WO2020127885A1 - Compositions for treating cancers and resistant cancers - Google Patents
Compositions for treating cancers and resistant cancers Download PDFInfo
- Publication number
- WO2020127885A1 WO2020127885A1 PCT/EP2019/086546 EP2019086546W WO2020127885A1 WO 2020127885 A1 WO2020127885 A1 WO 2020127885A1 EP 2019086546 W EP2019086546 W EP 2019086546W WO 2020127885 A1 WO2020127885 A1 WO 2020127885A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- seq
- amino acid
- acid sequence
- antibody
- cancer
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/16—Amides, e.g. hydroxamic acids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
- A61K39/39533—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum against materials from animals
- A61K39/3955—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum against materials from animals against proteinaceous materials, e.g. enzymes, hormones, lymphokines
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2881—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against CD71
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/70—Immunoglobulins specific features characterized by effect upon binding to a cell or to an antigen
- C07K2317/76—Antagonist effect on antigen, e.g. neutralization or inhibition of binding
Definitions
- the invention is in the field of cancerology. More particularly, the invention relates to use of anti-transferrin receptor 1 antibodies and ion chelators, as a combined preparation for use in the treatment of cancers and resistant cancers.
- TfRl Transferrin receptor 1
- holo-Tf serum Fe3+- loaded transferrin
- Iron chelators are iron binding molecules that bind iron and block its function. They are principally used in the treatment of iron overload diseases.
- TfRl is ubiquitously expressed at low levels by almost all cells. However, higher levels exist on cells that need large amounts of iron such as maturing erythroid precursor cells which require iron for hemoglobin synthesis. Nevertheless, TfRl is not expressed on pluripotent hematopoietic stem cells and on mature erythrocytes (Gross et al., 1997). TfRl-knock out mice exhibit severe anemia and die by embryonic day 12.5. High TfRl expression is reported on placental trophoblasts which need the TfRl to transport iron to maturing erythroid precursor cells.
- TfRl is also present on rapidly proliferating cells including the intestinal epithelium, the basal epidermis and activated lymphocytes (Haynes et al., 1981; Gatter et al., 1983). TfRl is expressed as well on the endocrine pancreas, vascular endothelium of brain capillaries (blood brain barrier), seminiferous tubules of the testes, breast luminal membranes, pituitary cells, kuppfer cells of liver, kidney tubules, and hepatocytes (Gatter et al., 1983).
- Cancer cells need more iron than normal cells and they express higher TfRl levels. For example, breast cancer cells show 4-5 fold higher TfRl level than normal breast cells (Walker and Day, 1986). A higher rate of recurrence was correlated with high TfRl expression in primary bladder malignancies (Smith et al., 1990). Higher TfRl correlated with the tumor grade and prognosis in non hodgkin’s lymphoma, lung adenocarcinoma, breast cancer, gliomas, and chronic lyphocytic leukemias (Habeshaw et al., 1983; Kondo et al., 1990; Yang et al., 2001; Prior et al., 1990; Das Gupta and Shah, 1990).
- the invention relates to i) an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of cancers.
- TfRl antibody anti- transferrin receptor 1
- iron chelator an iron chelator
- cancer cells are proliferating rapidly and require higher iron levels than normal cells representing a good target for iron chelators.
- Inventors hypothesis is that combining iron chelator and an antibody anti- transferrin receptor 1 (TfRl) such as H7 with each acting on a separate iron source (chelators on the LIP and iron stored in ferritin of cancer cells) and H7 (iron from internalized holo-Tf), they can improve the iron deprivation efficiency in the iron avid cancer cells.
- TfRl antibody anti- transferrin receptor 1
- DFO and DFX iron chelators in this study since, besides the fact that they are used in the clinic, they have different characteristics.
- DFO is not liposoluble, it can nevertheless enter slowly into the cells and localize merely in the cytosol (Hoyes and Porter, 1993) while DFX is liposoluble and has access to intracellular organelles in addition to the cytosol (Glickstein et al., 2005).
- Redox properties of iron are different for the 2 chelators, totally neutralized by the hexadentate iron chelator DFO but not with the tridentate chelator DFX.
- the invention relates to an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of cancers.
- TfRl antibody anti- transferrin receptor 1
- iron chelator an iron chelator
- the invention relates to a method for treating cancer and resistant cancers in a subject in need thereof comprising a step of administering said subject with a therapeutically amount of i)an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation.
- a therapeutically amount of i)an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator as a combined preparation.
- the terms“treating” or“treatment” refer to both prophylactic or preventive treatment as well as curative or disease modifying treatment, including treatment of subject at risk of contracting the disease or suspected to have contracted the disease as well as subject who are ill or have been diagnosed as suffering from a disease or medical condition, and includes suppression of clinical relapse.
- the treatment may be administered to a subject having a medical disorder or who ultimately may acquire the disorder, in order to prevent, cure, delay the onset of, reduce the severity of, or ameliorate one or more symptoms of a disorder or recurring disorder, or in order to prolong the survival of a subject beyond that expected in the absence of such treatment.
- therapeutic regimen is meant the pattern of treatment of an illness, e.g., the pattern of dosing used during therapy.
- a therapeutic regimen may include an induction regimen and a maintenance regimen.
- the phrase “induction regimen” or “induction period” refers to a therapeutic regimen (or the portion of a therapeutic regimen) that is used for the initial treatment of a disease.
- the general goal of an induction regimen is to provide a high level of drug to a subject during the initial period of a treatment regimen.
- An induction regimen may employ (in part or in whole) a "loading regimen", which may include administering a greater dose of the drug than a physician would employ during a maintenance regimen, administering a drug more frequently than a physician would administer the drug during a maintenance regimen, or both.
- maintenance regimen refers to a therapeutic regimen (or the portion of a therapeutic regimen) that is used for the maintenance of a subject during treatment of an illness, e.g., to keep the subject in remission for long periods of time (months or years).
- a maintenance regimen may employ continuous therapy (e.g., administering a drug at a regular intervals, e.g., weekly, monthly, yearly, etc.) or intermittent therapy (e.g., interrupted treatment, intermittent treatment, treatment at relapse, or treatment upon achievement of a particular predetermined criteria [e.g., pain, disease manifestation, etc.]).
- the term“subject” denotes a mammal, such as a rodent, a feline, a canine, and a primate.
- the subject according to the invention is a human. More particularly, the subject according to the invention has or susceptible to have a cancer. In a particular embodiment, the subject according to the invention has or susceptible to have a pancreatic cancer. More particularly, the subject according to the invention has or susceptible to have a pancreatic ductal adenocarcinoma (PD AC).
- PD AC pancreatic ductal adenocarcinoma
- the term“cancer” refers to an abnormal cells divide without control and can invade nearby tissues. Cancer cells can also spread to other parts of the body through the blood and lymph systems. There are several main types of cancer. In the context of the invention, the term“cancers” relates to cancers which absorb iron. More particularly, iron uptake by transferrin receptor is the most important way for cancer cells to absorb iron which in required for their survival.
- the cancer is selected from the following group but not limited to: pancreatic cancer, neuroblastoma, solid cancer, leukemia, lymphoma, glioblastoma, breast cancer, cancer related cachexia, gastrointestinal cancer such as colorectal cancer, cholangiocarcinoma, carcinoma of the oral cavity, gastric cancer, lung cancer such as small cell lung cancer, lung adenocarcinoma, melanoma, multiple myeloma, ovarian cancer, prostate cancer, renal cancer, hepatocarcinoma.
- pancreatic cancer More particularly, the cancer is pancreatic cancer.
- pancreatic cancer There are different types of pancreatic cancer. They are divided into two main groups, based on the different types of cells found in the pancreas. Exocrine tumours start in the exocrine cells, where enzymes that help to digest food are made. 96% pancreatic cancers are exocrine tumours.
- pancreatic ductal adenocarcinoma PDAC
- Neuroendocrine tumours start in the neuroendocrine cells. These cells produce hormones that help control the normal functions of the body. For example, they produce insulin which helps to control the level of sugar in the blood. These tumours are known as pancreatic neuroendocrine tumours or PancNETs.
- the cancer is pancreatic ductal adenocarcinoma (PDAC).
- Pancreatic ductal adenocarcinoma is a type of exocrine pancreatic cancer. It is the most common type of pancreatic cancer 95% of all pancreatic cancers are PDAC.
- PDAC develops from cells lining small tubes in the pancreas called ducts (duct cells in the diagram above). These carry the digestive juices, which contain enzymes, into the main pancreatic duct and then on into the duodenum (first part of the small intestine).
- PDAC can grow anywhere in the pancreas, though it is most often found in the head of the pancreas. Symptoms can include tummy (abdominal) and back pain, weight loss and changes to bowel habits.
- transferrin receptor refers to a membrane transport protein which is involved in iron uptake in vertebrates. It imports iron by internalizing the transferrin- iron complex through receptor-mediated endocytosis.
- transferrin receptor protein 1 transferrin receptor protein 1
- TfR2 Transferrin receptor 2
- TfRl transferrin receptor protein 1
- CD71 Cluster of Differentiation 71
- TfRl is a transmembrane glycoprotein composed of two disulfide-linked monomers joined by two disulfide bonds.
- antibody is used in the broadest sense and specifically covers monoclonal antibodies, polyclonal antibodies, multispecific antibodies (e.g. bispecific antibodies) formed from at least two intact antibodies, and antibody fragments so long as they exhibit the desired biological activity of TfRl . Typically, such antibody inhibits the iron transport in the tumour cells.
- the term includes antibody fragments that comprise an antigen binding domain such as Fab', Fab, F(ab')2, single domain antibodies (DABs), TandAbs dimer, Fv, scFv (single chain Fv), dsFv, ds-scFv, Fd, linear antibodies, minibodies, diabodies, bispecific antibody fragments, bibody, tribody (scFv-Fab fusions, bispecific or trispecific, respectively); sc-diabody; kappa(lamda) bodies (scFv-CL fusions); BiTE (Bispecific T-cell Engager, scFv-scFv tandems to attract T cells); DVD-Ig (dual variable domain antibody, bispecific format); SIP (small immunoprotein, a kind of minibody); SMIP ("small modular immunopharmaceutical” scFv-Fc dimer; DART (ds-stabilized diabody "Dual Affinity ReTargeting"
- Antibodies can be fragmented using conventional techniques. For example, F(ab')2 fragments can be generated by treating the antibody with pepsin. The resulting F(ab')2 fragment can be treated to reduce disulfide bridges to produce Fab' fragments. Papain digestion can lead to the formation of Fab fragments.
- Fab, Fab' and F(ab')2, scFv, Fv, dsFv, Fd, dAbs, TandAbs, ds-scFv, dimers, minibodies, diabodies, bispecific antibody fragments and other fragments can also be synthesized by recombinant techniques or can be chemically synthesized. Techniques for producing antibody fragments are well known and described in the art. For example, each of Beckman et al., 2006; Holliger & Hudson, 2005; Le Gall et al., 2004; Reff & Heard, 2001 ; Reiter et al., 1996; and Young et al., 1995 further describe and enable the production of effective antibody fragments.
- the antibody is a“chimeric” antibody as described in U.S. Pat. No. 4,816,567.
- the antibody is a humanized antibody, such as described U.S. Pat. Nos. 6,982,321 and 7,087,409.
- the antibody is a human antibody.
- A“human antibody” such as described in US 6,075, 181 and 6, 150,584.
- the antibody is a single domain antibody such as described in EP 0 368 684, WO 06/030220 and WO 06/003388.
- the antibody is a monoclonal antibody.
- Monoclonal antibodies can be prepared and isolated using any technique that provides for the production of antibody molecules by continuous cell lines in culture. Techniques for production and isolation include but are not limited to the hybridoma technique, the human B-cell hybridoma technique and the EBV-hybridoma technique.
- the antibody anti-TfRl is conjugated to the drugs. Said antibody is called as antibody drug conjugate (ADC). In a particular embodiment, such antibody is combined with the potency of chemotherapeutic agents.
- ADC antibody drug conjugate
- the antibody anti-TfRl is able to induce cytotoxicity, also known as the antibody-dependent cell-mediated cytotoxicity (ADCC).
- ADCC is a mechanism of cell-mediated immune defense whereby an effector cell of the immune system actively lyses a target cell, whose membrane-surface antigens have been bound by specific antibodies.
- variable region Three highly divergent stretches within the variable region of the heavy and light chains are referred to as“hypervariable regions” which are interposed between more conserved flanking stretches known as“framework region” or“FRs”.
- FR refers to amino acid sequences which are naturally found between and adjacent to hypervariable region.
- three hypervariable regions of a light chain and three hypervariable regions of a heavy chain are disposed relative to each other in three dimensional space to form an antigen binding surface. This surface mediates recognition and binding of the target antigen.
- the three hypervariable regions of each of the heavy and light chain are referred to as “complementary determining regions” or“CDRs” and are characterized, for example by Rabat et al.
- the residues in antibody variable domains are conventionally numbered according to a system devised by Rabat et al.
- This system is set forth in Rabat et al., 1987, in Sequences of Proteins of Immunological Interest, US Department of Health and Human Services, NIH, USA (hereafter“Rabat et al”). This numbering system is used in the present specification.
- the Rabat residue designations do not always correspond directly with the linear numbering of the amino acid residues in SEQ ID sequences.
- the actual linear amino acid sequence may contain fewer or additional amino acids than in the strict Rabat numbering corresponding to a shortening of, or insertion into, a structural component, whether framework or complementarity determining region (CDR), of the basic variable domain structure.
- CDR complementarity determining region
- the correct Rabat numbering of residues may be determined for a given antibody by alignment of residues of homology in the sequence of the antibody with a“standard” Rabat numbered sequence.
- the CDRs of the heavy chain variable domain are located at residues 31-35B (H- CDR1), residues 50-65 (H-CDR2) and residues 95-102 (H-CDR3) according to the Rabat numbering system.
- the CDRs of the light chain variable domain are located at residues 24-34 (L-CDR1), residues 50-56 (L-CDR2) and residues 89-97 (L-CDR3) according to the Rabat numbering system. (htp://www.bioiiif.org.Uk/abs/#cdrdef).
- the CDR of the antibodies of the invention are in the Rabat nomenclature.
- the antibody for use according to the invention wherein said antibody is an anti-TfRl antibody chosen among H7, F12, C32, F2, H9, G9.
- the antibody for use according to the invention wherein said antibody is H7 (SEQ ID NO: 1).
- the H7 antibody has the following sequences as described below:
- the antibody for use according to the invention wherein said antibody is H7 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:2, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:3, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:4, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:5; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:6, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:7.
- the antibody for use according to the invention wherein said antibody is F12 antibody (SEQ ID NO: 10).
- the F12 antibody has the following sequences as described below:
- the antibody for use according to the invention wherein said antibody is F12 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO: 11, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO: 12, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO: 13, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO: 14; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO: 15, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO: 16.
- F12 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO: 11, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO: 12, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO: 13, (d) a light chain CDR1 comprising the amino acid sequence of SEQ
- the antibody for use according to the invention wherein said antibody is C32 antibody (SEQ ID NO: 19).
- the C32 antibody has the following sequences as described below:
- the antibody for use according to the invention wherein said antibody is C32 antibody comprising: a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:20, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:21, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:22, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:23; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:24, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:25.
- the antibody for use according to the invention wherein said antibody is F2 antibody (SEQ ID NO: 28).
- the F2 antibody has the following sequences as described below:
- the antibody for use according to the invention wherein said antibody is F2 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:29, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:30, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:31, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:32; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:33, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:34.
- F2 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:29, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:30, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:31, (d) a light chain CDR1 comprising
- the antibody for use according to the invention wherein said antibody is H9 antibody (SEQ ID NO: 37).
- the H9 antibody has the following sequences as described below:
- the antibody for use according to the invention wherein said antibody is H9 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:38, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:39, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:40, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:41 ; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:42, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:43.
- the antibody for use according to the invention wherein said antibody is G9 antibody (SEQ ID NO: 46).
- the H9 antibody has the following sequences as described below:
- the antibody for use according to the invention wherein said antibody is G9 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:47, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:48, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:49, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:50; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:51, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:52.
- G9 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:47, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:48, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:49, (d) a light chain CDR1 comprising
- iron chelator refers to synthetic and natural iron chelators which chelate iron. Chelation is a type of bonding of ions and molecules to metal ion. Chelation therapy is used as nutritional supplement, dental and oral application, heavy-metal detoxification, and as pharmaceuticals. Iron-chelation therapy has its origins in the treatment of iron-overload syndromes. In the context of the invention, the iron chelator is used in combination with an anti-transferrin receptor 1 antibody as described above.
- Iron chelators are well-known in the art and include but not limited to: Deferoxamine (Desferal®, DFO), Desferrithiocinn (DFT), Deferiprone (Ferriprox®), 8-hydroxy quinoline derivatives, Deferasirox (ICL670; Exjade®, DFX), Tachpyridin, Dexrazone (ICRF-197; DZR), Thiosemicarbazones, Pyridoxal isonicotinoyl hydrazone analogs, phytochemicals (Proanthocyanidins, epicatechins, flavonols and anthocyanin), Herbal remedies (curcumin, Kolaviron, PycnogenolTM, Baicalein and its glycoside baicalin, Tetramethylpyrazine and ferulic acid).
- the iron chelator is Deferoxamine (DFO). It is a natural product produced by the bacterium, Streptomyces pilosus. It was the first chelator introduced in the clinic for iron overload treatment. It is a hexadentade chelator that binds selectively ferric Fe 3+ with high affinity forming a 1 : 1 complex Deferoxamine acts by binding free iron in the bloodstream and enhancing its elimination in the urine. DFO is commercialized as Desferal®, by Novartis. The chemical formula of DFO is: C25H48N608.
- DFO refers to Butanedi amide, N'-[5-[[4-[[5-(acetylhydroxyamino)pentyl]amino]-l,4-dioxobutyl]hydroxyamino]pentyl]-N- (5-aminopentyl)-N-hydroxy and has the following structure (formula I) and CAS number: 70- 51-9:
- the iron chelator is Deferasirox (DFX). It is a synthetic tridentate iron chelator that binds Fe3+ iron and forms a 2: 1 ligand to iron complex allowing iron to catalyze redox reactions. It is commercialized as Exjade by Novartis.
- the cas number of DFX is 201530-41-8.
- DFX has the following chemical formula C21H15N304 and structure (formula II) in the art: Benzoic acid, 4-[3,5-bis(2-hydroxyphenyl)-lH-l,2,4-triazol-l-yl]-:
- the term“simultaneous use” refers to an administration of 2 active ingredients by the same route and at the same time or at substantially the same time.
- the term “separate use” refers to an administration of 2 active ingredients at the same time or at substantially the same time by different routes.
- the term “sequential use” refers to an administration of 2 active ingredients at different times, the administration route being identical or different.
- the invention relates to i)an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of resistant cancers.
- resistant cancers refers to a cancer that does not respond to treatment notably to convention therapies (chemotherapy, radiotherapy etc).
- the cancer is resistant at the beginning of treatment.
- the cancer become resistant during treatment, such cancer is called refractory cancer.
- the term“subject” denotes a mammal, such as a rodent, a feline, a canine, and a primate.
- the subject according to the invention is a human. More particularly, the subject according to the invention has or susceptible to have resistant cancer.
- the resistant cancer is selected from the group consisting of but not limited to pancreatic cancer, neuroblastoma, leukemia, lymphoma, glioblastoma, colon cancer.
- the cancer is resistant to rituximab.
- Rituximab is a chimeric monoclonal antibody against the protein CD20.
- the cancer is resistant to an immune check point inhibitor.
- immune checkpoint inhibitor refers to molecules that totally or partially reduce, inhibit, interfere with or modulate one or more immune checkpoint proteins.
- immune checkpoint protein has its general meaning in the art and refers to a molecule that is expressed by T cells in that either turn up a signal (stimulatory checkpoint molecules) or turn down a signal (inhibitory checkpoint molecules).
- Immune checkpoint molecules are recognized in the art to constitute immune checkpoint pathways similar to the CTLA-4 and PD-1 dependent pathways (see e.g. Pardoll, 2012. Nature Rev Cancer 12:252-264; Mellman et al. , 2011. Nature 480:480- 489).
- Examples of stimulatory checkpoint include CD27 CD28 CD40, CD122, CD137, 0X40, GITR, and ICOS.
- inhibitory checkpoint molecules examples include A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 and VISTA.
- A2AR Adenosine A2A receptor
- B7-H4 also called VTCN1
- B and T Lymphocyte Attenuator (BTLA) and also called CD272 has HVEM (Herpesvirus Entry Mediator) as its ligand.
- HVEM Herpesvirus Entry Mediator
- Surface expression of BTLA is gradually downregulated during differentiation of human CD8+ T cells from the naive to effector cell phenotype, however tumor-specific human CD8+ T cells express high levels of BTLA.
- CTLA-4 Cytotoxic T -Lymphocyte- Associated protein 4 and also called CD152. Expression of CTLA-4 on Treg cells serves to control T cell proliferation.
- IDO Indoleamine 2, 3 -di oxygenase
- TDO tryptophan catabolic enzyme
- Another important molecule is TDO, tryptophan 2,3 -di oxygenase.
- IDO is known to suppress T and NK cells, generate and activate Tregs and myeloid-derived suppressor cells, and promote tumour angiogenesis.
- KIR Killer-cell Immunoglobulin-like Receptor
- LAG3, Lymphocyte Activation Gene-3 works to suppress an immune response by action to Tregs as well as direct effects on CD8+ T cells.
- PD- 1 Programmed Death 1 (PD-1) receptor
- PD-L1 and PD-L2 This checkpoint is the target of Merck & Co.'s melanoma drug Keytruda, which gained FDA approval in September 2014.
- An advantage of targeting PD-1 is that it can restore immune function in the tumor microenvironment.
- TIM-3 short for T-cell Immunoglobulin domain and Mucin domain 3, expresses on activated human CD4+ T cells and regulates Thl and Thl7 cytokines.
- TIM-3 acts as a negative regulator of Thl/Tcl function by triggering cell death upon interaction with its ligand, galectin-9.
- VISTA Short for V-domain Ig suppressor of T cell activation, VISTA is primarily expressed on hematopoietic cells so that consistent expression of VISTA on leukocytes within tumors may allow VISTA blockade to be effective across a broad range of solid tumors. Tumor cells often take advantage of these checkpoints to escape detection by the immune system. Thus, inhibiting a checkpoint protein on the immune system may enhance the anti-tumor T-cell response.
- an immune checkpoint inhibitor refers to any compound inhibiting the function of an immune checkpoint protein. Inhibition includes reduction of function and full blockade.
- the immune checkpoint inhibitor could be an antibody, synthetic or native sequence peptides, small molecules or aptamers which bind to the immune checkpoint proteins and their ligands.
- the immune checkpoint inhibitor is an antibody.
- antibodies are directed against A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 or VISTA.
- the immune checkpoint inhibitor is an anti -PD- 1 antibody such as described in WO2011082400, W02006121168, W02015035606, W02004056875, W02010036959, W02009114335, W02010089411, WO2008156712, WO2011110621, WO2014055648 and WO2014194302.
- anti-PD-1 antibodies which are commercialized: Nivolumab (Opdivo®, BMS), Pembrolizumab (also called Lambrolizumab, KEYTRUDA® or MK-3475, MERCK).
- the immune checkpoint inhibitor is an anti-PD-Ll antibody such as described in WO2013079174, W02010077634, W02004004771, WO2014195852, W02010036959, WO2011066389, W02007005874, W02015048520, US8617546 and WO2014055897.
- anti-PD-Ll antibodies which are on clinical trial: Atezolizumab (MPDL3280A, Genentech/Roche), Durvalumab (AZD9291, AstraZeneca), Avelumab (also known as MSB0010718C, Merck) and BMS-936559 (BMS).
- the immune checkpoint inhibitor is an anti-PD-L2 antibody such as described in US7709214, US7432059 and US8552154.
- the immune checkpoint inhibitor inhibits Tim-3 or its ligand.
- the immune checkpoint inhibitor is an anti-Tim-3 antibody such as described in WO03063792, WO2011155607, WO2015117002, WO2010117057 and W02013006490.
- the immune checkpoint inhibitor is a small organic molecule.
- small organic molecule refers to a molecule of a size comparable to those organic molecules generally used in pharmaceuticals.
- small organic molecules range in size up to about 5000 Da, more preferably up to 2000 Da, and most preferably up to about 1000 Da.
- the small organic molecules interfere with transduction pathway of A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 or VISTA.
- small organic molecules interfere with transduction pathway of PD-1 and Tim-3.
- they can interfere with molecules, receptors or enzymes involved in PD-1 and Tim-3 pathway.
- the small organic molecules interfere with Indoleamine- pyrrole 2,3-dioxygenase (IDO) inhibitor.
- IDO is involved in the tryptophan catabolism (Liu et al 2010, Vacchelli et al 2014, Zhai et al 2015). Examples of IDO inhibitors are described in WO 2014150677.
- IDO inhibitors include without limitation 1 -methyl-tryptophan (IMT), b- (3-benzofuranyl)-alanine, P-(3-benzo(b)thienyl)-alanine), 6-nitro-tryptophan, 6- fluoro-tryptophan, 4-methyl-tryptophan, 5 -methyl tryptophan, 6-methyl-tryptophan, 5- methoxy -tryptophan, 5 -hydroxy -tryptophan, indole 3-carbinol, 3,3'- diindolylmethane, epigallocatechin gallate, 5-Br-4-Cl-indoxyl 1,3-diacetate, 9- vinylcarbazole, acemetacin, 5- bromo-tryptophan, 5-bromoindoxyl diacetate, 3- Amino-naphtoic acid, pyrrolidine dithiocarbamate, 4-phenylimidazole a brassinin derivative, a thiohyl
- the IDO inhibitor is selected from 1 -methyl -tryptophan, b-(3- benzofuranyl)-alanine, 6-nitro-L-tryptophan, 3- Amino-naphtoic acid and b-[3- benzo(b)thienyl] -alanine or a derivative or prodrug thereof.
- the inhibitor of IDO is Epacadostat, (INCB24360, INCB024360) has the following chemical formula in the art and refers to -N-(3-bromo-4- fluorophenyl)-N'-hydroxy-4- ⁇ [2-(sulfamoylamino)-ethyl]amino ⁇ -l,2,5-oxadiazole-3 carboximidamide :
- the inhibitor is BGB324, also called R428, such as described in W02009054864, refers to lH-1, 2, 4-Triazole-3, 5-diamine, l-(6,7-dihydro-5H- benzo[6,7]cyclohepta[l,2-c]pyridazin-3-yl)-N3-[(7S)-6,7,8,9-tetrahydro-7-(l-pyrrolidinyl)- 5H-benzocyclohepten-2-yl]- and has the following formula in the art:
- the inhibitor is CA-170 (or AUPM-170): an oral, small molecule immune checkpoint antagonist targeting programmed death ligand-1 (PD-L1) and V- domain Ig suppressor of T cell activation (VISTA) (Liu et al 2015).
- PD-170 or AUPM-170
- VISTA V- domain Ig suppressor of T cell activation
- the immune checkpoint inhibitor is an aptamer.
- the aptamers are directed against A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 or VISTA.
- aptamers are DNA aptamers such as described in Prodeus et al 2015.
- a major disadvantage of aptamers as therapeutic entities is their poor pharmacokinetic profiles, as these short DNA strands are rapidly removed from circulation due to renal filtration.
- aptamers according to the invention are conjugated to with high molecular weight polymers such as polyethylene glycol (PEG).
- PEG polyethylene glycol
- the aptamer is an anti -PD-1 aptamer.
- the anti -PD-1 aptamer is MP7 pegylated as described in Prodeus et al 2015.
- the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator is used in combination with a third agent for treatment of a disease or disorder.
- the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator may be used in combination with conventional cancer therapies such as, e.g., surgery, radiotherapy, chemotherapy, or combinations thereof.
- the present invention also provides for therapeutic applications where the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator are used in combination with at least one further therapeutic agent, e.g. for treating cancers and metastatic cancers.
- Such administration may be simultaneous, separate or sequential.
- the agents may be administered as one composition or as separate compositions, as appropriate.
- the further therapeutic agent is typically relevant for the disorder to be treated.
- Exemplary therapeutic agents include other anti-cancer antibodies, cytotoxic agents, chemotherapeutic agents, radiotherapeutics agents, anti-angiogenic agents, anti-cancer immunogens, cell cycle control/apoptosis regulating agents, hormonal regulating agents, and other agents described below.
- inventors combined gemcitabine treatment (the reference treatment for PD AC) to iron deprivation using H7 and iron chelator combination. Indeed, in preliminary experiments they observe a synergistic effect of DFX and gemcitabine in BxPC3 3D cultures which is additionally increased by H7 treatment. By using an anti-TfRl antibody, they could also benefit in vivo from the ADCC capabilities of H7 in addition to the intrinsic effects accomplished by iron deprivation.
- the invention relates to an i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) a chemotherapeutic agent for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
- TfRl antibody anti- transferrin receptor 1
- iron chelator an iron chelator
- chemotherapeutic agent for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
- chemotherapeutic agent refers to chemical compounds that are effective in inhibiting tumor growth.
- examples of chemotherapeutic agents include alkylating agents such as thiotepa and cyclosphosphamide; alkyl sulfonates such as busulfan, improsulfan and piposulfan; aziridines such as benzodopa, carboquone, meturedopa, and uredopa; ethylenimines and methylamelamines including altretamine, triethylenemelamine, trietylenephosphoramide, triethylenethiophosphaorarnide and trimethylolomelamine; acetogenins (especially bullatacin and bullatacinone); a carnptothecin (including the synthetic analogue topotecan); bryostatin; callystatin; CC-1065 (including its adozelesin, carzelesin and bizelesin synthetic analogues);
- calicheamicin especially calicheamicin (11 and calicheamicin 211, see, e.g., Agnew Chem Inti. Ed. Engl. 33 : 183-186 (1994); dynemicin, including dynemicin A; an esperamicin; as well as neocarzinostatin chromophore and related chromoprotein enediyne antiobiotic chromomophores), aclacinomysins, actinomycin, authramycin, azaserine, bleomycins, cactinomycin, carabicin, canninomycin, carzinophilin, chromomycins, dactinomycin, daunorubicin, detorubicin, 6-diazo-5-oxo-L-norleucine, doxorubicin (including morpholino- doxorubicin, cyanomorpholino-doxorubicin, 2-pyr
- paclitaxel (TAXOL®, Bristol-Myers Squibb Oncology, Princeton, N.].) and doxetaxel (TAXOTERE®, Rhone-Poulenc Rorer, Antony, France); chlorambucil; gemcitabine; 6- thioguanine; mercaptopurine; methotrexate; platinum analogs such as cisp latin and carhop latin; vinblastine; platinum; etoposide (VP- 16); ifosfamide; mitomycin C; mitoxantrone; vincristine; vinorelbine; navelbine; novantrone; teniposide; daunomycin; aminopterin; xeloda; ibandronate; CPT-1 1 ; topoisomerase inhibitor RFS 2000; difluoromethylornithine (DMFO); retinoic acid; capecitabine; and pharmaceutically acceptable salts, acids or derivatives of any of the above.
- antihormonal agents that act to regulate or inhibit honnone action on tumors
- anti-estrogens including for example tamoxifen, raloxifene, aromatase inhibiting 4(5)-imidazoles, 4-hydroxytamoxifen, trioxifene, keoxifene, LY117018, onapristone, and toremifene (Fareston); and anti-androgens such as flutamide, nilutamide, bicalutamide, leuprolide, and goserelin; and pharmaceutically acceptable salts, acids or derivatives of any of the above.
- the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator are used in combination with gemcitabine.
- the i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator are used in combination with Monomethyl Auristatin F (MMAF) which is a synthetic antineoplastic agent and an inhibitor of microtubule polymerization using a non-cleavable linker.
- MMAF Monomethyl Auristatin F
- the invention relates to an i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) an immune check point inhibitor for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
- TfRl antibody anti- transferrin receptor 1
- iron chelator an iron chelator
- immune check point inhibitor for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
- administering refers to the act of injecting or otherwise physically delivering a substance as it exists outside the body (e.g., an antibody anti-TfRl and an iron chelator) into the subject, such as by mucosal, intradermal, intravenous, subcutaneous, intramuscular delivery and/or any other method of physical delivery described herein or known in the art.
- a disease, or a symptom thereof is being treated, administration of the substance typically occurs after the onset of the disease or symptoms thereof.
- administration of the substance typically occurs before the onset of the disease or symptoms thereof.
- a “therapeutically effective amount” is meant a sufficient amount of an antibody anti- TfRl for use in a method for the treatment of melanoma at a reasonable benefit/risk ratio applicable to any medical treatment. It will be understood that the total daily usage of the compounds and compositions of the present invention will be decided by the attending physician within the scope of sound medical judgment.
- the specific therapeutically effective dose level for any particular subject will depend upon a variety of factors including the age, body weight, general health, sex and diet of the subject; the time of administration, route of administration, and rate of excretion of the specific compound employed; the duration of the treatment; drugs used in combination or coincidental with the specific polypeptide employed; and like factors well known in the medical arts.
- the daily dosage of the products may be varied over a wide range from 0.01 to 1,000 mg per adult per day.
- the compositions contain 0.01, 0.05, 0.1, 0.5, 1.0, 2.5, 5.0, 10.0, 15.0, 25.0, 50.0, 100, 250 and 500 mg of the active ingredient for the symptomatic adjustment of the dosage to the subject to be treated.
- a medicament typically contains from about 0.01 mg to about 500 mg of the active ingredient, typically from 1 mg to about 100 mg of the active ingredient.
- An effective amount of the drug is ordinarily supplied at a dosage level from 0.0002 mg/kg to about 20 mg/kg of body weight per day, especially from about 0.001 mg/kg to 7 mg/kg of body weight per day.
- the invention relates to an i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) an immune check point inhibitor, for use in the treatment of resistant cancer, as a combined preparation.
- TfRl antibody anti- transferrin receptor 1
- iron chelator an iron chelator
- immune check point inhibitor an immune check point inhibitor
- the terms“combined treatment”,“combined therapy” or“therapy combination” refer to a treatment that uses more than one medication.
- the combined therapy may be dual therapy or bi-therapy.
- the i) antibody-anti TfRl and ii) the iron chelator as a combined preparation according to the invention for simultaneous, separate or sequential use in the method for treating.
- the term“simultaneous use” refers to an administration of 2 active ingredients by the same route and at the same time or at substantially the same time.
- the term “separate use” refers to an administration of 2 active ingredients at the same time or at substantially the same time by different routes.
- the term “sequential use” refers to an administration of 2 active ingredients at different times, the administration route being identical or different.
- the i) anti-TfRl antibody and ii) the iron chelator as described above may be combined with pharmaceutically acceptable excipients, and optionally sustained-release matrices, such as biodegradable polymers, to form pharmaceutical compositions.
- pharmaceutically acceptable excipients such as biodegradable polymers
- pharmaceutically acceptable carrier or excipient refers to a non-toxic solid, semi-solid or liquid filler, diluent, encapsulating material or formulation auxiliary of any type.
- compositions of the present invention for oral, sublingual, subcutaneous, intramuscular, intravenous, transdermal, local or rectal administration can be administered in a unit administration form, as a mixture with conventional pharmaceutical supports, to animals and human beings.
- Suitable unit administration forms comprise oral-route forms such as tablets, gel capsules, powders, granules and oral suspensions or solutions, sublingual and buccal administration forms, aerosols, implants, subcutaneous, transdermal, topical, intraperitoneal, intramuscular, intravenous, subdermal, transdermal, intrathecal and intranasal administration forms and rectal administration forms.
- the pharmaceutical compositions contain vehicles which are pharmaceutically acceptable for a formulation capable of being injected.
- vehicles which are pharmaceutically acceptable for a formulation capable of being injected.
- These may be in particular isotonic, sterile, saline solutions (monosodium or disodium phosphate, sodium, potassium, calcium or magnesium chloride and the like or mixtures of such salts), or dry, especially freeze-dried compositions which upon addition, depending on the case, of sterilized water or physiological saline, permit the constitution of injectable solutions.
- the pharmaceutical forms suitable for injectable use include sterile aqueous solutions or dispersions; formulations including sesame oil, peanut oil or aqueous propylene glycol; and sterile powders for the extemporaneous preparation of sterile injectable solutions or dispersions.
- the form In all cases, the form must be sterile and must be fluid to the extent that easy syringability exists. It must be stable under the conditions of manufacture and storage and must be preserved against the contaminating action of microorganisms, such as bacteria and fungi.
- Solutions comprising compounds of the invention as free base or pharmacologically acceptable salts can be prepared in water suitably mixed with a surfactant, such as hydroxypropylcellulose. Dispersions can also be prepared in glycerol, liquid polyethylene glycols, and mixtures thereof and in oils. Under ordinary conditions of storage and use, these preparations contain a preservative to prevent the growth of microorganisms.
- the polypeptide (or nucleic acid encoding thereof) can be formulated into a composition in a neutral or salt form.
- Pharmaceutically acceptable salts include the acid addition salts (formed with the free amino groups of the protein) and which are formed with inorganic acids such as, for example, hydrochloric or phosphoric acids, or such organic acids as acetic, oxalic, tartaric, mandelic, and the like. Salts formed with the free carboxyl groups can also be derived from inorganic bases such as, for example, sodium, potassium, ammonium, calcium, or ferric hydroxides, and such organic bases as isopropylamine, trimethylamine, histidine, procaine and the like.
- the carrier can also be a solvent or dispersion medium containing, for example, water, ethanol, polyol (for example, glycerol, propylene glycol, and liquid polyethylene glycol, and the like), suitable mixtures thereof, and vegetables oils.
- the proper fluidity can be maintained, for example, by the use of a coating, such as lecithin, by the maintenance of the required particle size in the case of dispersion and by the use of surfactants.
- the prevention of the action of microorganisms can be brought about by various antibacterial and antifungal agents, for example, parabens, chlorobutanol, phenol, sorbic acid, thimerosal, and the like.
- isotonic agents for example, sugars or sodium chloride.
- Prolonged absorption of the injectable compositions can be brought about by the use in the compositions of agents delaying absorption, for example, aluminium monostearate and gelatin.
- Sterile injectable solutions are prepared by incorporating the active polypeptides in the required amount in the appropriate solvent with several of the other ingredients enumerated above, as required, followed by filtered sterilization.
- dispersions are prepared by incorporating the various sterilized active ingredients into a sterile vehicle which contains the basic dispersion medium and the required other ingredients from those enumerated above.
- sterile powders for the preparation of sterile injectable solutions
- the preferred methods of preparation are vacuum drying and freeze-drying techniques which yield a powder of the active ingredient plus any additional desired ingredient from a previously sterile-filtered solution thereof.
- solutions will be administered in a manner compatible with the dosage formulation and in such amount as is therapeutically effective.
- the formulations are easily administered in a variety of dosage forms, such as the type of injectable solutions described above, but drug release capsules and the like can also be employed.
- the solution should be suitably buffered if necessary and the liquid diluent first rendered isotonic with sufficient saline or glucose.
- aqueous solutions are especially suitable for intravenous, intramuscular, subcutaneous and intraperitoneal administration.
- sterile aqueous media which can be employed will be known to those of skill in the art in light of the present disclosure.
- one dosage could be dissolved in 1 ml of isotonic NaCl solution and either added to 1000 ml of hypodermoclysis fluid or inj ected at the proposed site of infusion. Some variation in dosage will necessarily occur depending on the condition of the subject being treated. The person responsible for administration will, in any event, determine the appropriate dose for the individual subject.
- the invention relates to a pharmaceutical composition comprising the combined preparation according to the invention.
- the pharmaceutical composition according to the invention for use in the treatment of cancer.
- the pharmaceutical composition according to the invention for use in the treatment of resistant cancer.
- FIGURES are a diagrammatic representation of FIGURES.
- Figure 1 The effect of the combination of H7 with DFO or DFX on the cell viabilities of PDAC cells.
- BxPC3 and CFPAC cells were plated, 24hrs later they were treated with either DFO (3mM) or DFX (4 mM) alone or with increasing concentrations of H7 alone ranging from (0.3 pg/ml to 2pg/ml) or with the combination (H7 and DFO at 3 mM) or (H7 and DFX 4 pM). After 5 days cell viability was assessed using the MTS assay (cellTiter 96, Promega).
- DFO DFO
- DFX 4 mM
- HP AC cells in DMEM medium were plated and treated the next day with either DFO alone at 0.5 or 1 pM or increasing concentrations of H7 as indicated in A or combinations with different H7 concentrations and DFO at 0.5 or 1 pM 5 days after treatment cell viability is assessed by MTS.
- Figure 2 H7, DFO, and DFX dose response curves on BxPC3 and CFPAC cells (A,B,C). PDAC cells were plated, 24hrs later H7, DFO, or DFX were added with increasing concentrations. After 5 days cell viability was assessed using MTS assay (cellTiter 96, Promega). Effect of the combination of H7 and DFO or DFX on cell viability (D,E).
- BxPC3 and CFPAC cells were plated, 24hrs later they were treated with either DFO (3mM) or DFX (4 mM) alone or with increasing concentrations of H7 alone ranging from (0.3 pg/ml to 2pg/ml) or with the combination (H7 and DFO at 3 mM) or (H7 and DFX 4 mM). After 5 days cell viability was assessed using the MTS assay (cellTiter 96, Promega).
- Figure 3 Effect of the combination of H7 with DFO (A) or DFX (B) on the cell cycle phase repartition of BxPC3 and CFPAC cells. After 24 hours of plating, cells were treated for 3 days with either H7 (2 pg/ml), DFO (3 mM), DFX (2 mM), the combination of H7 at 2 pg/ml with DFO 3 mM or the combination of H7 (2 pg/ml) and DFX (2 mM). Cells were then stained with PI before FACS analysis. Combination of H7 and iron chelator treatment synergizes to block cell cycle progression in D phase.
- Figure 4 Effect of the combination of H7 with DFO (A) or DFX (B) on apoptosis of BxPC3 and CFPAC cells. After 24 hours of plating, cells were treated for 5 days with either H7 (2 pg/ml), with DFO (3 pM), DFX (2 pM), combination of H7 (2 pg/ml) with DFO 3 pM, or combination of H7 (2 pg/ml) and DFX (2 pM). Cells were then stained with AnnexinV- FITC and 7AAD before FACS analysis. Early (Annexin positive) and late apoptosis (Annexin positive 7AAD positive) are presented. The association of H7 treatment with an iron chelator increases apoptosis induction in both cell lines compared to single treatment.
- Figure 5 Effect of iron chelators on holo-Tf-Alexa 488 uptake of the CFPAC cell line.
- Non confluent CFPAC cells were incubated with 500 nM holoTf conjugated to Alexa 488 and either left untreated or treated with DFO or DFX (100 pM), non fluorescent holoTf (10 mM), or H7 at 45 nM for 4 hrs at 37°C.
- Internalized fluorescence was measured by FACS and the results are shown as the % holoTf uptake relative to NT.
- an excess of holo-Tf blocks as expected fluorescent holo-Tf uptake, like the competitor H7.
- Iron chelators do not reduce fluorescent holo-Tf uptake consistent with their inability to chelate iron from holo-Tf. If it was the case, holo-Tf would be converted in iron free Tf (apo-Tf) that has low affinity for TfRl, therefore, fluorescence intensity of the cells would be reduced.
- FIG. 6 Viability of CFPAC cell treated with H7, DFO, or DFX combined or not with Ferric ammonium citrate.
- Cells were either non treated (NT) or treated as indicated for 5 days and cell viability is then measured by MTS (cell Titer, 96).
- FAC in excess (free iron) reverses the viability decrease observed with iron chelators as expected, but also viability decrease observed with H7 likely by an increase of uptake of free iron.
- holo-Tf in excess reverses as expected the viability decrease obtained with H7, but also with the decrease of viability observed with iron chelators, likely by an increase of holo-Tf uptake. This shows that the two mechanism of iron uptake are independent.
- Figure 7 In vivo effect of H7 and DFX combination on BxPC3 PDAC growth in nude mice.
- BxPC3 cells s.c. were grafted in nude mice.
- Established tumors were either treated with NaCl, H7 at 5 mg/kg twice a week, i.p., DFX 40 mg/kg by gavage, 3 times a week or combination of the 2 treatments for 4 weeks (from day 20 to day 48). Mice were sacrificed when their tumor reached 1500 mm3. Tumor size was plotted in function of the time (day) after graft.
- the HP AC cell line is resistant to H7 treatment in DMEM medium due to the presence of iron in this medium (0.25 mM ferric nitrate) which can reverse the effect of the antibody as mentioned earlier in the complementary results.
- Figure IB shows that adding a very low concentration of DFO 0.5 mM or 1 mM (at which DFO shows no effect by itself) to H7, the HP AC cell line becomes sensitive to H7 treatment showing a decrease in cell viability by 40%. Because at these concentrations both H7 and DFO are not effective, it seems there is a synergistic effect for this combination, probably DFO binding iron in the medium and thus allowing H7 to decrease cell viability by blocking holoTf uptake.
- H7 (2 pg/ml) combination with DFO (3 pM) induced a strong increase in the percentage of cells in the S phase (data not shown). This was also accompanied with an increase in subGl phase (apoptotic cells) indicating that after 3 days some of the cells are dying.
- subGl phase apoptotic cells
- the same combination lead to an S phase arrest more probably at the early S phase or the Gl/S boundary and an increase in cells in SubGl phase as well (data not shown).
- PDAC cells are more sensitive to apoptosis induction when H7 is combined with DFO or DFX
- H7 as well as DFO induce NDRG1 expression on the BxPC3 and CFPAC cell lines (data not shown).
- DFO at 10 mM as a positive control for the induction of NDRG1 (data not shown).
- PDAC cells were plated, 24hrs later H7, DFO, or DFX were added with increasing concentrations. After 5 days cell viability was assessed using MTS assay (cellTiter 96, Promega). Effect of the combination of H7 and DFO or DFX on cell viability (D,E). BxPC3 and CFPAC cells were plated, 24hrs later they were treated with either DFO (3mM) or DFX (4 mM) alone or with increasing concentrations of H7 alone ranging from (0.3 pg/ml to 2pg/ml) or with the combination (H7 and DFO at 3 mM) or (H7 and DFX 4 mM). After 5 days cell viability was assessed using the MTS assay (cellTiter 96, Promega). An additive effect on cell viability decrease is obtained with the combination treatment ( Figure 2D-E).
- H7 H7 (2 pg/ml), DFO (3 mM), DFX (2 mM), the combination of H7 at 2 pg/ml with DFO 3 mM or the combination of H7 (2 pg/ml) and DFX (2 mM).
- Cells were then stained with PI before FACS analysis.
- Combination of H7 and iron chelator treatment synergizes to block cell cycle progression in D phase ( Figure 3).
- H7 H7 (2 pg/ml), with DFO (3 pM), DFX (2 pM), combination of H7 (2 pg/ml) with DFO 3 pM, or combination of H7 (2 pg/ml) and DFX (2 pM).
- Cells were then stained with AnnexinV- FITC and 7AAD before FACS analysis. Early (Annexin positive) and late apoptosis (Annexin positive 7AAD positive) are presented.
- the association of H7 treatment with an iron chelator increases apoptosis induction in both cell lines compared to single treatment ( Figure 4). 9) Effect of iron chelators on holo-Tf-Alexa 488 uptake of the CFPAC cell line.
- Non confluent CFPAC cells were incubated with 500 nM holoTf conjugated to Alexa 488 and either left untreated or treated with DFO or DFX (100 mM), non fluorescent holoTf (10 mM), or H7 at 45 nM for 4 hrs at 37°C. Internalized fluorescence was measured by FACS and the results are shown as the % holoTf uptake relative to NT.
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Medicinal Chemistry (AREA)
- General Health & Medical Sciences (AREA)
- Veterinary Medicine (AREA)
- Immunology (AREA)
- Pharmacology & Pharmacy (AREA)
- Organic Chemistry (AREA)
- Animal Behavior & Ethology (AREA)
- Public Health (AREA)
- Epidemiology (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Genetics & Genomics (AREA)
- Engineering & Computer Science (AREA)
- General Chemical & Material Sciences (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Microbiology (AREA)
- Endocrinology (AREA)
- Biochemistry (AREA)
- Mycology (AREA)
- Biophysics (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Molecular Biology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Medicines Containing Antibodies Or Antigens For Use As Internal Diagnostic Agents (AREA)
- Peptides Or Proteins (AREA)
Abstract
Inventors hypothesis is that combining iron chelators and an anti- transferrin receptor 1 (TfRI) antibody such as H7, each acting on a separate iron source (chelators on the LIP and iron stored in ferritin of cancer cells) and H7 (iron from internalized holo-Tf), can improve the iron deprivation efficiency in the iron avid cancer cells. Inventors have chosen DFO and DFX as iron chelators in this study since, besides the fact that they are used in the clinic, they have different characteristics. They used the BxPC3, CFPAC, and HPAC cell lines to study the effects of these combinations on cell viability, apoptosis, cell cycle, and NDRGI induction and compared these effects to the single treatments. Preliminary data obtained recently on 3D cultures of the BxPC3 cell line confirmed the increased effect of DFX and H7 combinations on cell viability compared to single treatment alone. Accordingly, the invention relates to i) an anti- transferrin receptor 1 (TfRI) antibody and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of cancers.
Description
COMPOSITIONS FOR TREATING CANCERS AND RESISTANT CANCERS
FIELD OF THE INVENTION:
The invention is in the field of cancerology. More particularly, the invention relates to use of anti-transferrin receptor 1 antibodies and ion chelators, as a combined preparation for use in the treatment of cancers and resistant cancers.
BACKGROUND OF THE INVENTION:
Iron deprivation is an emerging strategy in cancer therapeutics. Tumors have high iron content and rely on iron for their growth and progression1. Cancer stem cells also require iron for their survival 2 3. Iron levels in cells can be reduced with iron chelators4 which are already used in the clinic for iron overload disorders. Transferrin receptor 1 (TfRl) is the main receptor responsible for the cell iron supply through receptor-mediated internalization of serum Fe3+- loaded transferrin (holo-Tf). Within the cell, Fe3+ is released, reduced, excluded from the early endosome by divalent metal ion transporter 1 (DMT1), and used for cell metabolism. Fe3+ excess is stored in ferritin, while TfRl is recycled at the cell surface together with iron-free transferrin (apo-Tf)5. Iron chelators are iron binding molecules that bind iron and block its function. They are principally used in the treatment of iron overload diseases.
TfRl is ubiquitously expressed at low levels by almost all cells. However, higher levels exist on cells that need large amounts of iron such as maturing erythroid precursor cells which require iron for hemoglobin synthesis. Nevertheless, TfRl is not expressed on pluripotent hematopoietic stem cells and on mature erythrocytes (Gross et al., 1997). TfRl-knock out mice exhibit severe anemia and die by embryonic day 12.5. High TfRl expression is reported on placental trophoblasts which need the TfRl to transport iron to maturing erythroid precursor cells. High TfRl is also present on rapidly proliferating cells including the intestinal epithelium, the basal epidermis and activated lymphocytes (Haynes et al., 1981; Gatter et al., 1983). TfRl is expressed as well on the endocrine pancreas, vascular endothelium of brain capillaries (blood brain barrier), seminiferous tubules of the testes, breast luminal membranes, pituitary cells, kuppfer cells of liver, kidney tubules, and hepatocytes (Gatter et al., 1983).
Cancer cells need more iron than normal cells and they express higher TfRl levels. For example, breast cancer cells show 4-5 fold higher TfRl level than normal breast cells (Walker
and Day, 1986). A higher rate of recurrence was correlated with high TfRl expression in primary bladder malignancies (Smith et al., 1990). Higher TfRl correlated with the tumor grade and prognosis in non hodgkin’s lymphoma, lung adenocarcinoma, breast cancer, gliomas, and chronic lyphocytic leukemias (Habeshaw et al., 1983; Kondo et al., 1990; Yang et al., 2001; Prior et al., 1990; Das Gupta and Shah, 1990).
Accordingly, there is a need to find new tools to treat cancers and resistant cancers dependent of iron metabolism.
SUMMARY OF THE INVENTION:
The invention relates to i) an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of cancers. In particular, the invention is defined by the claims.
DETAILED DESCRIPTION OF THE INVENTION:
In cancer, cancer cells are proliferating rapidly and require higher iron levels than normal cells representing a good target for iron chelators. Inventors hypothesis is that combining iron chelator and an antibody anti- transferrin receptor 1 (TfRl) such as H7 with each acting on a separate iron source (chelators on the LIP and iron stored in ferritin of cancer cells) and H7 (iron from internalized holo-Tf), they can improve the iron deprivation efficiency in the iron avid cancer cells.
Inventors have chosen DFO and DFX as iron chelators in this study since, besides the fact that they are used in the clinic, they have different characteristics. DFO is not liposoluble, it can nevertheless enter slowly into the cells and localize merely in the cytosol (Hoyes and Porter, 1993) while DFX is liposoluble and has access to intracellular organelles in addition to the cytosol (Glickstein et al., 2005). Redox properties of iron are different for the 2 chelators, totally neutralized by the hexadentate iron chelator DFO but not with the tridentate chelator DFX.
They used the BxPC3, CFPAC, and HP AC cell lines to study the effects of these combinations on cell viability, apoptosis, cell cycle, and NDRG1 induction and compare these effects to the single treatments.
Preliminary data that they obtained recently on 3D cultures of BxPC3 cell line confirmed the increased effect of DFX and H7 combinations on cell viability compared to single treatment alone. The advantages of this combination is that low concentrations of iron chelators
can be used thus avoiding the potential toxic effects associated with iron chelators. Although by using H7 they are targeting the main route of iron supply however the presence of other iron uptake mechanisms is always a concern with using anti-TfRl antibody. Therefore, the combination of iron chelators which binds iron directly, in the extracellular fluids in vivo and intracellular iron (from iron in the LIP and ferritin turnover), with holoTf uptake blockade potentially leads to better iron deprivation and thus better effects.
Accordingly, inventors have shown that the combination of iron chelators with an anti transferrin receptor 1 antibody has the characteristics and qualifications that allow it to be tried in clinical trials.
In a first aspect, the invention relates to an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of cancers.
More particularly, the invention relates to a method for treating cancer and resistant cancers in a subject in need thereof comprising a step of administering said subject with a therapeutically amount of i)an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation.
As used herein, the terms“treating” or“treatment” refer to both prophylactic or preventive treatment as well as curative or disease modifying treatment, including treatment of subject at risk of contracting the disease or suspected to have contracted the disease as well as subject who are ill or have been diagnosed as suffering from a disease or medical condition, and includes suppression of clinical relapse. The treatment may be administered to a subject having a medical disorder or who ultimately may acquire the disorder, in order to prevent, cure, delay the onset of, reduce the severity of, or ameliorate one or more symptoms of a disorder or recurring disorder, or in order to prolong the survival of a subject beyond that expected in the absence of such treatment. By "therapeutic regimen" is meant the pattern of treatment of an illness, e.g., the pattern of dosing used during therapy. A therapeutic regimen may include an induction regimen and a maintenance regimen. The phrase "induction regimen" or "induction period" refers to a therapeutic regimen (or the portion of a therapeutic regimen) that is used for the initial treatment of a disease. The general goal of an induction regimen is to provide a high level of drug to a subject during the initial period of a treatment regimen. An induction regimen
may employ (in part or in whole) a "loading regimen", which may include administering a greater dose of the drug than a physician would employ during a maintenance regimen, administering a drug more frequently than a physician would administer the drug during a maintenance regimen, or both. The phrase "maintenance regimen" or "maintenance period" refers to a therapeutic regimen (or the portion of a therapeutic regimen) that is used for the maintenance of a subject during treatment of an illness, e.g., to keep the subject in remission for long periods of time (months or years). A maintenance regimen may employ continuous therapy (e.g., administering a drug at a regular intervals, e.g., weekly, monthly, yearly, etc.) or intermittent therapy (e.g., interrupted treatment, intermittent treatment, treatment at relapse, or treatment upon achievement of a particular predetermined criteria [e.g., pain, disease manifestation, etc.]).
As used herein, the term“subject” denotes a mammal, such as a rodent, a feline, a canine, and a primate. Particularly, the subject according to the invention is a human. More particularly, the subject according to the invention has or susceptible to have a cancer. In a particular embodiment, the subject according to the invention has or susceptible to have a pancreatic cancer. More particularly, the subject according to the invention has or susceptible to have a pancreatic ductal adenocarcinoma (PD AC).
As used herein, the term“cancer” refers to an abnormal cells divide without control and can invade nearby tissues. Cancer cells can also spread to other parts of the body through the blood and lymph systems. There are several main types of cancer. In the context of the invention, the term“cancers” relates to cancers which absorb iron. More particularly, iron uptake by transferrin receptor is the most important way for cancer cells to absorb iron which in required for their survival. Typically, the cancer is selected from the following group but not limited to: pancreatic cancer, neuroblastoma, solid cancer, leukemia, lymphoma, glioblastoma, breast cancer, cancer related cachexia, gastrointestinal cancer such as colorectal cancer, cholangiocarcinoma, carcinoma of the oral cavity, gastric cancer, lung cancer such as small cell lung cancer, lung adenocarcinoma, melanoma, multiple myeloma, ovarian cancer, prostate cancer, renal cancer, hepatocarcinoma.
More particularly, the cancer is pancreatic cancer. There are different types of pancreatic cancer. They are divided into two main groups, based on the different types of cells found in the pancreas. Exocrine tumours start in the exocrine cells, where enzymes that help to digest food are made. 96% pancreatic cancers are exocrine tumours. The most common type of pancreatic cancer, pancreatic ductal adenocarcinoma (PDAC), is an exocrine tumour.
Neuroendocrine tumours start in the neuroendocrine cells. These cells produce hormones that help control the normal functions of the body. For example, they produce insulin which helps to control the level of sugar in the blood. These tumours are known as pancreatic neuroendocrine tumours or PancNETs.
In a particular embodiment, the cancer is pancreatic ductal adenocarcinoma (PDAC). Pancreatic ductal adenocarcinoma (PDAC) is a type of exocrine pancreatic cancer. It is the most common type of pancreatic cancer 95% of all pancreatic cancers are PDAC. PDAC develops from cells lining small tubes in the pancreas called ducts (duct cells in the diagram above). These carry the digestive juices, which contain enzymes, into the main pancreatic duct and then on into the duodenum (first part of the small intestine). PDAC can grow anywhere in the pancreas, though it is most often found in the head of the pancreas. Symptoms can include tummy (abdominal) and back pain, weight loss and changes to bowel habits.
As used herein, the term“transferrin receptor” refers to a membrane transport protein which is involved in iron uptake in vertebrates. It imports iron by internalizing the transferrin- iron complex through receptor-mediated endocytosis. There are two types of transferrin receptors: transferrin receptor protein 1 (TfRl) and Transferrin receptor 2 (TfR2). In the context of the invention, the transferrin receptor is transferrin receptor protein 1 (TfRl) also known as Cluster of Differentiation 71 (CD71). TfRl is a transmembrane glycoprotein composed of two disulfide-linked monomers joined by two disulfide bonds.
As used herein, the term“antibody” is used in the broadest sense and specifically covers monoclonal antibodies, polyclonal antibodies, multispecific antibodies (e.g. bispecific antibodies) formed from at least two intact antibodies, and antibody fragments so long as they exhibit the desired biological activity of TfRl . Typically, such antibody inhibits the iron transport in the tumour cells.
The term includes antibody fragments that comprise an antigen binding domain such as Fab', Fab, F(ab')2, single domain antibodies (DABs), TandAbs dimer, Fv, scFv (single chain Fv), dsFv, ds-scFv, Fd, linear antibodies, minibodies, diabodies, bispecific antibody fragments, bibody, tribody (scFv-Fab fusions, bispecific or trispecific, respectively); sc-diabody; kappa(lamda) bodies (scFv-CL fusions); BiTE (Bispecific T-cell Engager, scFv-scFv tandems to attract T cells); DVD-Ig (dual variable domain antibody, bispecific format); SIP (small immunoprotein, a kind of minibody); SMIP ("small modular immunopharmaceutical" scFv-Fc dimer; DART (ds-stabilized diabody "Dual Affinity ReTargeting"); small antibody mimetics
comprising one or more CDRs and the like. The techniques for preparing and using various antibody-based constructs and fragments are well known in the art (see Kabat et ah, 1991, specifically incorporated herein by reference). Diabodies, in particular, are further described in EP 404, 097 and WO 93/1 1 161; whereas linear antibodies are further described in Zapata et al. (1995). Antibodies can be fragmented using conventional techniques. For example, F(ab')2 fragments can be generated by treating the antibody with pepsin. The resulting F(ab')2 fragment can be treated to reduce disulfide bridges to produce Fab' fragments. Papain digestion can lead to the formation of Fab fragments. Fab, Fab' and F(ab')2, scFv, Fv, dsFv, Fd, dAbs, TandAbs, ds-scFv, dimers, minibodies, diabodies, bispecific antibody fragments and other fragments can also be synthesized by recombinant techniques or can be chemically synthesized. Techniques for producing antibody fragments are well known and described in the art. For example, each of Beckman et al., 2006; Holliger & Hudson, 2005; Le Gall et al., 2004; Reff & Heard, 2001 ; Reiter et al., 1996; and Young et al., 1995 further describe and enable the production of effective antibody fragments. In some embodiments, the antibody is a“chimeric” antibody as described in U.S. Pat. No. 4,816,567. In some embodiments, the antibody is a humanized antibody, such as described U.S. Pat. Nos. 6,982,321 and 7,087,409. In some embodiments, the antibody is a human antibody. A“human antibody” such as described in US 6,075, 181 and 6, 150,584. In some embodiments, the antibody is a single domain antibody such as described in EP 0 368 684, WO 06/030220 and WO 06/003388.
In a particular embodiment, the antibody is a monoclonal antibody. Monoclonal antibodies can be prepared and isolated using any technique that provides for the production of antibody molecules by continuous cell lines in culture. Techniques for production and isolation include but are not limited to the hybridoma technique, the human B-cell hybridoma technique and the EBV-hybridoma technique.
In a particular embodiment, the antibody anti-TfRl is conjugated to the drugs. Said antibody is called as antibody drug conjugate (ADC). In a particular embodiment, such antibody is combined with the potency of chemotherapeutic agents. The technology associated with the development of monoclonal antibodies to tumor associated target molecules, the use of more effective cytotoxic agents, and the design of chemical linkers to covalently bind these components, has progressed rapidly in recent years (Ducry L, et a/. Bioconjugate Chemistry, 21 :5-13, 2010).
In a particular embodiment, the antibody anti-TfRl is able to induce cytotoxicity, also known as the antibody-dependent cell-mediated cytotoxicity (ADCC). ADCC is a mechanism of cell-mediated immune defense whereby an effector cell of the immune system actively lyses a target cell, whose membrane-surface antigens have been bound by specific antibodies.
Three highly divergent stretches within the variable region of the heavy and light chains are referred to as“hypervariable regions” which are interposed between more conserved flanking stretches known as“framework region” or“FRs”. Thus the term“FR” refers to amino acid sequences which are naturally found between and adjacent to hypervariable region. In an antibody molecule, three hypervariable regions of a light chain and three hypervariable regions of a heavy chain are disposed relative to each other in three dimensional space to form an antigen binding surface. This surface mediates recognition and binding of the target antigen. The three hypervariable regions of each of the heavy and light chain are referred to as “complementary determining regions” or“CDRs” and are characterized, for example by Rabat et al.
Typically, the residues in antibody variable domains are conventionally numbered according to a system devised by Rabat et al. This system is set forth in Rabat et al., 1987, in Sequences of Proteins of Immunological Interest, US Department of Health and Human Services, NIH, USA (hereafter“Rabat et al”). This numbering system is used in the present specification. The Rabat residue designations do not always correspond directly with the linear numbering of the amino acid residues in SEQ ID sequences. The actual linear amino acid sequence may contain fewer or additional amino acids than in the strict Rabat numbering corresponding to a shortening of, or insertion into, a structural component, whether framework or complementarity determining region (CDR), of the basic variable domain structure. The correct Rabat numbering of residues may be determined for a given antibody by alignment of residues of homology in the sequence of the antibody with a“standard” Rabat numbered sequence. The CDRs of the heavy chain variable domain are located at residues 31-35B (H- CDR1), residues 50-65 (H-CDR2) and residues 95-102 (H-CDR3) according to the Rabat numbering system. The CDRs of the light chain variable domain are located at residues 24-34 (L-CDR1), residues 50-56 (L-CDR2) and residues 89-97 (L-CDR3) according to the Rabat numbering system. (htp://www.bioiiif.org.Uk/abs/#cdrdef). According to the invention, the CDR of the antibodies of the invention are in the Rabat nomenclature.
In the context of the invention, the antibody for use according to the invention, wherein said antibody is an anti-TfRl antibody chosen among H7, F12, C32, F2, H9, G9.
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is H7 (SEQ ID NO: 1).
In a particular embodiment, the H7 antibody has the following sequences as described below:

Table 1 : sequences of H7 antibody
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is H7 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:2, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:3, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:4, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:5; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:6, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:7.
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is F12 antibody (SEQ ID NO: 10).
In a particular embodiment, the F12 antibody has the following sequences as described below:

Table 2: sequences of F12 antibody
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is F12 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO: 11, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO: 12, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO: 13, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO: 14; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO: 15, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO: 16.
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is C32 antibody (SEQ ID NO: 19).
In a particular embodiment, the C32 antibody has the following sequences as described below:

Table 3 : sequences of C32 antibody
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is C32 antibody comprising: a) a heavy chain CDR1 comprising the amino acid
sequence of SEQ ID NO:20, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:21, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:22, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:23; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:24, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:25.
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is F2 antibody (SEQ ID NO: 28).
In a particular embodiment, the F2 antibody has the following sequences as described below:

Table 4: sequences of F2 antibody
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is F2 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:29, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:30, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:31, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:32; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:33, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:34.
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is H9 antibody (SEQ ID NO: 37).
In a particular embodiment, the H9 antibody has the following sequences as described below:

Table 5 : sequences of H9 antibody
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is H9 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:38, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:39, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:40, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:41 ; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:42, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:43.
The antibody for use according to the invention, wherein said antibody is G9 antibody (SEQ ID NO: 46). In a particular embodiment, the H9 antibody has the following sequences as described below:
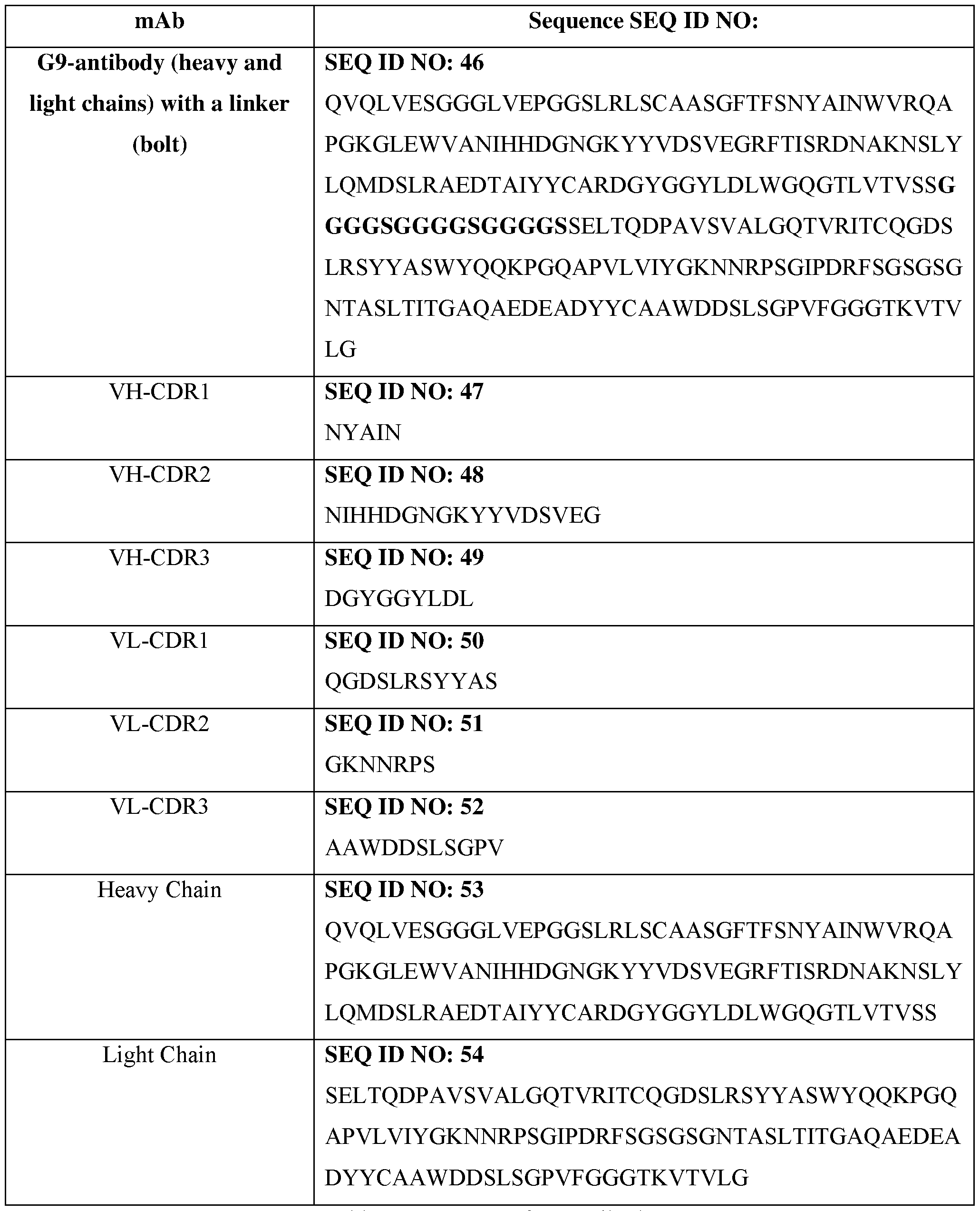
Table 6: sequences of G9 antibody
In a particular embodiment, the antibody for use according to the invention, wherein said antibody is G9 antibody comprising a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:47, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:48, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:49, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:50; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:51, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:52.
As used herein, the term“iron chelator” refers to synthetic and natural iron chelators which chelate iron. Chelation is a type of bonding of ions and molecules to metal ion. Chelation therapy is used as nutritional supplement, dental and oral application, heavy-metal detoxification, and as pharmaceuticals. Iron-chelation therapy has its origins in the treatment of iron-overload syndromes. In the context of the invention, the iron chelator is used in combination with an anti-transferrin receptor 1 antibody as described above. Iron chelators are well-known in the art and include but not limited to: Deferoxamine (Desferal®, DFO), Desferrithiocinn (DFT), Deferiprone (Ferriprox®), 8-hydroxy quinoline derivatives, Deferasirox (ICL670; Exjade®, DFX), Tachpyridin, Dexrazone (ICRF-197; DZR), Thiosemicarbazones, Pyridoxal isonicotinoyl hydrazone analogs, phytochemicals (Proanthocyanidins, epicatechins, flavonols and anthocyanin), Herbal remedies (curcumin, Kolaviron, Pycnogenol™, Baicalein and its glycoside baicalin, Tetramethylpyrazine and ferulic acid).
In the context of the invention, the iron chelator is Deferoxamine (DFO). It is a natural product produced by the bacterium, Streptomyces pilosus. It was the first chelator introduced in the clinic for iron overload treatment. It is a hexadentade chelator that binds selectively ferric Fe3+ with high affinity forming a 1 : 1 complex Deferoxamine acts by binding free iron in the bloodstream and enhancing its elimination in the urine. DFO is commercialized as Desferal®, by Novartis. The chemical formula of DFO is: C25H48N608. DFO refers to Butanedi amide, N'-[5-[[4-[[5-(acetylhydroxyamino)pentyl]amino]-l,4-dioxobutyl]hydroxyamino]pentyl]-N- (5-aminopentyl)-N-hydroxy and has the following structure (formula I) and CAS number: 70- 51-9:

In another embodiment, the iron chelator is Deferasirox (DFX). It is a synthetic tridentate iron chelator that binds Fe3+ iron and forms a 2: 1 ligand to iron complex allowing iron to catalyze redox reactions. It is commercialized as Exjade by Novartis. The cas number of DFX is 201530-41-8. DFX has the following chemical formula C21H15N304 and structure (formula II) in the art: Benzoic acid, 4-[3,5-bis(2-hydroxyphenyl)-lH-l,2,4-triazol-l-yl]-:

Formula II
As used herein, the term“simultaneous use” refers to an administration of 2 active ingredients by the same route and at the same time or at substantially the same time. The term “separate use” refers to an administration of 2 active ingredients at the same time or at substantially the same time by different routes. The term “sequential use” refers to an administration of 2 active ingredients at different times, the administration route being identical or different.
The combination as described above is suitable to treat resistant cancers.
Accordingly, in a second aspect, the invention relates to i)an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of resistant cancers.
As used herein, the term“resistant cancers” refers to a cancer that does not respond to treatment notably to convention therapies (chemotherapy, radiotherapy etc). In a particular embodiment, the cancer is resistant at the beginning of treatment. In another embodiment, the cancer become resistant during treatment, such cancer is called refractory cancer.
As used herein, the term“subject” denotes a mammal, such as a rodent, a feline, a canine, and a primate. Particularly, the subject according to the invention is a human. More particularly, the subject according to the invention has or susceptible to have resistant cancer.
In a particular embodiment, the resistant cancer is selected from the group consisting of but not limited to pancreatic cancer, neuroblastoma, leukemia, lymphoma, glioblastoma, colon cancer.
In another embodiment, the cancer is resistant to rituximab. Rituximab is a chimeric monoclonal antibody against the protein CD20.
In another embodiment, the cancer is resistant to an immune check point inhibitor.
As used herein, the term "immune checkpoint inhibitor" refers to molecules that totally or partially reduce, inhibit, interfere with or modulate one or more immune checkpoint proteins.
As used herein, the term "immune checkpoint protein" has its general meaning in the art and refers to a molecule that is expressed by T cells in that either turn up a signal (stimulatory checkpoint molecules) or turn down a signal (inhibitory checkpoint molecules). Immune checkpoint molecules are recognized in the art to constitute immune checkpoint pathways similar to the CTLA-4 and PD-1 dependent pathways (see e.g. Pardoll, 2012. Nature Rev Cancer 12:252-264; Mellman et al. , 2011. Nature 480:480- 489). Examples of stimulatory checkpoint include CD27 CD28 CD40, CD122, CD137, 0X40, GITR, and ICOS. Examples of inhibitory checkpoint molecules include A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 and VISTA. The Adenosine A2A receptor (A2AR) is regarded as an important checkpoint in cancer therapy because adenosine in the immune microenvironment, leading to the activation of the A2a receptor, is negative immune feedback loop and the tumor microenvironment has relatively high concentrations of adenosine. B7-H3, also called CD276, was originally understood to be a co-stimulatory molecule but is now regarded as co-inhibitory.
B7-H4, also called VTCN1, is expressed by tumor cells and tumor-associated macrophages and plays a role in tumour escape. B and T Lymphocyte Attenuator (BTLA) and also called CD272, has HVEM (Herpesvirus Entry Mediator) as its ligand. Surface expression of BTLA is gradually downregulated during differentiation of human CD8+ T cells from the naive to effector cell phenotype, however tumor-specific human CD8+ T cells express high levels of BTLA. CTLA-4, Cytotoxic T -Lymphocyte- Associated protein 4 and also called CD152. Expression of CTLA-4 on Treg cells serves to control T cell proliferation. IDO, Indoleamine 2, 3 -di oxygenase, is a tryptophan catabolic enzyme. A related immune-inhibitory enzymes. Another important molecule is TDO, tryptophan 2,3 -di oxygenase. IDO is known to suppress T and NK cells, generate and activate Tregs and myeloid-derived suppressor cells, and promote tumour angiogenesis. KIR, Killer-cell Immunoglobulin-like Receptor, is a receptor for MHC Class I molecules on Natural Killer cells. LAG3, Lymphocyte Activation Gene-3, works to suppress an immune response by action to Tregs as well as direct effects on CD8+ T cells. PD- 1, Programmed Death 1 (PD-1) receptor, has two ligands, PD-L1 and PD-L2. This checkpoint is the target of Merck & Co.'s melanoma drug Keytruda, which gained FDA approval in September 2014. An advantage of targeting PD-1 is that it can restore immune function in the tumor microenvironment. TIM-3, short for T-cell Immunoglobulin domain and Mucin domain 3, expresses on activated human CD4+ T cells and regulates Thl and Thl7 cytokines. TIM-3 acts as a negative regulator of Thl/Tcl function by triggering cell death upon interaction with its ligand, galectin-9. VISTA, Short for V-domain Ig suppressor of T cell activation, VISTA is primarily expressed on hematopoietic cells so that consistent expression of VISTA on leukocytes within tumors may allow VISTA blockade to be effective across a broad range of solid tumors. Tumor cells often take advantage of these checkpoints to escape detection by the immune system. Thus, inhibiting a checkpoint protein on the immune system may enhance the anti-tumor T-cell response.
In some embodiments, an immune checkpoint inhibitor refers to any compound inhibiting the function of an immune checkpoint protein. Inhibition includes reduction of function and full blockade. In some embodiments, the immune checkpoint inhibitor could be an antibody, synthetic or native sequence peptides, small molecules or aptamers which bind to the immune checkpoint proteins and their ligands.
In a particular embodiment, the immune checkpoint inhibitor is an antibody.
Typically, antibodies are directed against A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 or VISTA.
In a particular embodiment, the immune checkpoint inhibitor is an anti -PD- 1 antibody such as described in WO2011082400, W02006121168, W02015035606, W02004056875, W02010036959, W02009114335, W02010089411, WO2008156712, WO2011110621, WO2014055648 and WO2014194302. Examples of anti-PD-1 antibodies which are commercialized: Nivolumab (Opdivo®, BMS), Pembrolizumab (also called Lambrolizumab, KEYTRUDA® or MK-3475, MERCK).
In some embodiments, the immune checkpoint inhibitor is an anti-PD-Ll antibody such as described in WO2013079174, W02010077634, W02004004771, WO2014195852, W02010036959, WO2011066389, W02007005874, W02015048520, US8617546 and WO2014055897. Examples of anti-PD-Ll antibodies which are on clinical trial: Atezolizumab (MPDL3280A, Genentech/Roche), Durvalumab (AZD9291, AstraZeneca), Avelumab (also known as MSB0010718C, Merck) and BMS-936559 (BMS).
In some embodiments, the immune checkpoint inhibitor is an anti-PD-L2 antibody such as described in US7709214, US7432059 and US8552154.
In the context of the invention, the immune checkpoint inhibitor inhibits Tim-3 or its ligand.
In a particular embodiment, the immune checkpoint inhibitor is an anti-Tim-3 antibody such as described in WO03063792, WO2011155607, WO2015117002, WO2010117057 and W02013006490.
In some embodiments, the immune checkpoint inhibitor is a small organic molecule.
The term "small organic molecule" as used herein, refers to a molecule of a size comparable to those organic molecules generally used in pharmaceuticals. The term excludes biological macro molecules (e. g. proteins, nucleic acids, etc.). Typically, small organic molecules range in size up to about 5000 Da, more preferably up to 2000 Da, and most preferably up to about 1000 Da.
Typically, the small organic molecules interfere with transduction pathway of A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 or VISTA.
In a particular embodiment, small organic molecules interfere with transduction pathway of PD-1 and Tim-3. For example, they can interfere with molecules, receptors or enzymes involved in PD-1 and Tim-3 pathway.
In a particular embodiment, the small organic molecules interfere with Indoleamine- pyrrole 2,3-dioxygenase (IDO) inhibitor. IDO is involved in the tryptophan catabolism (Liu et al 2010, Vacchelli et al 2014, Zhai et al 2015). Examples of IDO inhibitors are described in
WO 2014150677. Examples of IDO inhibitors include without limitation 1 -methyl-tryptophan (IMT), b- (3-benzofuranyl)-alanine, P-(3-benzo(b)thienyl)-alanine), 6-nitro-tryptophan, 6- fluoro-tryptophan, 4-methyl-tryptophan, 5 -methyl tryptophan, 6-methyl-tryptophan, 5- methoxy -tryptophan, 5 -hydroxy -tryptophan, indole 3-carbinol, 3,3'- diindolylmethane, epigallocatechin gallate, 5-Br-4-Cl-indoxyl 1,3-diacetate, 9- vinylcarbazole, acemetacin, 5- bromo-tryptophan, 5-bromoindoxyl diacetate, 3- Amino-naphtoic acid, pyrrolidine dithiocarbamate, 4-phenylimidazole a brassinin derivative, a thiohydantoin derivative, a b- carboline derivative or a brassilexin derivative. In a particular embodiment, the IDO inhibitor is selected from 1 -methyl -tryptophan, b-(3- benzofuranyl)-alanine, 6-nitro-L-tryptophan, 3- Amino-naphtoic acid and b-[3- benzo(b)thienyl] -alanine or a derivative or prodrug thereof.
In a particular embodiment, the inhibitor of IDO is Epacadostat, (INCB24360, INCB024360) has the following chemical formula in the art and refers to -N-(3-bromo-4- fluorophenyl)-N'-hydroxy-4-{[2-(sulfamoylamino)-ethyl]amino}-l,2,5-oxadiazole-3 carboximidamide :
In a particular embodiment, the inhibitor is BGB324, also called R428, such as described in W02009054864, refers to lH-1, 2, 4-Triazole-3, 5-diamine, l-(6,7-dihydro-5H- benzo[6,7]cyclohepta[l,2-c]pyridazin-3-yl)-N3-[(7S)-6,7,8,9-tetrahydro-7-(l-pyrrolidinyl)- 5H-benzocyclohepten-2-yl]- and has the following formula in the art:
In a particular embodiment, the inhibitor is CA-170 (or AUPM-170): an oral, small molecule immune checkpoint antagonist targeting programmed death ligand-1 (PD-L1) and V- domain Ig suppressor of T cell activation (VISTA) (Liu et al 2015). Preclinical data of CA-170 are presented by Curis Collaborator and Aurigene on November at ACR-NCI-EORTC International Conference on Molecular Targets and Cancer Therapeutics.
In some embodiments, the immune checkpoint inhibitor is an aptamer.
Typically, the aptamers are directed against A2AR, B7-H3, B7-H4, BTLA, CTLA-4, CD277, IDO, KIR, PD-1, LAG-3, TIM-3 or VISTA.
In a particular embodiment, aptamers are DNA aptamers such as described in Prodeus et al 2015. A major disadvantage of aptamers as therapeutic entities is their poor pharmacokinetic profiles, as these short DNA strands are rapidly removed from circulation due to renal filtration. Thus, aptamers according to the invention are conjugated to with high molecular weight polymers such as polyethylene glycol (PEG). In a particular embodiment, the aptamer is an anti -PD-1 aptamer. Particularly, the anti -PD-1 aptamer is MP7 pegylated as described in Prodeus et al 2015.
In certain embodiments, the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator is used in combination with a third agent for treatment of a disease or disorder. When used for treating cancer, the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator may be used in combination with conventional cancer therapies such as, e.g., surgery, radiotherapy, chemotherapy, or combinations thereof.
The present invention also provides for therapeutic applications where the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator are used in combination with at least one further therapeutic agent, e.g. for treating cancers and metastatic cancers. Such administration may be simultaneous, separate or sequential. For simultaneous administration the agents may be administered as one composition or as separate compositions, as appropriate. The further therapeutic agent is typically relevant for the disorder to be treated. Exemplary therapeutic agents include other anti-cancer antibodies, cytotoxic agents, chemotherapeutic agents, radiotherapeutics agents, anti-angiogenic agents, anti-cancer immunogens, cell cycle control/apoptosis regulating agents, hormonal regulating agents, and other agents described below.
In the context of the invention, inventors combined gemcitabine treatment (the reference treatment for PD AC) to iron deprivation using H7 and iron chelator combination. Indeed, in preliminary experiments they observe a synergistic effect of DFX and gemcitabine in BxPC3 3D cultures which is additionally increased by H7 treatment. By using an anti-TfRl antibody, they could also benefit in vivo from the ADCC capabilities of H7 in addition to the intrinsic effects accomplished by iron deprivation.
Accordingly, in a third aspect, the invention relates to an i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) a chemotherapeutic agent for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
As used herein, the term "chemotherapeutic agent" refers to chemical compounds that are effective in inhibiting tumor growth. Examples of chemotherapeutic agents include alkylating agents such as thiotepa and cyclosphosphamide; alkyl sulfonates such as busulfan, improsulfan and piposulfan; aziridines such as benzodopa, carboquone, meturedopa, and uredopa; ethylenimines and methylamelamines including altretamine, triethylenemelamine,
trietylenephosphoramide, triethylenethiophosphaorarnide and trimethylolomelamine; acetogenins (especially bullatacin and bullatacinone); a carnptothecin (including the synthetic analogue topotecan); bryostatin; callystatin; CC-1065 (including its adozelesin, carzelesin and bizelesin synthetic analogues); cryptophycins (particularly cryptophycin 1 and cryptophycin 8); dolastatin; duocarmycin (including the synthetic analogues, KW-2189 and CBI-TMI); eleutherobin; pancrati statin; a sarcodictyin; spongistatin; nitrogen mustards such as chlorambucil, chlornaphazine, cholophosphamide, estrarnustine, ifosfamide, mechlorethamine, mechlorethamine oxide hydrochloride, melphalan, novembichin, phenesterine, prednimus tine, trofosfamide, uracil mustard; nitrosureas such as carmustine, chlorozotocin, fotemustine, lomustine, nimustine, ranimustine; antibiotics such as the enediyne antibiotics (e.g. calicheamicin, especially calicheamicin (11 and calicheamicin 211, see, e.g., Agnew Chem Inti. Ed. Engl. 33 : 183-186 (1994); dynemicin, including dynemicin A; an esperamicin; as well as neocarzinostatin chromophore and related chromoprotein enediyne antiobiotic chromomophores), aclacinomysins, actinomycin, authramycin, azaserine, bleomycins, cactinomycin, carabicin, canninomycin, carzinophilin, chromomycins, dactinomycin, daunorubicin, detorubicin, 6-diazo-5-oxo-L-norleucine, doxorubicin (including morpholino- doxorubicin, cyanomorpholino-doxorubicin, 2-pyrrolino-doxorubicin and deoxydoxorubicin), epirubicin, esorubicin, idanrbicin, marcellomycin, mitomycins, mycophenolic acid, nogalarnycin, olivomycins, peplomycin, potfiromycin, puromycin, quelamycin, rodorubicin, streptomgrin, streptozocin, tubercidin, ubenimex, zinostatin, zorubicin; anti-metabolites such as methotrexate and 5-fluorouracil (5-FU); folic acid analogues such as denopterin, methotrexate, pteropterin, trimetrexate; purine analogs such as fludarabine, 6-mercaptopurine, thiamiprine, thioguanine; pyrimidine analogs such as ancitabine, azacitidine, 6-azauridine, carmofur, cytarabine, dideoxyuridine, doxifluridine, enocitabine, floxuridine, 5-FU; androgens such as calusterone, dromostanolone propionate, epitiostanol, mepitiostane, testolactone; anti adrenals such as aminoglutethimide, mitotane, trilostane; folic acid replenisher such as frolinic acid; aceglatone; aldophospharnide glycoside; aminolevulinic acid; amsacrine; bestrabucil; bisantrene; edatraxate; defo famine; demecolcine; diaziquone; elfornithine; elliptinium acetate; an epothilone; etoglucid; gallium nitrate; hydroxyurea; lentinan; lonidamine; maytansinoids such as maytansine and ansamitocins; mitoguazone; mitoxantrone; mopidamol; nitracrine; pento statin; phenamet; pirarubicin; podophyllinic acid; 2-ethylhydrazide; procarbazine; PSK®; razoxane; rhizoxin; sizofiran; spirogennanium; tenuazonic acid; triaziquone; 2, 2', 2"- trichlorotriethylamine; trichothecenes (especially T-2 toxin, verracurin A, roridinA and
anguidine); urethan; vindesine; dacarbazine; mannomustine; mitobromtol; mitolactol; pipobroman; gacytosine; arabinoside ("Ara-C"); cyclophosphamide; thiotepa; taxoids, e.g. paclitaxel (TAXOL®, Bristol-Myers Squibb Oncology, Princeton, N.].) and doxetaxel (TAXOTERE®, Rhone-Poulenc Rorer, Antony, France); chlorambucil; gemcitabine; 6- thioguanine; mercaptopurine; methotrexate; platinum analogs such as cisp latin and carhop latin; vinblastine; platinum; etoposide (VP- 16); ifosfamide; mitomycin C; mitoxantrone; vincristine; vinorelbine; navelbine; novantrone; teniposide; daunomycin; aminopterin; xeloda; ibandronate; CPT-1 1 ; topoisomerase inhibitor RFS 2000; difluoromethylornithine (DMFO); retinoic acid; capecitabine; and pharmaceutically acceptable salts, acids or derivatives of any of the above. Also included in this definition are antihormonal agents that act to regulate or inhibit honnone action on tumors such as anti-estrogens including for example tamoxifen, raloxifene, aromatase inhibiting 4(5)-imidazoles, 4-hydroxytamoxifen, trioxifene, keoxifene, LY117018, onapristone, and toremifene (Fareston); and anti-androgens such as flutamide, nilutamide, bicalutamide, leuprolide, and goserelin; and pharmaceutically acceptable salts, acids or derivatives of any of the above.
In a particular embodiment, the i) antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator are used in combination with gemcitabine.
In a particular embodiment, the i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator are used in combination with Monomethyl Auristatin F (MMAF) which is a synthetic antineoplastic agent and an inhibitor of microtubule polymerization using a non-cleavable linker.
In a fourth aspect, the invention relates to an i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) an immune check point inhibitor for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
As used herein the terms "administering" or "administration" refer to the act of injecting or otherwise physically delivering a substance as it exists outside the body (e.g., an antibody anti-TfRl and an iron chelator) into the subject, such as by mucosal, intradermal, intravenous, subcutaneous, intramuscular delivery and/or any other method of physical delivery described herein or known in the art. When a disease, or a symptom thereof, is being treated, administration of the substance typically occurs after the onset of the disease or symptoms
thereof. When a disease or symptoms thereof, are being prevented, administration of the substance typically occurs before the onset of the disease or symptoms thereof.
By a "therapeutically effective amount" is meant a sufficient amount of an antibody anti- TfRl for use in a method for the treatment of melanoma at a reasonable benefit/risk ratio applicable to any medical treatment. It will be understood that the total daily usage of the compounds and compositions of the present invention will be decided by the attending physician within the scope of sound medical judgment. The specific therapeutically effective dose level for any particular subject will depend upon a variety of factors including the age, body weight, general health, sex and diet of the subject; the time of administration, route of administration, and rate of excretion of the specific compound employed; the duration of the treatment; drugs used in combination or coincidental with the specific polypeptide employed; and like factors well known in the medical arts. For example, it is well known within the skill of the art to start doses of the compound at levels lower than those required to achieve the desired therapeutic effect and to gradually increase the dosage until the desired effect is achieved. However, the daily dosage of the products may be varied over a wide range from 0.01 to 1,000 mg per adult per day. Typically, the compositions contain 0.01, 0.05, 0.1, 0.5, 1.0, 2.5, 5.0, 10.0, 15.0, 25.0, 50.0, 100, 250 and 500 mg of the active ingredient for the symptomatic adjustment of the dosage to the subject to be treated. A medicament typically contains from about 0.01 mg to about 500 mg of the active ingredient, typically from 1 mg to about 100 mg of the active ingredient. An effective amount of the drug is ordinarily supplied at a dosage level from 0.0002 mg/kg to about 20 mg/kg of body weight per day, especially from about 0.001 mg/kg to 7 mg/kg of body weight per day.
In a fifth aspect, the invention relates to an i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) an immune check point inhibitor, for use in the treatment of resistant cancer, as a combined preparation.
As used herein, the terms“combined treatment”,“combined therapy” or“therapy combination” refer to a treatment that uses more than one medication. The combined therapy may be dual therapy or bi-therapy.
Typically, the i) antibody-anti TfRl and ii) the iron chelator as a combined preparation according to the invention for simultaneous, separate or sequential use in the method for treating. As used herein, the term“simultaneous use” refers to an administration of 2 active
ingredients by the same route and at the same time or at substantially the same time. The term “separate use” refers to an administration of 2 active ingredients at the same time or at substantially the same time by different routes. The term “sequential use” refers to an administration of 2 active ingredients at different times, the administration route being identical or different.
The i) anti-TfRl antibody and ii) the iron chelator as described above may be combined with pharmaceutically acceptable excipients, and optionally sustained-release matrices, such as biodegradable polymers, to form pharmaceutical compositions. "Pharmaceutically" or "pharmaceutically acceptable" refer to molecular entities and compositions that do not produce an adverse, allergic or other untoward reaction when administered to a mammal, especially a human, as appropriate. A pharmaceutically acceptable carrier or excipient refers to a non-toxic solid, semi-solid or liquid filler, diluent, encapsulating material or formulation auxiliary of any type. The pharmaceutical compositions of the present invention for oral, sublingual, subcutaneous, intramuscular, intravenous, transdermal, local or rectal administration, the active principle, alone or in combination with another active principle, can be administered in a unit administration form, as a mixture with conventional pharmaceutical supports, to animals and human beings. Suitable unit administration forms comprise oral-route forms such as tablets, gel capsules, powders, granules and oral suspensions or solutions, sublingual and buccal administration forms, aerosols, implants, subcutaneous, transdermal, topical, intraperitoneal, intramuscular, intravenous, subdermal, transdermal, intrathecal and intranasal administration forms and rectal administration forms. Typically, the pharmaceutical compositions contain vehicles which are pharmaceutically acceptable for a formulation capable of being injected. These may be in particular isotonic, sterile, saline solutions (monosodium or disodium phosphate, sodium, potassium, calcium or magnesium chloride and the like or mixtures of such salts), or dry, especially freeze-dried compositions which upon addition, depending on the case, of sterilized water or physiological saline, permit the constitution of injectable solutions. The pharmaceutical forms suitable for injectable use include sterile aqueous solutions or dispersions; formulations including sesame oil, peanut oil or aqueous propylene glycol; and sterile powders for the extemporaneous preparation of sterile injectable solutions or dispersions. In all cases, the form must be sterile and must be fluid to the extent that easy syringability exists. It must be stable under the conditions of manufacture and storage and must be preserved against the contaminating action of microorganisms, such as bacteria and fungi. Solutions comprising
compounds of the invention as free base or pharmacologically acceptable salts can be prepared in water suitably mixed with a surfactant, such as hydroxypropylcellulose. Dispersions can also be prepared in glycerol, liquid polyethylene glycols, and mixtures thereof and in oils. Under ordinary conditions of storage and use, these preparations contain a preservative to prevent the growth of microorganisms. The polypeptide (or nucleic acid encoding thereof) can be formulated into a composition in a neutral or salt form. Pharmaceutically acceptable salts include the acid addition salts (formed with the free amino groups of the protein) and which are formed with inorganic acids such as, for example, hydrochloric or phosphoric acids, or such organic acids as acetic, oxalic, tartaric, mandelic, and the like. Salts formed with the free carboxyl groups can also be derived from inorganic bases such as, for example, sodium, potassium, ammonium, calcium, or ferric hydroxides, and such organic bases as isopropylamine, trimethylamine, histidine, procaine and the like. The carrier can also be a solvent or dispersion medium containing, for example, water, ethanol, polyol (for example, glycerol, propylene glycol, and liquid polyethylene glycol, and the like), suitable mixtures thereof, and vegetables oils. The proper fluidity can be maintained, for example, by the use of a coating, such as lecithin, by the maintenance of the required particle size in the case of dispersion and by the use of surfactants. The prevention of the action of microorganisms can be brought about by various antibacterial and antifungal agents, for example, parabens, chlorobutanol, phenol, sorbic acid, thimerosal, and the like. In many cases, it will be preferable to include isotonic agents, for example, sugars or sodium chloride. Prolonged absorption of the injectable compositions can be brought about by the use in the compositions of agents delaying absorption, for example, aluminium monostearate and gelatin. Sterile injectable solutions are prepared by incorporating the active polypeptides in the required amount in the appropriate solvent with several of the other ingredients enumerated above, as required, followed by filtered sterilization. Generally, dispersions are prepared by incorporating the various sterilized active ingredients into a sterile vehicle which contains the basic dispersion medium and the required other ingredients from those enumerated above. In the case of sterile powders for the preparation of sterile injectable solutions, the preferred methods of preparation are vacuum drying and freeze-drying techniques which yield a powder of the active ingredient plus any additional desired ingredient from a previously sterile-filtered solution thereof. Upon formulation, solutions will be administered in a manner compatible with the dosage formulation and in such amount as is therapeutically effective. The formulations are easily administered in a variety of dosage forms, such as the type of injectable solutions described above, but drug
release capsules and the like can also be employed. For parenteral administration in an aqueous solution, for example, the solution should be suitably buffered if necessary and the liquid diluent first rendered isotonic with sufficient saline or glucose. These particular aqueous solutions are especially suitable for intravenous, intramuscular, subcutaneous and intraperitoneal administration. In this connection, sterile aqueous media which can be employed will be known to those of skill in the art in light of the present disclosure. For example, one dosage could be dissolved in 1 ml of isotonic NaCl solution and either added to 1000 ml of hypodermoclysis fluid or inj ected at the proposed site of infusion. Some variation in dosage will necessarily occur depending on the condition of the subject being treated. The person responsible for administration will, in any event, determine the appropriate dose for the individual subject.
In a sixth aspect, the invention relates to a pharmaceutical composition comprising the combined preparation according to the invention.
In a particular embodiment, the pharmaceutical composition according to the invention for use in the treatment of cancer.
In a particular embodiment, the pharmaceutical composition according to the invention for use in the treatment of resistant cancer.
The invention will be further illustrated by the following figures and examples. However, these examples and figures should not be interpreted in any way as limiting the scope of the present invention.
FIGURES:
Figure 1: The effect of the combination of H7 with DFO or DFX on the cell viabilities of PDAC cells. BxPC3 and CFPAC cells were plated, 24hrs later they were treated with either DFO (3mM) or DFX (4 mM) alone or with increasing concentrations of H7 alone ranging from (0.3 pg/ml to 2pg/ml) or with the combination (H7 and DFO at 3 mM) or (H7 and DFX 4 pM). After 5 days cell viability was assessed using the MTS assay (cellTiter 96, Promega). B. HP AC cells in DMEM medium were plated and treated the next day with either DFO alone at 0.5 or 1 pM or increasing concentrations of H7 as indicated in A or combinations with different H7 concentrations and DFO at 0.5 or 1 pM 5 days after treatment cell viability is assessed by MTS.
Figure 2: H7, DFO, and DFX dose response curves on BxPC3 and CFPAC cells (A,B,C). PDAC cells were plated, 24hrs later H7, DFO, or DFX were added with increasing concentrations. After 5 days cell viability was assessed using MTS assay (cellTiter 96, Promega). Effect of the combination of H7 and DFO or DFX on cell viability (D,E). BxPC3 and CFPAC cells were plated, 24hrs later they were treated with either DFO (3mM) or DFX (4 mM) alone or with increasing concentrations of H7 alone ranging from (0.3 pg/ml to 2pg/ml) or with the combination (H7 and DFO at 3 mM) or (H7 and DFX 4 mM). After 5 days cell viability was assessed using the MTS assay (cellTiter 96, Promega).
Figure 3: Effect of the combination of H7 with DFO (A) or DFX (B) on the cell cycle phase repartition of BxPC3 and CFPAC cells. After 24 hours of plating, cells were treated for 3 days with either H7 (2 pg/ml), DFO (3 mM), DFX (2 mM), the combination of H7 at 2 pg/ml with DFO 3 mM or the combination of H7 (2 pg/ml) and DFX (2 mM). Cells were then stained with PI before FACS analysis. Combination of H7 and iron chelator treatment synergizes to block cell cycle progression in D phase.
Figure 4: Effect of the combination of H7 with DFO (A) or DFX (B) on apoptosis of BxPC3 and CFPAC cells. After 24 hours of plating, cells were treated for 5 days with either H7 (2 pg/ml), with DFO (3 pM), DFX (2 pM), combination of H7 (2 pg/ml) with DFO 3 pM, or combination of H7 (2 pg/ml) and DFX (2 pM). Cells were then stained with AnnexinV- FITC and 7AAD before FACS analysis. Early (Annexin positive) and late apoptosis (Annexin positive 7AAD positive) are presented. The association of H7 treatment with an iron chelator increases apoptosis induction in both cell lines compared to single treatment.
Figure 5: Effect of iron chelators on holo-Tf-Alexa 488 uptake of the CFPAC cell line. Non confluent CFPAC cells were incubated with 500 nM holoTf conjugated to Alexa 488 and either left untreated or treated with DFO or DFX (100 pM), non fluorescent holoTf (10 mM), or H7 at 45 nM for 4 hrs at 37°C. Internalized fluorescence was measured by FACS and the results are shown as the % holoTf uptake relative to NT. Here, an excess of holo-Tf blocks as expected fluorescent holo-Tf uptake, like the competitor H7. Iron chelators do not reduce fluorescent holo-Tf uptake consistent with their inability to chelate iron from holo-Tf. If it was the case, holo-Tf would be converted in iron free Tf (apo-Tf) that has low affinity for TfRl, therefore, fluorescence intensity of the cells would be reduced.
Figure 6: Viability of CFPAC cell treated with H7, DFO, or DFX combined or not with Ferric ammonium citrate. Cells were either non treated (NT) or treated as indicated for 5 days and cell viability is then measured by MTS (cell Titer, 96). (Up) FAC in excess (free
iron) reverses the viability decrease observed with iron chelators as expected, but also viability decrease observed with H7 likely by an increase of uptake of free iron. (Down) holo-Tf in excess reverses as expected the viability decrease obtained with H7, but also with the decrease of viability observed with iron chelators, likely by an increase of holo-Tf uptake. This shows that the two mechanism of iron uptake are independent.
Figure 7: In vivo effect of H7 and DFX combination on BxPC3 PDAC growth in nude mice. BxPC3 cells s.c. were grafted in nude mice. Established tumors were either treated with NaCl, H7 at 5 mg/kg twice a week, i.p., DFX 40 mg/kg by gavage, 3 times a week or combination of the 2 treatments for 4 weeks (from day 20 to day 48). Mice were sacrificed when their tumor reached 1500 mm3. Tumor size was plotted in function of the time (day) after graft.
EXAMPLES:
1) Combination treatment of H7 with either DFO or DFX showed a better decrease in cell viability of PDAC cell lines compared to single treatment
First we tested the effects of the combinations on cell viability. For the DFO combinations, BxPC3 and CFPAC cells were treated with either DFO alone at approximately half maximal inhibitory concentration 3 mM (data not shown) or with increasing H7 concentrations starting from 0.3 pg/ml and reaching 2 pg/ml (data not shown) or with the combinations of a fixed dose of DFO (3mM) and the different concentrations of H7. The dose response curve of DFX demonstrates the inhibitory effects of DFX alone on the viability of both BxPC3 (data not shown) and CFPAC (data not shown) cell lines. The combinations of H7 and DFX are done with a fixed DFX concentration of 4 mM and a varying concentration of H7 just like the DFO combinations.
The results show that adding H7 to DFO or DFX resulted in an increased suppression of cell viability in a dose dependent manner (Figure 1). For example, on the BxPC3 cell line DFO alone at 4 mM showed a cell viability of 47% (Figure 51 A), with H7 alone the viability was 92% at 0.03 pg/ml, 77 % at 0.5 pg/ml, and 57% at 2 pg/ml. When H7 was combined to DFO 4 mM, the viability was reduced to 37 %, 20%, and 15%, respectively. If we take another example but on the CFPAC cell line, DFO alone at 3 mM showed a viability of 66 % while H7 alone at 2 pg/ml showed a 60% viability and the viability was 22% for the combination. The enhanced effects on cell viability were also observed with DFX (Figure 1 A). For instance, on the BxPC3 cell line the viability decreased from 48 % with DFX at 4 mM and 57 % with H7 at
2 pg/ml, to 15 % with the combination at these concentrations. On the CFPAC cell line, the viability for DFX 4 mM was 29% and with H7 at 2 pg/ml was 38% and decreased to 7% with the combination indicating an almost complete inhibition of viability.
The HP AC cell line is resistant to H7 treatment in DMEM medium due to the presence of iron in this medium (0.25 mM ferric nitrate) which can reverse the effect of the antibody as mentioned earlier in the complementary results. In order to determine if we can sensitize the HP AC cell line to H7 by adding DFO we tried different combinations of H7 and DFO on cell viability. Figure IB shows that adding a very low concentration of DFO 0.5 mM or 1 mM (at which DFO shows no effect by itself) to H7, the HP AC cell line becomes sensitive to H7 treatment showing a decrease in cell viability by 40%. Because at these concentrations both H7 and DFO are not effective, it seems there is a synergistic effect for this combination, probably DFO binding iron in the medium and thus allowing H7 to decrease cell viability by blocking holoTf uptake.
2) G1 and S phase arrests are observed with the combination of the anti-TfRl antibody and DFO or DFX
It been shown that iron deprivation results in a block in the G1 or S phase of the cell cycle depending on the cell line and the chelator used (Siriwardana and Seligman, 2013). We wanted to determine if the combination of the iron chelators with H7 affects the distribution of cells in the different phases of the cell cycle. After 3 days of treatment, H7 alone at 10 pg/ml arrested cells in the S phase and so did DFO at a dose of 10 mM (data not shown). We used concentrations of H7 (2 pg/ml) and DFO (3 mM) or DFX (2 mM or 4 mM). Cetuximab (10 pg/ml) served as a negative control showing no effect on the cell cycle in vitro (data not shown).
On the BxPC3 cell line, H7 (2 pg/ml) combination with DFO (3 pM) induced a strong increase in the percentage of cells in the S phase (data not shown). This was also accompanied with an increase in subGl phase (apoptotic cells) indicating that after 3 days some of the cells are dying. On the CFPAC cell line, the same combination (same concentrations) lead to an S phase arrest more probably at the early S phase or the Gl/S boundary and an increase in cells in SubGl phase as well (data not shown).
Different concentrations of DFX induced different blocks in the cell cycle as seen with dose response of DFX on BxPC3 (data not shown) and CFPAC (data not shown). On BxPC3, DFX at 2 pM did not alter the cell cycle while at 4 pM an S phase block was observed. At 10 pM cells were blocked in the Gl/S interphase. A possible explanation would be that at lower DFX concentration cells were blocked in S phase while at higher DFX concentration better iron
deprivation was obtained and so cells could not even pass from the G1 phase to the S phase because of the complete inhibition of the ribonucleotide reductase enzyme activity.
When H7 and DFX at 2 mM are combined on the BxPC3 cell line, cells were arrested in S phase (data not shown). However, when H7 is combined with 4 pM of DFX there is a block in Gl/S boundary, an effect which is similar to that of DFX alone at 10 pM, indicating that with these combination more iron deprivation occurred. The same results were obtained with the CFPAC cell line where the combination of H7 with DFX 2 pM showed a stop in S phase while the combination of H7 with DFX 4 pM resulted in an arrest at the Gl/S boundary just like DFX 10 pM alone did (data not shown). These results indicates that the combinations of H7 with DFO or DFX induces more iron deprivation and hence a better blockade of the cell cycle (Gl/S or S phase).
3) PDAC cells are more sensitive to apoptosis induction when H7 is combined with DFO or DFX
As already shown above with the cell cycle results, after 3 days of the combination treatment there is an increase in the percentage of subGl cells compared to each treatment alone. In order to demonstrate better the effect of the combination on cell apoptosis, we stained the cells with Annexin V and 7AAD and analyzed the results by flow cytometry after 5 days of treatment. In this experiment Cetuximab at 10 pg/ml was used as a negative control, with no increase in apoptosis being observed with this treatment (data not shown). On the BxPC3 cell line the combination of H7 at 2 pg/ml and DFO 3 pM increased the percentage of apoptosis (combined early and late apoptosis) from 33% with H7 alone and 39% with DFX to 70% with the combination. These results indicate that there is an additive effect with the combination on this cell line. On the CFPAC cell line, H7 alone and DFO alone at the same concentrations mentioned above induced apoptosis of 19% and 22%, respectively and 64% with the combination, indicating a possible synergistic effect (data not shown). Combinations of H7 with different concentrations of DFX (1, 2, or 4 pM) show as well increased apoptosis on both cell lines (data not shown). Therefore, combining the anti-TfRl antibody with both iron chelators improves the effects on apoptosis compared to single treatment.
4) Upregulation of the expression of the metastasis suppressor NDRG1 with the combination of H7 and DFO
We have already shown that H7 as well as DFO induce NDRG1 expression on the BxPC3 and CFPAC cell lines (data not shown). We wanted to determine if the combination of H7 and DFO had an additive or a synergistic effect on the induction of NDRG1. Because
NDRG1 expression is strongly induced by the single treatment of both H7 and DFO, we used a very low concentrations of both, since the effect of one would dominate over the other and it would be difficult to determine an effect with the combination. We used DFO at 10 mM as a positive control for the induction of NDRG1 (data not shown). On the BxPC3 cell line, a modest effect was observed on NDRG1 induction with H7 at 0.5 pg/ml and there was almost no effect for DFO whether at 0.5 mM or 1 mM. When H7 at 0.5 mg/ml was combined with DFO at either 0.5 mM or 1 mM, a better induction of NDRG1 was observed (data not shown). On the CFPAC cell line, this increase in NDRG1 was also observed combining H7 at 0.5 pg/ml and DFO at 1 mM (data not shown). The most striking result was observed on the HP AC cell line cultured in DMEM which is resistant to H7 treatment, (data not shown). Neither H7 at 10 pg/ml had effect on NDRGl expression nor DFO at 0.5 mM or 1 mM. In contrast, the positive control DFO showed a strong NDRGl induction at 10 mM. Interestingly, the combination of H7 at 10 pg/ml with either concentrations of DFO (0.5 or 1 mM) induced NDRGl expression indicating that the combination of H7 with a low dose of DFO is sufficient to induce NDRGl on this cell line. Thus combinations of DFO and H7 also augments the induction of NDRGl in all the cell lines tested.
5) Anti-TfRl mAb H7 and chelators mechanism of action
We next asked if the mechanism of inhibition of both inhibitors (the iron chelators or the TfRl blocking antibody H7) were acting on distinct or similar iron sources (chelators on the LIP and iron stored in ferritin) and H7 (iron from internalized holoTf).
First we checked if iron chelators could directly chelate iron from holoTf (i.e. iron saturated Tf) in the extracellular medium. We used the same protocol used in the article (data not shown). Briefly, CFPAC cells were incubated for 4 hrs. at 37°C with holoTf-Alexa 488 (500 nM) combined or not with an excess of iron chelators (100 pM) (data not shown). In this experimental setup, because apoTf (unsaturated Tf) cannot be internalized through TfRl mediated endocytosis due to poor affinity for TfRl at extracellular pH (Young et ak, 1984), cells can only accumulate fluorescence by internalization of holo-Tf and not apo-Tf. Iron chelators had no effect on fluorescence accumulation in cells indicating that iron chelators do not readily chelate iron directly form holoTf consistent with other studies (Devanur et ak, 2008).
As expected, an excess of non fluorescent holoTf abrogated fluorescence accumulation in cells by a competition mechanism, and as previously shown, H7 45 nM i.e at more than 10 times lower concentration than holoTf, blocked holoTf uptake by 40% (data not shown). We then tested if the decreased viability observed with each iron deprivating agent could be
reversed by an excess of either holoTf or soluble iron (ferric ammonium citrate, FAC). CFPAC cells were incubated with of H7 and/or iron chelators in the presence or not of FAC (data not shown) or holoTf (data not shown) for 5 days and viability was determined.
Holo-Tf and ferric citrate reversed the inhibitory effect of both H7 and iron chelators, indicating that their mechanism of action likely converges towards LIP and intracellular iron storage reduction. The increased toxic effects observed on PD AC cell lines by combining the 2 inhibitors are likely be due to reaching an intracellular LIP concentration below a threshold level necessary for cancer cell normal metabolism.
6) An additive effect on cell viability decrease is obtained with the combination treatment.
PDAC cells were plated, 24hrs later H7, DFO, or DFX were added with increasing concentrations. After 5 days cell viability was assessed using MTS assay (cellTiter 96, Promega). Effect of the combination of H7 and DFO or DFX on cell viability (D,E). BxPC3 and CFPAC cells were plated, 24hrs later they were treated with either DFO (3mM) or DFX (4 mM) alone or with increasing concentrations of H7 alone ranging from (0.3 pg/ml to 2pg/ml) or with the combination (H7 and DFO at 3 mM) or (H7 and DFX 4 mM). After 5 days cell viability was assessed using the MTS assay (cellTiter 96, Promega). An additive effect on cell viability decrease is obtained with the combination treatment (Figure 2D-E).
7) Effect of the combination of H7 with DFO or DFX on the cell cycle phase repartition of BxPC3 and CFPAC cells.
After 24 hours of plating, cells were treated for 3 days with either H7 (2 pg/ml), DFO (3 mM), DFX (2 mM), the combination of H7 at 2 pg/ml with DFO 3 mM or the combination of H7 (2 pg/ml) and DFX (2 mM). Cells were then stained with PI before FACS analysis. Combination of H7 and iron chelator treatment synergizes to block cell cycle progression in D phase (Figure 3).
8) Effect of the combination of H7 with DFO (A) or DFX (B) on apoptosis of BxPC3 and CFPAC cells.
After 24 hours of plating, cells were treated for 5 days with either H7 (2 pg/ml), with DFO (3 pM), DFX (2 pM), combination of H7 (2 pg/ml) with DFO 3 pM, or combination of H7 (2 pg/ml) and DFX (2 pM). Cells were then stained with AnnexinV- FITC and 7AAD before FACS analysis. Early (Annexin positive) and late apoptosis (Annexin positive 7AAD positive) are presented. The association of H7 treatment with an iron chelator increases apoptosis induction in both cell lines compared to single treatment (Figure 4).
9) Effect of iron chelators on holo-Tf-Alexa 488 uptake of the CFPAC cell line.
Non confluent CFPAC cells were incubated with 500 nM holoTf conjugated to Alexa 488 and either left untreated or treated with DFO or DFX (100 mM), non fluorescent holoTf (10 mM), or H7 at 45 nM for 4 hrs at 37°C. Internalized fluorescence was measured by FACS and the results are shown as the % holoTf uptake relative to NT.
Here, an excess of holo-Tf blocks as expected fluorescent holo-Tf uptake, like the competitor H7. Iron chelators do not reduce fluorescent holo-Tf uptake consistent with their inability to chelate iron from holo-Tf. If it was the case, holo-Tf would be converted in iron free Tf (apo-Tf) that has low affinity for TfRl, therefore, fluorescence intensity of the cells would be reduced (Figure 5).
10) Viability of CFPAC cell treated with H7, DFO, or DFX combined or not with Ferric ammonium citrate. Cells were either non treated (NT) or treated as indicated for 5 days and cell viability is then measured by MTS (cell Titer, 96). (Figure 6 Left) FAC in excess (free iron) reverses the viability decrease observed with iron chelators as expected, but also viability decrease observed with H7 likely by an increase of uptake of free iron. (Figure 6 Right) holo Tf in excess reverses as expected the viability decrease obtained with H7, but also with the decrease of viability observed with iron chelators, likely by an increase of holo-Tf uptake. This shows that the two mechanism of iron uptake are independent (Figure 6).
11) In vivo effect of H7 and DFX combination on BxPC3 PD AC growth in nude mice. BxPC3 cells s.c. were grafted in nude mice. Established tumors were either treated with NaCl, H7 at 5 mg/kg twice a week, i.p., DFX 40 mg/kg by gavage, 3 times a week or combination of the 2 treatments for 4 weeks (from day 20 to day 48). Mice were sacrificed when their tumor reached 1500 mm3. Tumor size was plotted in function of the time (day) after graft.
The association of H7 and the iron chelator DFX reduced tumor growth compared to single treatment alone. In this experiment, DFX alone or H7 alone had no effect (Figure 7).
Conclusion:
The combinations of low concentrations of the iron chelators DFO or DFX, largely below concentrations observed in patients rated for iron overload (7.4 mM for DFO ad 80 mM for DFX) (Crichton et ak, 2016), with the anti-TfRl antibody effectively decreased cell viability compared to single treatments. They also showed more pronounced effects on the cell cycle arrest as well on apoptosis induction and NDRGl induction. Preliminary data that we obtained
recently on 3D cultures of BxPC3 cell line confirmed the increased effect of DFX and H7 combinations on cell viability compared to single treatment alone. Indeed, in 3D, while H7 alone had no visible inhibitory effect, it clearly potentialized DFX effect. DFX IC50 was 10 mM with no effects at 1 mM and when H7 (10 pg/mL was combined to DFX, inhibitory effects was detected starting for DFX concentration of 0.1 pM.
The advantages of this combination is that low concentrations of iron chelators can be used thus avoiding the potential toxic effects associated with iron chelators. Although by using H7 we are targeting the main route of iron supply however the presence of other iron uptake mechanisms is always a concern with using anti-TfRl antibody. Therefore, the combination of iron chelators which binds iron directly, in the extracellular fluids in vivo and intracellular iron (from iron in the LIP and ferritin turnover), with holoTf uptake blockade potentially leads to better iron deprivation and thus better effects.
REFERENCES:
Throughout this application, various references describe the state of the art to which this invention pertains. The disclosures of these references are hereby incorporated by reference into the present disclosure.
Claims
1. i) An antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation for simultaneous, separate or sequential use in the treatment of cancers.
2. The combined preparation for use according to claim 1, wherein said antibody is H7 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:2, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:3, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:4,
(d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:5; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:6, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:7.
3. The combined preparation for use according to claim 1, wherein said antibody is F12 antibody comprising: (a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:l 1, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO: 12, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO: 13, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO: 14;
(e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO: 15, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO: 16.
4. The combined preparation for use according to claim 1, wherein said antibody is C32 antibody comprising: a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:20, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:21, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:22, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:23; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:24, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:25.
5. The combined preparation for use according to claim 1, wherein said antibody is F2 antibody comprising: a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:29, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:30, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:31, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:32;
(e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:33, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:34.
6. The combined preparation for use according to claim 1, wherein said antibody is H9 antibody comprising: a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:38, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:39, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:40, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:41; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:42, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:43.
7. The combined preparation for use according to claim 1, wherein said antibody is G9 antibody comprising: a) a heavy chain CDR1 comprising the amino acid sequence of SEQ ID NO:47, (b) a heavy chain CDR2 comprising the amino acid sequence of SEQ ID NO:48, (c) a heavy chain CDR3 comprising the amino acid sequence of SEQ ID NO:49, (d) a light chain CDR1 comprising the amino acid sequence of SEQ ID NO:50; (e) a light chain CDR2 comprising the amino acid sequence of SEQ ID NO:51, (f) a light chain CDR3 comprising the amino acid sequence of SEQ ID NO:52.
8. The combined preparation for use according to claim 1, wherein the iron chelator is DFO or DFX.
9. The combined preparation for use according to claims 1 to 7, wherein the cancer is selected from the following group but not limited to: pancreatic cancer, neuroblastoma, solid cancer, leukemia, lymphoma, glioblastoma, breast cancer, cancer related cachexia, gastrointestinal cancer such as colorectal cancer, cholangiocarcinoma, carcinoma of the oral cavity, gastric cancer, Lung cancer such as small cell lung cancer, lung adenocarcinoma, Melanoma, Multiple myeloma, ovarian cancer, prostate cancer, renal cancer, hepatocarcinoma.
10. The combined preparation for use according to claims 1 to 7, wherein the resistant cancer is selected from the group consisting of but not limited to pancreatic cancer, neuroblastoma, colon cancer, liver cancer, leukemia (including erythroleukemia), lymphoma, glioblastoma.
11. An i) antibody anti- transferrin receptor 1 (TfRl), ii) an irion chelator and iii) a chemotherapeutic agent for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
12. An i) antibody anti- transferrin receptor 1 (TfRl), ii) an iron chelator and iii) an immune check point inhibitor for simultaneous, separate or sequential use in the treatment of cancers, as a combined preparation.
13. A pharmaceutical composition comprising the combined preparation according to claims 1 to 12.
14. The pharmaceutical composition according to claim 13 is for use in the treatment of cancer.
15. A method for treating cancer and resistant cancers in a subject in need thereof comprising a step of administering said subject with a therapeutically amount of i) an antibody anti- transferrin receptor 1 (TfRl) and ii) an iron chelator, as a combined preparation.
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP18306821 | 2018-12-21 | ||
| EP18306821.2 | 2018-12-21 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2020127885A1 true WO2020127885A1 (en) | 2020-06-25 |
Family
ID=65234358
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/EP2019/086546 Ceased WO2020127885A1 (en) | 2018-12-21 | 2019-12-20 | Compositions for treating cancers and resistant cancers |
Country Status (1)
| Country | Link |
|---|---|
| WO (1) | WO2020127885A1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN118121604A (en) * | 2024-05-07 | 2024-06-04 | 四川成都中农大现代农业产业研究院 | Composition of epigallocatechin gallate and application of composition as copper ion carrier anti-liver cancer sensitizer |
Citations (42)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4816567A (en) | 1983-04-08 | 1989-03-28 | Genentech, Inc. | Recombinant immunoglobin preparations |
| EP0368684A1 (en) | 1988-11-11 | 1990-05-16 | Medical Research Council | Cloning immunoglobulin variable domain sequences. |
| EP0404097A2 (en) | 1989-06-22 | 1990-12-27 | BEHRINGWERKE Aktiengesellschaft | Bispecific and oligospecific, mono- and oligovalent receptors, production and applications thereof |
| WO1993011161A1 (en) | 1991-11-25 | 1993-06-10 | Enzon, Inc. | Multivalent antigen-binding proteins |
| WO1994025066A1 (en) * | 1993-04-29 | 1994-11-10 | The University Of Iowa | COMBINED TREATMENT OF IRON DEPLETION AND IgG ANTIBODY |
| WO1996019238A1 (en) * | 1994-12-19 | 1996-06-27 | The University Of Iowa Research Foundation | COMBINED TREATMENT OF IRON DEPLETION AND IgG ANTIBODY |
| US6075181A (en) | 1990-01-12 | 2000-06-13 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| US6150584A (en) | 1990-01-12 | 2000-11-21 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| WO2003063792A2 (en) | 2002-01-30 | 2003-08-07 | The Brigham And Women's Hospital, Inc. | Compositions and methods related to tim-3, a th1-specific cell surface molecule |
| WO2004004771A1 (en) | 2002-07-03 | 2004-01-15 | Ono Pharmaceutical Co., Ltd. | Immunopotentiating compositions |
| WO2004056875A1 (en) | 2002-12-23 | 2004-07-08 | Wyeth | Antibodies against pd-1 and uses therefor |
| US6982321B2 (en) | 1986-03-27 | 2006-01-03 | Medical Research Council | Altered antibodies |
| WO2006003388A2 (en) | 2004-06-30 | 2006-01-12 | Domantis Limited | Compositions and methods for treating inflammatory disorders |
| WO2006030220A1 (en) | 2004-09-17 | 2006-03-23 | Domantis Limited | Compositions monovalent for cd40l binding and methods of use |
| US7087409B2 (en) | 1997-12-05 | 2006-08-08 | The Scripps Research Institute | Humanization of murine antibody |
| WO2006121168A1 (en) | 2005-05-09 | 2006-11-16 | Ono Pharmaceutical Co., Ltd. | Human monoclonal antibodies to programmed death 1(pd-1) and methods for treating cancer using anti-pd-1 antibodies alone or in combination with other immunotherapeutics |
| WO2007005874A2 (en) | 2005-07-01 | 2007-01-11 | Medarex, Inc. | Human monoclonal antibodies to programmed death ligand 1 (pd-l1) |
| US7432059B2 (en) | 2000-06-28 | 2008-10-07 | Dana-Farber Cancer Institute, Inc. | Methods of identifying compounds that upmodulate T cell activation in the presence of a PD-1 mediated signal |
| WO2008156712A1 (en) | 2007-06-18 | 2008-12-24 | N. V. Organon | Antibodies to human programmed death receptor pd-1 |
| WO2009033176A1 (en) * | 2007-09-07 | 2009-03-12 | The Trustees Of The University Of Pennsylvania | A method of targeting a transferrin receptor |
| WO2009054864A1 (en) | 2007-10-26 | 2009-04-30 | Rigel Pharmaceuticals, Inc. | Polycyclic aryl substituted triazoles and polycyclic heteroaryl substituted triazoles useful as axl inhibitors |
| WO2009114335A2 (en) | 2008-03-12 | 2009-09-17 | Merck & Co., Inc. | Pd-1 binding proteins |
| WO2010036959A2 (en) | 2008-09-26 | 2010-04-01 | Dana-Farber Cancer Institute | Human anti-pd-1, pd-l1, and pd-l2 antibodies and uses therefor |
| WO2010077634A1 (en) | 2008-12-09 | 2010-07-08 | Genentech, Inc. | Anti-pd-l1 antibodies and their use to enhance t-cell function |
| WO2010089411A2 (en) | 2009-02-09 | 2010-08-12 | Universite De La Mediterranee | Pd-1 antibodies and pd-l1 antibodies and uses thereof |
| WO2010117057A1 (en) | 2009-04-10 | 2010-10-14 | 協和発酵キリン株式会社 | Method for treatment of blood tumor using anti-tim-3 antibody |
| WO2011066389A1 (en) | 2009-11-24 | 2011-06-03 | Medimmmune, Limited | Targeted binding agents against b7-h1 |
| WO2011082400A2 (en) | 2010-01-04 | 2011-07-07 | President And Fellows Of Harvard College | Modulators of immunoinhibitory receptor pd-1, and methods of use thereof |
| WO2011110621A1 (en) | 2010-03-11 | 2011-09-15 | Ucb Pharma, S.A. | Biological products: humanised agonistic anti-pd-1 antibodies |
| WO2011155607A1 (en) | 2010-06-11 | 2011-12-15 | 協和発酵キリン株式会社 | Anti-tim-3 antibody |
| WO2013006490A2 (en) | 2011-07-01 | 2013-01-10 | Cellerant Therapeutics, Inc. | Antibodies that specifically bind to tim3 |
| WO2013079174A1 (en) | 2011-11-28 | 2013-06-06 | Merck Patent Gmbh | Anti-pd-l1 antibodies and uses thereof |
| US8617546B2 (en) | 2008-10-02 | 2013-12-31 | Seoul National University Industry Foundation | Anticancer agent comprising anti-PD-1 antibody or anti-PD-L1 antibody |
| WO2014055897A2 (en) | 2012-10-04 | 2014-04-10 | Dana-Farber Cancer Institute, Inc. | Human monoclonal anti-pd-l1 antibodies and methods of use |
| WO2014055648A1 (en) | 2012-10-02 | 2014-04-10 | Bristol-Myers Squibb Company | Combination of anti-kir antibodies and anti-pd-1 antibodies to treat cancer |
| WO2014150677A1 (en) | 2013-03-15 | 2014-09-25 | Bristol-Myers Squibb Company | Inhibitors of indoleamine 2,3-dioxygenase (ido) |
| WO2014194302A2 (en) | 2013-05-31 | 2014-12-04 | Sorrento Therapeutics, Inc. | Antigen binding proteins that bind pd-1 |
| WO2014195852A1 (en) | 2013-06-03 | 2014-12-11 | Glaxosmithkline Intellectual Property (No.2) Limited | Combinations of an anti-pd-l1 antibody and a mek inhibitor and/or a braf inhibitor |
| WO2015035606A1 (en) | 2013-09-13 | 2015-03-19 | Beigene, Ltd. | Anti-pd1 antibodies and their use as therapeutics and diagnostics |
| WO2015048520A1 (en) | 2013-09-27 | 2015-04-02 | Genentech, Inc. | Anti-pdl1 antibody formulations |
| WO2015117002A1 (en) | 2014-01-31 | 2015-08-06 | Novartis Ag | Antibody molecules to tim-3 and uses thereof |
| WO2016179257A2 (en) * | 2015-05-04 | 2016-11-10 | Cytomx Therapeutics, Inc. | Anti-cd71 antibodies, activatable anti-cd71 antibodies, and methods of use thereof |
-
2019
- 2019-12-20 WO PCT/EP2019/086546 patent/WO2020127885A1/en not_active Ceased
Patent Citations (44)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4816567A (en) | 1983-04-08 | 1989-03-28 | Genentech, Inc. | Recombinant immunoglobin preparations |
| US6982321B2 (en) | 1986-03-27 | 2006-01-03 | Medical Research Council | Altered antibodies |
| EP0368684A1 (en) | 1988-11-11 | 1990-05-16 | Medical Research Council | Cloning immunoglobulin variable domain sequences. |
| EP0404097A2 (en) | 1989-06-22 | 1990-12-27 | BEHRINGWERKE Aktiengesellschaft | Bispecific and oligospecific, mono- and oligovalent receptors, production and applications thereof |
| US6075181A (en) | 1990-01-12 | 2000-06-13 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| US6150584A (en) | 1990-01-12 | 2000-11-21 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| WO1993011161A1 (en) | 1991-11-25 | 1993-06-10 | Enzon, Inc. | Multivalent antigen-binding proteins |
| WO1994025066A1 (en) * | 1993-04-29 | 1994-11-10 | The University Of Iowa | COMBINED TREATMENT OF IRON DEPLETION AND IgG ANTIBODY |
| WO1996019238A1 (en) * | 1994-12-19 | 1996-06-27 | The University Of Iowa Research Foundation | COMBINED TREATMENT OF IRON DEPLETION AND IgG ANTIBODY |
| US7087409B2 (en) | 1997-12-05 | 2006-08-08 | The Scripps Research Institute | Humanization of murine antibody |
| US7709214B2 (en) | 2000-06-28 | 2010-05-04 | Dana-Farber Cancer Institute, Inc. | Methods for upregulating an immune response with agents that inhibit the intereaction between PD-L2 and PD-1 |
| US7432059B2 (en) | 2000-06-28 | 2008-10-07 | Dana-Farber Cancer Institute, Inc. | Methods of identifying compounds that upmodulate T cell activation in the presence of a PD-1 mediated signal |
| WO2003063792A2 (en) | 2002-01-30 | 2003-08-07 | The Brigham And Women's Hospital, Inc. | Compositions and methods related to tim-3, a th1-specific cell surface molecule |
| WO2004004771A1 (en) | 2002-07-03 | 2004-01-15 | Ono Pharmaceutical Co., Ltd. | Immunopotentiating compositions |
| WO2004056875A1 (en) | 2002-12-23 | 2004-07-08 | Wyeth | Antibodies against pd-1 and uses therefor |
| WO2006003388A2 (en) | 2004-06-30 | 2006-01-12 | Domantis Limited | Compositions and methods for treating inflammatory disorders |
| WO2006030220A1 (en) | 2004-09-17 | 2006-03-23 | Domantis Limited | Compositions monovalent for cd40l binding and methods of use |
| WO2006121168A1 (en) | 2005-05-09 | 2006-11-16 | Ono Pharmaceutical Co., Ltd. | Human monoclonal antibodies to programmed death 1(pd-1) and methods for treating cancer using anti-pd-1 antibodies alone or in combination with other immunotherapeutics |
| WO2007005874A2 (en) | 2005-07-01 | 2007-01-11 | Medarex, Inc. | Human monoclonal antibodies to programmed death ligand 1 (pd-l1) |
| WO2008156712A1 (en) | 2007-06-18 | 2008-12-24 | N. V. Organon | Antibodies to human programmed death receptor pd-1 |
| WO2009033176A1 (en) * | 2007-09-07 | 2009-03-12 | The Trustees Of The University Of Pennsylvania | A method of targeting a transferrin receptor |
| WO2009054864A1 (en) | 2007-10-26 | 2009-04-30 | Rigel Pharmaceuticals, Inc. | Polycyclic aryl substituted triazoles and polycyclic heteroaryl substituted triazoles useful as axl inhibitors |
| WO2009114335A2 (en) | 2008-03-12 | 2009-09-17 | Merck & Co., Inc. | Pd-1 binding proteins |
| WO2010036959A2 (en) | 2008-09-26 | 2010-04-01 | Dana-Farber Cancer Institute | Human anti-pd-1, pd-l1, and pd-l2 antibodies and uses therefor |
| US8552154B2 (en) | 2008-09-26 | 2013-10-08 | Emory University | Anti-PD-L1 antibodies and uses therefor |
| US8617546B2 (en) | 2008-10-02 | 2013-12-31 | Seoul National University Industry Foundation | Anticancer agent comprising anti-PD-1 antibody or anti-PD-L1 antibody |
| WO2010077634A1 (en) | 2008-12-09 | 2010-07-08 | Genentech, Inc. | Anti-pd-l1 antibodies and their use to enhance t-cell function |
| WO2010089411A2 (en) | 2009-02-09 | 2010-08-12 | Universite De La Mediterranee | Pd-1 antibodies and pd-l1 antibodies and uses thereof |
| WO2010117057A1 (en) | 2009-04-10 | 2010-10-14 | 協和発酵キリン株式会社 | Method for treatment of blood tumor using anti-tim-3 antibody |
| WO2011066389A1 (en) | 2009-11-24 | 2011-06-03 | Medimmmune, Limited | Targeted binding agents against b7-h1 |
| WO2011082400A2 (en) | 2010-01-04 | 2011-07-07 | President And Fellows Of Harvard College | Modulators of immunoinhibitory receptor pd-1, and methods of use thereof |
| WO2011110621A1 (en) | 2010-03-11 | 2011-09-15 | Ucb Pharma, S.A. | Biological products: humanised agonistic anti-pd-1 antibodies |
| WO2011155607A1 (en) | 2010-06-11 | 2011-12-15 | 協和発酵キリン株式会社 | Anti-tim-3 antibody |
| WO2013006490A2 (en) | 2011-07-01 | 2013-01-10 | Cellerant Therapeutics, Inc. | Antibodies that specifically bind to tim3 |
| WO2013079174A1 (en) | 2011-11-28 | 2013-06-06 | Merck Patent Gmbh | Anti-pd-l1 antibodies and uses thereof |
| WO2014055648A1 (en) | 2012-10-02 | 2014-04-10 | Bristol-Myers Squibb Company | Combination of anti-kir antibodies and anti-pd-1 antibodies to treat cancer |
| WO2014055897A2 (en) | 2012-10-04 | 2014-04-10 | Dana-Farber Cancer Institute, Inc. | Human monoclonal anti-pd-l1 antibodies and methods of use |
| WO2014150677A1 (en) | 2013-03-15 | 2014-09-25 | Bristol-Myers Squibb Company | Inhibitors of indoleamine 2,3-dioxygenase (ido) |
| WO2014194302A2 (en) | 2013-05-31 | 2014-12-04 | Sorrento Therapeutics, Inc. | Antigen binding proteins that bind pd-1 |
| WO2014195852A1 (en) | 2013-06-03 | 2014-12-11 | Glaxosmithkline Intellectual Property (No.2) Limited | Combinations of an anti-pd-l1 antibody and a mek inhibitor and/or a braf inhibitor |
| WO2015035606A1 (en) | 2013-09-13 | 2015-03-19 | Beigene, Ltd. | Anti-pd1 antibodies and their use as therapeutics and diagnostics |
| WO2015048520A1 (en) | 2013-09-27 | 2015-04-02 | Genentech, Inc. | Anti-pdl1 antibody formulations |
| WO2015117002A1 (en) | 2014-01-31 | 2015-08-06 | Novartis Ag | Antibody molecules to tim-3 and uses thereof |
| WO2016179257A2 (en) * | 2015-05-04 | 2016-11-10 | Cytomx Therapeutics, Inc. | Anti-cd71 antibodies, activatable anti-cd71 antibodies, and methods of use thereof |
Non-Patent Citations (9)
| Title |
|---|
| AGNEW CHEM INTL. ED. ENGL., vol. 33, 1994, pages 183 - 186 |
| BOGDAN ALEXANDER R ET AL: "Regulators of Iron Homeostasis: New Players in Metabolism, Cell Death, and Disease", TRENDS IN BIOCHEMICAL SCIENCES, vol. 41, no. 3, 1 March 2016 (2016-03-01), pages 274 - 286, XP029451529, ISSN: 0968-0004, DOI: 10.1016/J.TIBS.2015.11.012 * |
| J D KEMP: "Iron deprivation and cancer: a view beginning with studies of monoclonal antibodies against the transferrin receptor", HISTOL HISTOPATHOL, vol. 12, no. 1, 1 January 1997 (1997-01-01), pages 291 - 296, XP055588876, DOI: 10.14670/HH-12.291 * |
| LAURA PANDOLFI ET AL: "H-Ferritin Enriches the Curcumin Uptake and Improves the Therapeutic Efficacy in Triple Negative Breast Cancer Cells", BIOMACROMOLECULES, vol. 18, no. 10, 19 September 2017 (2017-09-19), US, pages 3318 - 3330, XP055588777, ISSN: 1525-7797, DOI: 10.1021/acs.biomac.7b00974 * |
| MADELINE NEIVEYANS ET AL: "A recycling anti-transferrin receptor-1 monoclonal antibody as an efficient therapy for erythroleukemia through target up-regulation and antibody-dependent cytotoxic effector functions", MABS, vol. 11, no. 3, 3 April 2019 (2019-04-03), US, pages 593 - 605, XP055585372, ISSN: 1942-0862, DOI: 10.1080/19420862.2018.1564510 * |
| MELLMAN ET AL., NATURE, vol. 480, 2011, pages 480 - 489 |
| PARDOLL, NATURE REV CANCER, vol. 12, 2012, pages 252 - 264 |
| RANA MELHEM: "Ciblage du récepteur de la transferrine de type 1 (TfR1) et du métabolisme du Fer dans le cancer du pancréas", 10 July 2017 (2017-07-10), XP055581698, Retrieved from the Internet <URL:http://www.biu-montpellier.fr/florabium/jsp/tools/print/print_record_with_template.jsp> [retrieved on 20190416] * |
| SUZY V. TORTI ET AL: "Iron and cancer: more ore to be mined", NATURE REVIEWS. CANCER, vol. 13, no. 5, 18 April 2013 (2013-04-18), GB, pages 342 - 355, XP055301024, ISSN: 1474-175X, DOI: 10.1038/nrc3495 * |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN118121604A (en) * | 2024-05-07 | 2024-06-04 | 四川成都中农大现代农业产业研究院 | Composition of epigallocatechin gallate and application of composition as copper ion carrier anti-liver cancer sensitizer |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US12534530B2 (en) | Combination of a PD-1 antagonist and a VEGFR inhibitor for treating cancer | |
| EP3102604B1 (en) | Combination of a pd-1 antagonist and a 4-1bb agonist for treating cancer | |
| CA2978226C (en) | Combination of a pd-1 antagonist and a vegfr/fgfr/ret tyrosine kinase inhibitor for treating cancer | |
| WO2020104479A1 (en) | Methods and compositions for treating cancers and resistant cancers with anti transferrin receptor 1 antibodies | |
| AU2015264528A1 (en) | Combination of an anti-CCR4 antibody and a 4-1BB agonist for treating cancer | |
| WO2017091429A1 (en) | Combination therapy for cancer | |
| EP3411076A1 (en) | ANTIBODY-DRUG CONJUGATES TARGETING uPARAP | |
| AU2019346012A1 (en) | Combination of a PD-1 antagonist, an ATR inhibitor and a platinating agent for the treatment of cancer | |
| WO2020127885A1 (en) | Compositions for treating cancers and resistant cancers | |
| US20220354811A1 (en) | Methods and compositions for modulating macrophages polarization | |
| US20230159635A1 (en) | Medicament for treatment and/or prevention of cancer | |
| US20230322929A1 (en) | Compositions and Methods for Treating Solid Tumors with Anti-BTLA as Mono or Combination Therapy | |
| WO2024208253A1 (en) | Compositions and methods for treating solid tumors with anti-btla as combination therapy | |
| EP4578459A1 (en) | Pharmaceutical product for treatment and/or prevention of cancer | |
| EP4578458A1 (en) | Medicament for treatment and/or prevention of cancer | |
| RU2802962C2 (en) | Compositions and methods of treatment of liver cancer | |
| KR20250054778A (en) | Medicines for the treatment and/or prevention of cancer | |
| WO2024194692A1 (en) | Tgf-beta inhibitor for use in the treatment of dedifferentiated liposarcoma | |
| KR20250118852A (en) | Medicines for the treatment and/or prevention of cancer | |
| KR20240135691A (en) | Method for treating cancer using ketotifen in combination with a checkpoint inhibitor | |
| WO2023041744A1 (en) | Bet inhibitors for treating pab1 deficient cancer | |
| CN119768182A (en) | Drugs for the treatment and/or prevention of cancer |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 19827739 Country of ref document: EP Kind code of ref document: A1 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| 122 | Ep: pct application non-entry in european phase |
Ref document number: 19827739 Country of ref document: EP Kind code of ref document: A1 |