www.wales.nhs.
uk
Stroke & TIA
Dr Rebecca Chave-Cox Countdown 2 Finals, 2013
�Objectives
Define & differentiate stroke & TIA
Cover the basic epidemiology & aetiology
Discuss clinical presentations
Correlate symptoms to anatomical location
Learn to assess the patient
Discuss management
�Definition
Clinical diagnosis Stroke:
Focal, non-convulsive neurological deficit due to
vascular lesion with symptoms lasting over 24h (if pt survives)
Transient Ischaemic Attack:
Focal, non-convulsive, neurological deficit lasting
less than 24h with complete clinical recovery
�Stroke
The most common presentation is hemiplegia
85% caused by thromboembolic vascular occlusion Haemorrhagic strokes are often secondary to chronic
HTN (leading to rupture of microaneurysms)
Late deterioration after a stroke can be due to
'haemorrhagic transformation' post the acute event
�TIA
Symptoms are usually of sudden onset, often
recurrent & repeat episodes are often stereotypical
Maximum deficit reached in <1m Due to focal hypoperfusion in the brain Up to 20% patients will have a subsequent stroke
within 90 days (half of these in first 2 days)
Prompt investigation & management is essential
�Epidemiology
Commonest cause of adult disability 12% all deaths 5% NHS budget Stroke incidence = 150-200 per 100,000/yr TIA incidence = 30 cases per 100,000/yr Incidence rates increase with advancing age
�Prognosis of stroke
1/3 die, 1/3 recover well, 1/3 remain disabled
Mortality: 10% in first week 20% in first month 30% in first year
Worse prognosis:
coma defects in conjugate gaze with hemiplegia severe hemiplegia
Intracerebral haemorrhage has greater mortality but better functional recovery from acute, severe deficits
�Common aetiologies
Atherosclerosis
Cardiac or carotid embolism
Arterial dissection Intracerebral haemorrhage Lipohyalinosis of small arteries
�Risk Factors
H - Hypertension: major RF for both ischaemic & haemorrhagic stroke A - cArdiac: Cardiac causes (AF, Arrhythmias, cardiomyopathy, valve disease etc linked to embolism) & coronary Artery disease is marker for atherosclerosis elsewhere L - hyperLipidaemia: less significant than in coronary artery disease
T - Tobacco: quitting lowers risk of stroke
S - Sugar (diabetes mellitus): 2x increased cerebral infection risk & RF for atherosclerosis Homocysteine Family history: close family members at slightly increased risk, but DM & HTN also familial Obesity & diet: probably less important than in coronary artery disease
Oral contraceptive pill: may increase risk of thromboembolic stroke, central venous thrombosis & subarachnoid haemorrhage in the vulnerable
�Primary intracerebral haemorrhage
Commonly due to chronic hypertension; small vessel disease,
aneurysms; AVMs; bleeding disorders & cerebral amyloid angiopathy
In the context of chronic hypertension >70% haemorrhages
occur in the internal capsule or basal ganglia due to CharcotBouchard aneurysms
But, can occur in any part of the cortex, pons or cerebellum Clinical signs vary by location but often associated with mass
effect with reduced consciousness
Otherwise, very hard to distinguish from an infarct
�Localisation
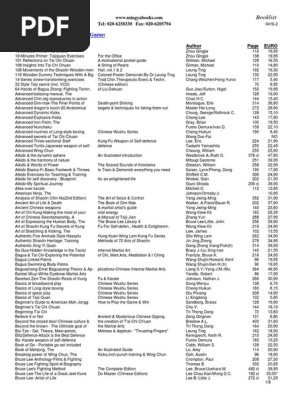
�Arterial supply
Posterior communicating artery Posterior cerebral artery Basilar artery Junction of vertebral arteries
External carotid Internal carotid Vertebral artery Common carotid
http://en.wikipedia.org/wiki/File:Vertebral_artery.png {Grays Anatomy plate}
�Circle of Willis
www.meducation.net/encyclopedia/27006
�Vascular territories
http://missinglink.ucsf.edu
�Middle cerebral artery occlusion
MCA is the artery most commonly involved in stroke Largest branch of the internal carotid & supplies the largest area of cerebral cortex Wernicke's & Broca's are found in the dominant hemisphere, therefore in most individuals speech will only be affected by a left MCA occlusion Non-dominant lesions cause visuospatial problems eg inattention Initially limbs are flaccid & areflexic; then reflexes recover & exaggerate; plantar responses become extensor and spastic limb tone develops There is variable weakness over days, weeks or months
�Middle cerebral artery
Contralateral hemiplegia
Contralateral hemisensory loss
Contralateral homonymous hemianopia
Dominant hemisphere: aphasia
Non-dominant hemisphere: neglect of contralateral
limb, dressing apraxia
�Middle cerebral artery
Both sides Dominant Wernickes (speech comprehension) Brocas (speech expression) Non-dominant
Motor cortex
Visuospatial
Sensory cortex
Hemianopia
�Visual field defects
http://medical-dictionary.thefreedictionary.com/homonymous+hemianopia
�Anterior cerebral artery
Pure ACA stroke is uncommon Proximal occlusion is usually well tolerated with few symptoms Distal occlusion causes:
Contralateral weakness
Contralateral sensory loss in leg
Incontinence
Occasionally there is a contralateral grasp, or other primitive reflexes
�Lacunar stroke
25% ischaemic strokes
Infarction of internal capsule
Pure hemiparesis
Hemisensory loss
Ataxic hemiparesis
Clumsy hand - dysarthria syndrome
�Opthalmic artery
Amourosis fugax
�Posterior cerebral artery occlusion
The PCAs are the terminal branches of the basilar
artery
The PCAs send cortical branches to the temporal lobe,
occipital lobe & visual cortex as well as perforating branches to the midbrain & thalamus
The effect of the occlusion depends on the site and is
associated with specific syndromes
�Posterior cerebral artery occlusion
Homonymous hemianopia with macula sparring
(which is supplied by MCA)
Complete visual loss with reduced/no insight Ipsilateral third nerve palsy with contralateral
hemiplegia
�Lateral medullary syndrome
Specific brainstem syndromes
Also known as posterior inferior cerebellar artery syndrome
The most widely recognised brainstem syndrome Sudden onset vertigo, vomiting & nystagmus Ipsilateral ataxia (cerebellar connections) Ipsilateral facial numbness (5th CN descending tract) Ipsilateral Horner's syndrome (sympathetic tract) Contralateral loss of pain & temperature sensation in limbs (ascending spinothalamic tract)
Dysarthria & dysphagia (10th CN)
�'Locked-in' syndrome
Specific brainstem syndromes
Due to bilateral infarction of ventral pons with or
without medullary involvement
Patient is conscious
However they are mute & paralysed
Patients can often move their eyes due to sparing of
the 3rd & 4th CN nuclei in the midbrain
�Assessment & Diagnosis
History
Onset - spread of symptoms; warning TIA? Focal symptoms - language/motor/sensory/visual
Headache? - if severe & progressive may indicate haemorrhage
Progressive consciousness impairment: suggests raised ICP secondary to haemorrhage; complete anterior circulation infarct or coning secondary to cerebellar haemorrhage Risk factors PMH: prev TIA/stroke, connective tissue disease, neoplasia, bleeding disorders, arrhythmias & cardiac disease DHx: especially for anticoagulants and oral contraceptive pill Normal functional levels: ADLs
�Examination
CVS:
embolus (pulse for AF, bruits esp carotid, valve lesion, signs of endocarditis) hypertension (BP, lying & standing) stenosis (asymmetric brachial BPs, pulse delay)
Chest:
Neuro:
pneumonia standard (cranial nerves & vision; limbs) GCS swallow
�Differential diagnosis for acute stroke
Stroke
Seizure Systemic infection Brain tumour Toxic-metabolic
Most likely
Least likely
�Basic Investigations
FBC: polycythaemia, infection
ESR & CRP: inflammatory disease Urinalysis & blood sugar: diabetes mellitus Cholesterol Blood culture: if suspect endocarditis or superadded infection Autoantibodies & coagulation studies: in young patients connective tissue disorder or prothrombotic disorder ECG/echo: arrhythmia; myocardial infection/ischaemia
Chest X-ray: heart failure; neoplasia
�Neuroimaging
All stroke patients should have a CT scan <24h to
differentiate ischaemia & haemorrhage
MRI needed if lesion clinically placed in posterior
fossa (ie brainstem & cerebellum)
MRI also better at detecting small strokes
�Vascular imaging
Carotid doppler: Effective, non-invasive demonstration of internal carotid artery stenosis when carotid bruit heard or carotid thromboembolism suspected
CTA & MRA CT & MR angiography (CTA & MRA) can help visualise carotids & posterior circulation for atheromatous disease, dissections & aneurysms
Angiography: Used to locate intracerebral aneurysms and diagnose cerebral vasculitides which are poorly detected on MRA Do not consider in first 2 weeks after acute stroke
�Management
Management of acute stroke
Establish initial diagnosis Admit directly to HASU Reopen artery (thrombolysis with alteplase) <4.5 hrs only
Prevent early recurrence
Aspirin 300mg for all ischaemic strokes Avoid anticoagulation (heparin) unless specifically indicated
Give clopidigrel instead of aspirin if there are co-morbidities
Protect from secondary brain damage Maintain physiology
Treat complications, including craniotomy for MCA oedema
�Complications of acute stroke
Neurological:
Non-neurological:
Cerebral oedema
Completion of stroke Early recurrence Haemorrhagic transformation Obstructive hydrocephalus Seizures Incorrect diagnosis
Infection Metabolic Drugs Hypoxia/hypercapnia
Large 'malignant' MCA territory infarcts are the commonest cause of death in the first week (peaks at 24h & 4-5 days) Severe hemispheric stroke syndrome; hemiplegia; forced eye & head deviation; progressive deterioration within 1st 2 days CT signs of infarct within 12 hours 80% mortality
Transtentorial herniation & cerebral oedema
Steroids have no effect on outcome Mannitol has no effect on outcome but may stabilise rapidly deteriorating patient Early hemicraniectomy improves survival & functional outcome almost threefold (NNT=2)
�Management of completed stroke
Prevent complications
Rehabilitation
Control hypertension if >220/120 Give aspirin (300mg)/dipyridamole or clopidogrel
Control cholesterol
Smoking cessation advice Good glycaemic control Remove/treat embolic source (nb no anticoagulation in 1st 7 days even if indicated for cardiac embolus) Treat inflammatory or connective tissue disorders
Stop thrombogenic drugs
Carotid endarterectomy
Disadvantages of a procedure: Significant risk of inducing stroke Risk of CN palsy or cardiac event Neck incision/haematoma
Cost & inconvenience
Criteria for intervention: 70% or more stenosis of internal carotid artery ipsilateral to affected cortex (contralateral to symptoms) 50-69% stenosis considered <50% stenosis not suitable for surgery
�Management of TIA
Confirm diagnosis (history & examination) Refer immediately to A&E for any 1 of the following: Symptoms present at time of assessment ABCD2 score 4 or more & within 7 days of symptoms
Patient in AF
Patient with recurrent TIAs
ALL other patients should be seen in the Rapid Access TIA
clinics
�ABCD2 Score
Criteria Age Qualifier 60 yrs + Points 1
Under 60
BP Over 140 Under 90 Clinical features Unilat weakness Speech disturbance only
0
1 0 2 1
Other
Duration of Sx Over 1 hour 10-59 mins Under 10 mins Diabetes
0
2 1 0 1
�Management of TIA
Identify & treat risk factors
Aspirin/dipyridamole or clopidogrel Avoid anticoagulants (heparin/warfarin) in the short
term unless clear need eg AF
Investigate possible sites for primary lesion (eg
carotid stenosis, cardiac embolus 2ndry to AF)
�Driving
Patients with suspected TIA or stroke must not drive
for 1 month
Can automatically resume driving if no residual
deficit at 1 month
Drivers with multiple TIAs in a short time may
require 3 months away from driving
�Primary & secondary prevention
Primary prevention: stops a disease from happening
Secondary prevention: stops recurrence of a disease
�Lifestyle interventions
Physical activity Weight reduction
Low salt, sugar, saturated fat diet
Less (or no) smoking or alcohol
�Medical interventions
Aim for BP <130/80
Clopidogrel monotherapy or aspirin/dipyridamole
dual therapy
Statins Warfarin - for people in AF (major cause of stroke);
only start 2 weeks after stroke to avoid haemorrhage
Good glycaemic control
Summary
Stroke is a clinical diagnosis and the commonest cause of adult disability in the UK
1/3 die, 1/3 recover, 1/3 remain disabled
Prompt recognition and referral to HASU is key High dose aspirin/dipyridamole or clopidogrel Thrombolyse ischaemic strokes within 4.5 hours (if no CI) Modify risk factors
High risk of stroke in days/weeks following TIA
Refer straight to A&E if high risk All other TIA patients should be seen in Rapid Access TIA clinic
�References
Oxford Handbook of Clinical Medicine
Pocket Essentials of Clinical Medicine 4th Ed, Ballinger & Patchett (Kumar & Clarke) SIGN: Management of patients with stroke or TIA: assessment, investigation, immediate management and secondary prevention (www.sign.ac.uk/guidelines/fulltext/108/index.html) NICE guidance CG68: Diagnosis and initial management of acute stroke and transient ischaemic attack (TIA) July 2008 (www.nice.org.uk/CG68) LTHT TIA guidelines (LGI/SJUH intranet) GP notebook (www.gpnotebook.co.uk DVLA (www.dvla.gov.uk) About.com (http://stroke.about.com) The Neurosurgeons Handbook, Samandouras
�Questions?