes place.
- AK1967 inhibits 15 ng/ ml DPP3 in a specific DPP3 activity assay with an IC50 of about 15 ng/ml ( Figure 7).
- the monoclonal antibody AK1967 (“Procizumab”), with the ability of inhibiting DPP3 activity by 70 %, was chosen as possible therapeutic antibody and was also used as template for chimerization and humanization.
- Humanization of murine antibodies may be conducted according to the following procedure:
- the antibody sequence is analyzed for the structural interaction of framework regions (FR) with the complementary determining regions (CDR) and the antigen. Based on structural modelling an appropriate FR of human origin is selected and the murine CDR sequences are transplanted into the human FR. Variations in the amino acid sequence of the CDRs or FRs may be introduced to regain structural interactions, which were abolished by the species switch for the FR sequences. This recovery of structural interactions may be achieved by random approach using phage display libraries or via directed approach guided by molecular modeling (Almagro and Fransson, 2008. Humanization of antibodies. Front Biosci. 13:1619-33).
- variable region can be connected to any subclass of constant regions (IgG, IgM, IgE. IgA), or only scaffolds, Fab fragments, Fv, Fab and F(ab)2.
- IgG constant regions
- IgM constant regions
- IgE. IgA only scaffolds
- Fab fragments fragments
- Fv fragments
- Fab fragments
- F(ab)2 the murine antibody variant with an IgG2a backbone was used.
- chimerization and humanization a human IgG IK backbone was used.
- CDRs Complementarity Determining Regions
- CLP model of septic shock Male Wistar rats (2-3 months, 300 to 400 g, group size refers to Table 8) from the Centre d'elevage Janvier (France) were allocated randomly to one of three groups. All the animals were anesthetized using ketamine hydrochloride (90 mg/ kg) and xylazine (9 mg/ kg) intraperitoneally (i.p.). For induction of polymicrobial sepsis, cecal ligation and puncture (CLP) was performed using Rittirsch’s protocol with minor modification. A ventral midline incision (1.5 cm) was made to allow exteriorization of the cecum. The cecum is then ligated just below the ileocecal valve and punctured once with an 18-gauge needle.
- CLP cecal ligation and puncture
- the abdominal cavity is then closed in two layers, followed by fluid resuscitation (3 ml/ 100 g body of weight of saline injected subcutaneously) and returning the animal to its cage. Sham animals were subjected to surgery, without getting their cecum punctured. CLP animals were randomized between placebo and therapeutic antibody.
- Hemodynamic variables were obtained using the AcqKnowledge system (BIOP AC Systems, Inc., USA). It provides a fully automated blood pressure analysis system.
- the catheter is connected to the BIOP AC system through a pressure sensor.
- rats were anesthetized (ketamine and xylazine). Animals were moved to the heating pad for the desired body temperature to 37-37.5 °C. The temperature feedback probe was inserted into the rectum. The rats were placed on the operating table in a supine position. The trachea was opened and a catheter (16G) was inserted for an external ventilator without to damage carotid arteries and vagus nerves. The arterial catheter was inserted into the right carotid artery. The carotid artery is separate from vagus before ligation.
- a central venous catheter was inserted through the left jugular vein allowing administration of PCZ or PBS.
- BP blood pressure
- TTE transthoracic echocardiographic
- pulmonary artery flow was recorded using pulsed wave Doppler. Velocity time integral of pulmonary artery outflow was measured.
- mitral flow was recorded using pulsed Doppler at the level of the tip of the mitral valves.
- the sepsis-induced heart failure rats treated with PBS show reduced shortening fraction compared to the sham animals (Fig. 9A).
- the CLP+PBS group also displays high mortality rate (Fig. 9B).
- application of Procizumab to sepsis-induced heart failure rats improves shortening fraction (Fig. 9A) and drastically reduces the mortality rate (Fig. 9B).
- Example 7 Effect of Procizumab on heart and kidney function
- Procizumab in isoproterenol-induced heart failure in mice was studied by monitoring the shortening fraction and renal resistive index.
- mice Isoproterenol-induced cardiac stress in mice:
- Acute heart failure was induced in male mice at 3 months of age by two daily subcutaneous injections of 300 mg/kg of Isoproterenol, a non-selective B-adrenergic agonist (DL-Isoproterenol hydrochloride, Sigma Chemical Co) (ISO) for two days (Ver gar o etal, 2016 ⁇ .
- the ISO dilution was performed in NaCl 0.9%.
- mice Isoproterenol-treated mice were randomly assigned to two groups (Table 9) and PBS or Procizumab (10 mg/kg) were injected intravenously after baseline echocardiography (Gao et al., 2011) and renal resistive index measurements (Lubas et al., 2014, Dewitte etal, 2012 ⁇ were performed at day 3 ( Figure 10 A and B).
- Procizumab to isoproterenol-induced heart failure mice restores heart function within the first hour after administration (Fig. 11 A). Kidney function of sick mice shows significant improvement at 6 hours post PCZ injection and is comparable to the kidney function of sham animals at 24 hours (Fig. 11B).
- AdrenOSS-1 circulating DPP3
- organ e.g. cardiovascular and renal dysfunction
- AdrenOSS-1 is a European prospective, observational, multinational study (ClinicalTrials.gov NCT02393781) including 583 patients admitted to the ICU with sepsis or septic shock.
- the primary outcome was 28-day mortality. Secondary outcomes included organ failure defined by SOFA score, organ support with focus on vasopressor use and need for renal replacement therapy. Blood for the central laboratory was sampled within 24 hours after ICU admission and on day 2.
- DPP3-LIA DPP3 protein concentrations
- Example 9 DPP3 in patients infected with coronavirus (SARS-CoV-2)
- Table 10 DPP3 levels in samples from patients infected with coronavirus (SARS-CoV-2)
- DPP3 concentrations ranged between 27 and 975 ng/ml with a median (IQR) of 156 (59.5 - 322.3) ng/ml. DPP3 concentrations are significantly elevated compared to healthy subjects. Samples from 5,400 normal (healthy) subjects (Swedish single-center prospective population-based Study (MPP- RES)) have been measured: median (interquartile range) plasma DPP3 was 14.5 ng/ml (11.3 ng/ml - 19 ng/ml).
- DPP3 was measured in EDTA plasma with a one-step luminescence sandwich immunoassay (LIA) as described recently (Rehfeld et al. 2019. JALM 3(6): 943-953 ⁇ .
- LIA luminescence sandwich immunoassay
- Example 11 Procizumab for cardiac protection in a septic animal model
- Reverse transcription was performed using random hexamer primers and Superscript II Reverse Transcriptase (Invitrogen, Carlsbad, USA), according to the manufacturer’s instructions.
- sense and anti-sense primers were designed using the Primer3 program for sus scrofa IL-6.
- the amplification reaction was performed in triplicate using SYBRGreen PCR Master Mix (Quanta Biosciences, Gaithersburg, MD), specific primers, and diluted template complementary DNA using an iCycler system (BioRad Laboratories).
- Relative quantification was achieved using the comparative 2-AACt method by normalization with the housekeeping gene (beta-actin). Results are expressed as relative fold increase above the mean value of left ventricle relative mRNA expression of the sham group arbitrarily fixed at 1.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Veterinary Medicine (AREA)
- Public Health (AREA)
- Animal Behavior & Ethology (AREA)
- Epidemiology (AREA)
- Organic Chemistry (AREA)
- Immunology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Engineering & Computer Science (AREA)
- Gastroenterology & Hepatology (AREA)
- Molecular Biology (AREA)
- Genetics & Genomics (AREA)
- Biochemistry (AREA)
- Biophysics (AREA)
- Cardiology (AREA)
- Heart & Thoracic Surgery (AREA)
- Chemical Kinetics & Catalysis (AREA)
- General Chemical & Material Sciences (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Peptides Or Proteins (AREA)
Abstract
Description





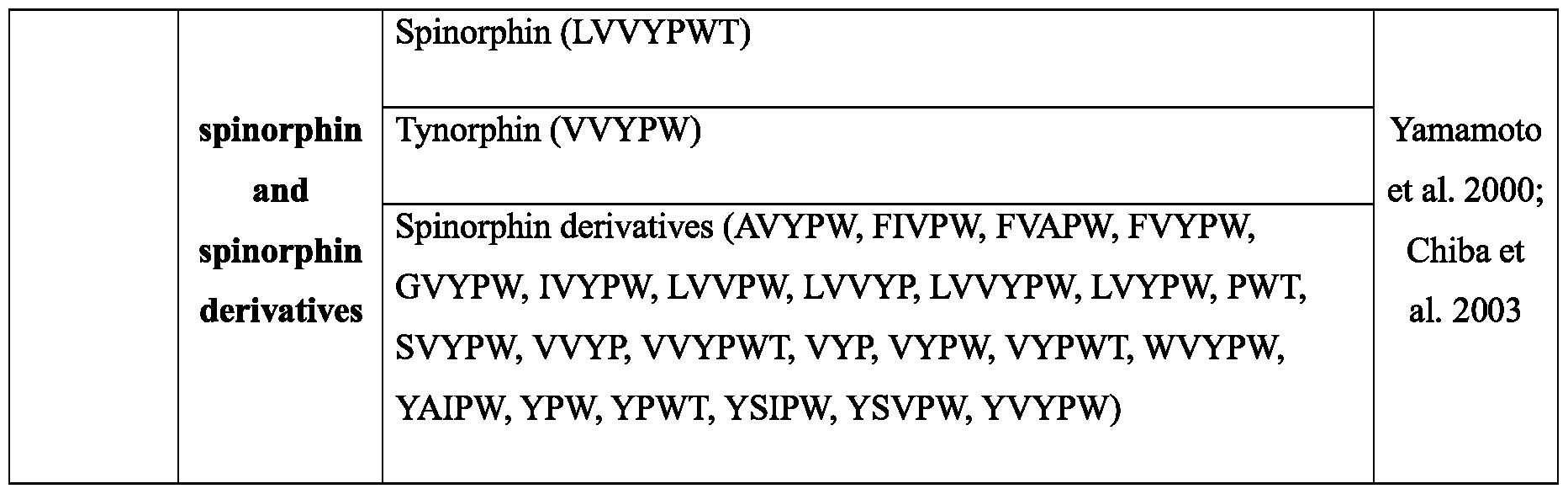









Claims
Priority Applications (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| CN202480018959.XA CN120857945A (en) | 2023-03-29 | 2024-04-02 | DPP3 inhibitors for myocardial protection and prevention of myocardial injury in critically ill patients with hypotension |
| EP24714526.1A EP4687942A1 (en) | 2023-03-29 | 2024-04-02 | Dpp3 inhibitor for myocardial protection and prevention of myocardial injury in critically ill patients with blood pressure decline |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP23165215 | 2023-03-29 | ||
| EP23165215.7 | 2023-03-29 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2024200862A1 true WO2024200862A1 (en) | 2024-10-03 |
Family
ID=85781904
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/EP2024/058887 Ceased WO2024200862A1 (en) | 2023-03-29 | 2024-04-02 | Dpp3 inhibitor for myocardial protection and prevention of myocardial injury in critically ill patients with blood pressure decline |
Country Status (3)
| Country | Link |
|---|---|
| EP (1) | EP4687942A1 (en) |
| CN (1) | CN120857945A (en) |
| WO (1) | WO2024200862A1 (en) |
Citations (24)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4804676A (en) | 1984-10-04 | 1989-02-14 | Sankyo Company Limited | Enkephalinase B inhibitors, their preparation, and pharmaceutical compositions containing the same |
| EP0353971A2 (en) | 1988-08-01 | 1990-02-07 | Ciba Corning Diagnostics Corp. | Acridinium esters and method for detection of an analyte using acridinium esters and liposomes |
| WO1991017271A1 (en) | 1990-05-01 | 1991-11-14 | Affymax Technologies N.V. | Recombinant library screening methods |
| WO1992001047A1 (en) | 1990-07-10 | 1992-01-23 | Cambridge Antibody Technology Limited | Methods for producing members of specific binding pairs |
| WO1992020791A1 (en) | 1990-07-10 | 1992-11-26 | Cambridge Antibody Technology Limited | Methods for producing members of specific binding pairs |
| WO1993012227A1 (en) | 1991-12-17 | 1993-06-24 | Genpharm International, Inc. | Transgenic non-human animals capable of producing heterologous antibodies |
| US5585089A (en) | 1988-12-28 | 1996-12-17 | Protein Design Labs, Inc. | Humanized immunoglobulins |
| US5807715A (en) | 1984-08-27 | 1998-09-15 | The Board Of Trustees Of The Leland Stanford Junior University | Methods and transformed mammalian lymphocyte cells for producing functional antigen-binding protein including chimeric immunoglobulin |
| EP1266025A1 (en) | 2000-02-29 | 2002-12-18 | Compound Therapeutics, Inc. | Protein scaffolds for antibody mimics and other binding proteins |
| US20040023334A1 (en) | 2001-08-30 | 2004-02-05 | Biorexis Pharmaceutical Corporation | Modified transferrin fusion proteins |
| WO2005040229A2 (en) | 2003-10-24 | 2005-05-06 | Avidia, Inc. | Ldl receptor class a and egf domain monomers and multimers |
| EP1941867A1 (en) | 2002-06-07 | 2008-07-09 | Dyax Corporation | Prevention and reduction of blood loss |
| US20100028995A1 (en) | 2004-02-23 | 2010-02-04 | Anaphore, Inc. | Tetranectin Trimerizing Polypeptides |
| WO2010060748A1 (en) | 2008-11-03 | 2010-06-03 | Molecular Partners Ag | Binding proteins inhibiting the vegf-a receptor interaction |
| EP2231860A1 (en) | 2007-12-19 | 2010-09-29 | Affibody AB | Polypeptide derived from protein a and able to bind pdgf |
| WO2011023685A1 (en) | 2009-08-27 | 2011-03-03 | Covagen Ag | Il-17 binding compounds and medical uses thereof |
| EP2314308A1 (en) | 2004-09-21 | 2011-04-27 | BioNTech AG | Use of microproteins as tryptase inhibitors |
| WO2011073214A2 (en) | 2009-12-14 | 2011-06-23 | Scil Proteins Gmbh | A method for identifying hetero-multimeric modified ubiquitin proteins with binding capability to ligands |
| WO2011154420A2 (en) | 2010-06-08 | 2011-12-15 | Pieris Ag | Tear lipocalin muteins binding il-4 r alpha |
| EP2949332A2 (en) | 2013-01-28 | 2015-12-02 | Nuevas Alternativas Naturales Thermafat, S.A.P.I. de C.V. | Compositions for the systemic treatment of pathological conditions resulting from oxidative stress and/or redox imbalance |
| WO2017182561A1 (en) | 2016-04-21 | 2017-10-26 | Sphingotec Therapeutics Gmbh | Methods for determining dpp3 and therapeutic methods |
| WO2019081595A2 (en) | 2017-10-25 | 2019-05-02 | Sphingotec Therapeutics Gmbh | Dpp3 binder directed to and binding to specific dpp3-epitopes and its use in the prevention or treatment of diseases / acute conditions that are associated with oxidative stress |
| WO2021185786A1 (en) | 2020-03-16 | 2021-09-23 | 4TEEN4 Pharmaceuticals GmbH | Dpp3 in patients infected with coronavirus |
| US20220211798A1 (en) * | 2018-12-21 | 2022-07-07 | 4TEEN4 Pharmaceuticals GmbH | Therapy guidance and/or therapy monitoring for a treatment with angiotensin-receptor-agonist and/or a precursor thereof |
-
2024
- 2024-04-02 WO PCT/EP2024/058887 patent/WO2024200862A1/en not_active Ceased
- 2024-04-02 CN CN202480018959.XA patent/CN120857945A/en active Pending
- 2024-04-02 EP EP24714526.1A patent/EP4687942A1/en active Pending
Patent Citations (24)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US5807715A (en) | 1984-08-27 | 1998-09-15 | The Board Of Trustees Of The Leland Stanford Junior University | Methods and transformed mammalian lymphocyte cells for producing functional antigen-binding protein including chimeric immunoglobulin |
| US4804676A (en) | 1984-10-04 | 1989-02-14 | Sankyo Company Limited | Enkephalinase B inhibitors, their preparation, and pharmaceutical compositions containing the same |
| EP0353971A2 (en) | 1988-08-01 | 1990-02-07 | Ciba Corning Diagnostics Corp. | Acridinium esters and method for detection of an analyte using acridinium esters and liposomes |
| US5585089A (en) | 1988-12-28 | 1996-12-17 | Protein Design Labs, Inc. | Humanized immunoglobulins |
| WO1991017271A1 (en) | 1990-05-01 | 1991-11-14 | Affymax Technologies N.V. | Recombinant library screening methods |
| WO1992001047A1 (en) | 1990-07-10 | 1992-01-23 | Cambridge Antibody Technology Limited | Methods for producing members of specific binding pairs |
| WO1992020791A1 (en) | 1990-07-10 | 1992-11-26 | Cambridge Antibody Technology Limited | Methods for producing members of specific binding pairs |
| WO1993012227A1 (en) | 1991-12-17 | 1993-06-24 | Genpharm International, Inc. | Transgenic non-human animals capable of producing heterologous antibodies |
| EP1266025A1 (en) | 2000-02-29 | 2002-12-18 | Compound Therapeutics, Inc. | Protein scaffolds for antibody mimics and other binding proteins |
| US20040023334A1 (en) | 2001-08-30 | 2004-02-05 | Biorexis Pharmaceutical Corporation | Modified transferrin fusion proteins |
| EP1941867A1 (en) | 2002-06-07 | 2008-07-09 | Dyax Corporation | Prevention and reduction of blood loss |
| WO2005040229A2 (en) | 2003-10-24 | 2005-05-06 | Avidia, Inc. | Ldl receptor class a and egf domain monomers and multimers |
| US20100028995A1 (en) | 2004-02-23 | 2010-02-04 | Anaphore, Inc. | Tetranectin Trimerizing Polypeptides |
| EP2314308A1 (en) | 2004-09-21 | 2011-04-27 | BioNTech AG | Use of microproteins as tryptase inhibitors |
| EP2231860A1 (en) | 2007-12-19 | 2010-09-29 | Affibody AB | Polypeptide derived from protein a and able to bind pdgf |
| WO2010060748A1 (en) | 2008-11-03 | 2010-06-03 | Molecular Partners Ag | Binding proteins inhibiting the vegf-a receptor interaction |
| WO2011023685A1 (en) | 2009-08-27 | 2011-03-03 | Covagen Ag | Il-17 binding compounds and medical uses thereof |
| WO2011073214A2 (en) | 2009-12-14 | 2011-06-23 | Scil Proteins Gmbh | A method for identifying hetero-multimeric modified ubiquitin proteins with binding capability to ligands |
| WO2011154420A2 (en) | 2010-06-08 | 2011-12-15 | Pieris Ag | Tear lipocalin muteins binding il-4 r alpha |
| EP2949332A2 (en) | 2013-01-28 | 2015-12-02 | Nuevas Alternativas Naturales Thermafat, S.A.P.I. de C.V. | Compositions for the systemic treatment of pathological conditions resulting from oxidative stress and/or redox imbalance |
| WO2017182561A1 (en) | 2016-04-21 | 2017-10-26 | Sphingotec Therapeutics Gmbh | Methods for determining dpp3 and therapeutic methods |
| WO2019081595A2 (en) | 2017-10-25 | 2019-05-02 | Sphingotec Therapeutics Gmbh | Dpp3 binder directed to and binding to specific dpp3-epitopes and its use in the prevention or treatment of diseases / acute conditions that are associated with oxidative stress |
| US20220211798A1 (en) * | 2018-12-21 | 2022-07-07 | 4TEEN4 Pharmaceuticals GmbH | Therapy guidance and/or therapy monitoring for a treatment with angiotensin-receptor-agonist and/or a precursor thereof |
| WO2021185786A1 (en) | 2020-03-16 | 2021-09-23 | 4TEEN4 Pharmaceuticals GmbH | Dpp3 in patients infected with coronavirus |
Non-Patent Citations (45)
| Title |
|---|
| "The Immunoassay Handbook", May 2005, ELSEVIER |
| ABRAMIC ET AL., BIOLO-AICAL CHEMISTRY,, vol. 381, 2000, pages 1233 - 1243 |
| AGIĊ ET AL., BIOORGANIC CHEMISTRY, vol. 35, no. 2, 2007, pages 153 - 169 |
| BENJAMIN DENIAU ET AL: "Circulating dipeptidyl peptidase 3 is a myocardial depressant factor: dipeptidyl peptidase 3 inhibition rapidly and sustainably improves haemodynamics", EUROPEAN JOURNAL OF HEART FAILURE, vol. 22, no. 2, 31 August 2019 (2019-08-31), NL, pages 290 - 299, XP055681384, ISSN: 1388-9842, DOI: 10.1002/ejhf.1601 * |
| BIRD ET AL., SCIENCE, vol. 242, 1988, pages 423 - 426 |
| BLET ET AL., CRIT CARE, vol. 25, 2021, pages 61 |
| CHAPMAN ET AL.: "Assessment and Classification of Patients with Myocardial Injury and Infarction in Clinical Practice", HEART, vol. 103, no. 1, 2016, pages 10 - 8 |
| CHAULIN, VASCULAR HEALTH AND RISK MANAGEMENT, vol. 17, 2021, pages 299 - 316 |
| CORREA ET AL., CRIT CARE, vol. 19, 2015, pages 98 |
| CVITESIC ET AL., J ENZVME INHIB MED CHEM, vol. 31, 2016, pages 40 - 45 |
| DEANIAU ET AL., EUR J HEART FAIL, vol. 22, no. 2, 2020, pages 290 - 299 |
| DELLINGER ET AL.: "Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock", CRIT CARE MED, vol. 41, no. 2, 2013, pages 580 - 637 |
| DOSTAL ET AL., J MOL CELL CARDIOL, vol. 29, 1997, pages 2893 - 902 |
| E. KABAT ET AL.: "Sequences of Proteins of Immunological Interest,", 1983, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES |
| FRANSSON: "Humanization of antibodies", FRONT BIOSCI., vol. 13, 1 January 2008 (2008-01-01), pages 1619 - 33 |
| FRANSSON: "Humanization of antibodies", FRONT BIOSCI., vol. 13, 2008, pages 1619 - 33 |
| FUCHS ET AL., FASEB J, vol. 17, no. 14, 2003, pages 2118 - 2120 |
| GARG ET AL., INTERNAL AND EMER-AENCY MEDICINE, vol. 12, no. 2, 2017, pages 147 - 155 |
| GOLDBERG ET AL., CIRCULATION, vol. 119, 2009, pages 1211 - 1219 |
| GWECHENBERGER ET AL., CIRCULATION, vol. 99, no. 4, 1999, pages 546 - 551 |
| HALAWA ET AL., POL. ARCH. MED. WEWN, vol. 101, no. 3, 1999, pages 197 - 203 |
| HOCHMAN ET AL., J AM COLL CARDIOL, vol. 36, 2000, pages 1063 - 1070 |
| HOOD ET AL., IMMUNOLOGY, 1984 |
| HULTSCHIJ! C ET AL., CURR OPIN CHEM BIOL., February 2006 (2006-02-01) |
| HUNKAPILLERHOOD, NATURE, vol. 323, 1986, pages 15 - 16 |
| HUSTON ET AL., PROC. NATL. ACAD. SCI. U.S.A, vol. 8 5, 1988, pages 5879 - 588 3 |
| INAOKA ET AL., J. BIOCHEM, vol. 104, no. 5, 1988, pages 706 - 711 |
| JONES ET AL., ANALYTICAL BIOCHEMISTRY, 1982 |
| KIRK-OTHMER: "Encyclopedia of chemical technology", vol. 15, 1993, JOHN WILEY & SONS, pages: 518 - 562 |
| KOZINSKI ET AL., CRITICAL REVIEWS IN CLINICAL LABORATORY SCIENCES, vol. 54, no. 3, 2017, pages 143 - 172 |
| LANZAVECCHIA ET AL., EUR. J. IMMUNOL, vol. 17, 1987, pages 105 |
| LORENZ ET AL., ANTIMICROB AGENTS CHEMOTHER, vol. 55, no. 1, 2011, pages 165 - 173 |
| PARK ET AL., CARDIAC TROPONINS: FROM MYOCARDIAL INFARCTION TO CHRONIC DISEASE. CARDIOVASC RES, vol. 113, no. 14, 2017, pages 1708 - 18 |
| PEBERDV ET AL.: "Post-cardiac arrest care: 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care", CIRCULATION, 2010, pages 768 - 786 |
| PETERSON, ANALYTICAL BIOCHEMISTRY, vol. 356, 1977, pages 346 - 356 |
| RASTIIA ET AL., ACTA CHIMICA SLOVENICA, vol. 62, 2015, pages 867 - 878 |
| REHFELD ET AL., JALM, vol. 3, no. 6, 2019, pages 943 - 953 |
| REYNOLDSHOCHMAN, CIRCULATION, vol. 117, 2008, pages 686 - 697 |
| ROKS ET AL., HEART VESSELS, vol. 12, 1997, pages 119 - 24 |
| SANDOVAL ET AL., CIRCULATION, vol. 146, 2022, pages 569 - 581 |
| SINGER ET AL., JAMA, vol. 315, no. 8, 2016, pages 801 - 810 |
| THVEESEN ET AL., EUR. HEART J, vol. 40, 2019, pages 237 - 269 |
| THYGESEN ET AL.: "Fourth Universal Definition of Myocardial Infarction", EUR HEART J., vol. 40, no. 3, 2018, pages 237 - 69 |
| VINCENTDE BACKER, N. ENGL. J. MED, vol. 370, no. 6, 2014, pages 583 |
| YAMAMOTO ET AL., LIFE SCIENCES, vol. 62, no. 19, 2000, pages 1767 - 1773 |
Also Published As
| Publication number | Publication date |
|---|---|
| EP4687942A1 (en) | 2026-02-11 |
| CN120857945A (en) | 2025-10-28 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| EP4021571B1 (en) | Therapy guidance and/or therapy monitoring for treatment of shock | |
| US20230193348A1 (en) | Dpp3 for therapy guidance, monitoring and stratification of nt-adm antibodies in patients with shock | |
| KR20220145897A (en) | Anti-adrenomedulin (ADM) antibody or anti-ADM antibody fragment or anti-ADM non-IG scaffold for use in the treatment or prevention of shock | |
| JP2025063078A (en) | Therapeutic guidance and/or therapeutic monitoring for treatment with angiotensin receptor agonists and/or their precursors | |
| US20230213519A1 (en) | Dpp3 in patients infected with coronavirus | |
| WO2024200862A1 (en) | Dpp3 inhibitor for myocardial protection and prevention of myocardial injury in critically ill patients with blood pressure decline | |
| US20260028423A1 (en) | Prediction of an increase of dpp3 in a patient with septic shock | |
| WO2024126793A1 (en) | Dpp3 inhibitor for improvement of pulmonary function in critically ill patients | |
| RU2838370C1 (en) | Dpp3 for implementation, monitoring and stratification of therapy with nt-adm antibodies in patients with shock | |
| RU2835616C1 (en) | Therapeutic guidance and/or monitoring therapy for treating shock | |
| EP3922993A1 (en) | Dpp3 in patients infected with coronavirus | |
| CA3207969A1 (en) | Anti-adrenomedullin (adm) antibody or anti-adm antibody fragment or anti-adm non-ig scaffold for use in therapy or prevention of shock and prediction of an increase of dpp3 in a critically ill patient | |
| JP2026016426A (en) | Induction of therapy and/or monitoring of therapy for the treatment of shock syndrome | |
| HK40056645A (en) | Therapy guidance and/or therapy monitoring for a treatment with angiotensin-receptor-agonist and/or a precursor thereof |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 24714526 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 202480018959.X Country of ref document: CN |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2025555289 Country of ref document: JP |
|
| WWP | Wipo information: published in national office |
Ref document number: 202480018959.X Country of ref document: CN |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2024714526 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2024714526 Country of ref document: EP Effective date: 20251029 |
|
| ENP | Entry into the national phase |
Ref document number: 2024714526 Country of ref document: EP Effective date: 20251029 |
|
| ENP | Entry into the national phase |
Ref document number: 2024714526 Country of ref document: EP Effective date: 20251029 |
|
| ENP | Entry into the national phase |
Ref document number: 2024714526 Country of ref document: EP Effective date: 20251029 |
|
| ENP | Entry into the national phase |
Ref document number: 2024714526 Country of ref document: EP Effective date: 20251029 |