Brain Advance Access published October 7, 2008
doi:10.1093/brain/awn238
Brain (2008) Page 1 of 13
Bilateral subthalamic stimulation impairs
cognitive ^motor performance in Parkinson’s
disease patients
Jay L. Alberts,1,2,3 Claudia Voelcker-Rehage,4 Katie Hallahan,1 Megan Vitek,1 Rashi Bamzai1
and Jerrold L. Vitek2,5
1
Department of Biomedical Engineering, Cleveland Clinic, 2Center for Neurological Restoration, Cleveland Clinic,
Cleveland FES Center, L. Stokes Cleveland VA Medical Center, Cleveland, OH, USA, 4Jacobs Center on Lifelong Learning
and Institutional Development, Jacobs University, Bremen, Germany and 5Department of Neuroscience, Cleveland Clinic,
Cleveland, OH, USA
3
Deep brain stimulation (DBS) is a surgical procedure that has been shown effective in improving the cardinal
motor signs of advanced Parkinson’s disease, however, declines in cognitive function have been associated with
bilateral subthalamic nucleus (STN) DBS. Despite the fact that most activities of daily living clearly have motor
and cognitive components performed simultaneously, postoperative assessments of cognitive and motor function occur, in general, in isolation of one another. The primary aim of this study was to determine the effects of
unilateral and bilateral STN DBS on upper extremity motor function and cognitive performance under singleand dual-task conditions in advanced Parkinson’s disease patients. Data were collected from eight advanced
Parkinson’s disease patients between the ages of 48 and 70 years (mean 56.5) who had bilaterally placed STN
stimulators. Stimulation parameters for DBS devices were optimized clinically and were stable for at least
6 months prior to study participation. Data were collected while patients were Off anti-parkinsonian medications under three stimulation conditions: Off stimulation, unilateral DBS and bilateral DBS. In each stimulation
condition patients performed a cognitive (n-back task) and motor (force tracking) task under single- and dualtask conditions. During dual-task conditions, patients performed the n-back and force-maintenance task
simultaneously. Under relatively simple dual-task conditions there were no differences in cognitive or motor
performance under unilateral and bilateral stimulation. As dual-task complexity increased, cognitive and
motor performance was significantly worse with bilateral compared with unilateral stimulation. In the most
complex dual-task condition (i.e. 2-back + force tracking), bilateral stimulation resulted in a level of motor
performance that was similar to the Off stimulation condition. Significant declines in cognitive and motor function under modest dual-task conditions with bilateral but not with unilateral STN DBS suggest that unilateral
procedures may be an alternative to bilateral DBS for some patients, in particular, those with asymmetric
symptomology. From a clinical perspective, these results underscore the need to assess cognitive and motor
function simultaneously during DBS programming as these conditions may better reflect the context in which
daily activities are performed.
Keywords: Parkinson’s disease; deep brain stimulation; force control; cognitive function; dual-task
Abbreviations: DBS = deep brain stimulation; DTL = dual-task loss; GPi = globus pallidus internus; RRMSE = relative root
mean square error; STN = subthalamic nucleus; TWR = time within the target range; VTA = volume of tissue activated
Received March 27, 2008. Revised August 27, 2008. Accepted August 29, 2008
ß The Author (2008). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oxfordjournals.org
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
Correspondence to: Jay L. Alberts, Department of Biomedical Engineering/ND20, Center for Neurological Restoration,
Cleveland Clinic, 9500 Euclid Ave, Cleveland, OH 44195, USA
E-mail: albertj@ccf.org
�Page 2 of 13
Brain (2008)
Introduction
The impacts of a decline in cognitive resources
(e.g. working memory) in Parkinson’s disease patients and
the effects of bilateral STN DBS on these resources and the
motor functioning of Parkinson’s disease patients have not
been well documented. Bilateral STN DBS has been shown
to improve reaction time in Parkinson’s disease patients
using a simple reaction time paradigm (Temel et al.,
2006a). However, bilateral STN did not improve reaction
time when these same patients completed a choice or
complex reaction time task. The absence of an improvement in reaction time under more complex conditions may
suggest that bilateral STN DBS may result in ‘cognitive
slowing’ or a decline in information processing capability
(Temel et al., 2006a). More recently, Hershey and
colleagues (2007) assessed spatial working memory during
bilateral and unilateral STN DBS. Declines in spatial
working memory were present with bilateral DBS. During
unilateral stimulation, motor function improved more
when DBS was active in the more affected side of the
brain (e.g. contralateral to more affected side) compared
with the less affected side. However, with DBS in the more
affected side of the brain working memory was impaired
compared with stimulation in the less affected side of the
brain. They concluded that unilateral and bilateral STN
DBS can differentially affect cognitive and motor performance (Hershey et al., 2007). These recent data underscore
the importance of using assessment tasks with varying levels
of difficulty (Temel et al., 2006a) and examination of
cognitive and motor effects during both unilateral and
bilateral STN DBS (Hershey et al., 2007). To date, little
consideration has been given to how a decline in cognitive
function, as a result of bilateral STN DBS in particular, may
impact cognitive and motor performance in Parkinson’s
disease patients using a dual-task paradigm; an experimental condition that better replicates the context in which
most daily activities are performed.
Using clinical and objective kinematic measures, we have
shown that unilateral STN DBS, 11–26 months post-DBS
surgery, led to significant improvements in ipsilateral and
contralateral motor function in advanced Parkinson’s
disease patients (Alberts et al., 2004). Our results indicate
that unilateral STN DBS improves the control and
coordination of grasping forces produced by each limb
during the performance of a bimanual dexterity task and
leads to an overall improvement in interlimb coordination
(Alberts et al., 2004) and maximum force produced by each
limb (Alberts et al., 2008). Additional studies provide
clinical confirmation of our findings and indicate unilateral
STN DBS improves motor functioning of both limbs
(Chung et al., 2006; Slowinski et al., 2007; Tabbal et al.,
2008). It is clear that unilateral STN DBS improves
ipsilateral and contralateral motor function in advanced
Parkinson’s disease patients (Alberts et al., 2004; Germano
et al., 2004; Piper et al., 2005; Chung et al., 2006; Slowinski
et al., 2007; Tabbal et al., 2008). The incidence of adverse
neuropsychological effects appears to be less in unilateral
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
Deep brain stimulation (DBS) is a surgical procedure that
has been shown effective in improving the cardinal motor
signs of advanced Parkinson’s disease (The Deep Brain
Stimulation Study Group, 2001). Despite the lack of a clear
consensus, current surgical practice is to implant stimulating electrodes in the subthalamic nucleus (STN) during a
single surgical session (Benabid et al., 2000). Although
effective for Parkinson’s disease motor symptom relief,
short- and long-term reports indicate that bilateral STN
DBS may be associated with significant postoperative
morbidity in the form of cognitive deficits, declines in
working memory, reduced information processing speed
and increased depression and anxiety (Saint-Cyr et al.,
2000; Gironell et al., 2003; Hershey et al., 2004; RodriguezOroz et al., 2005; Schupbach et al., 2005); the following
provide reviews on the neuropsychological effects of DBS
(Voon et al., 2005; Skidmore et al., 2006; Temel et al.,
2006b). In a recent meta-analysis examining the cognitive
sequelae of STN DBS, it was concluded, that while STN
DBS is safe, significant declines in executive function, verbal
learning and memory are associated with bilateral STN DBS
(Parsons et al., 2006). While some neuropsychological
complications associated with bilateral STN DBS such as
depression, anxiety and apathy may be transient or
responsive to medical or behavioural therapy (Voon et al.,
2005), solutions for reversing declines in working memory
and other important cognitive functions that persist
following bilateral STN DBS have not been identified.
A decline in cognitive functioning (e.g. working memory
and attention) has been shown to be an important factor
that contributes to worsening postural stability, an
increased rate of falling (Woollacott and Shumway-Cook,
2002) and decreased manual function in older adults
(Voelcker-Rehage and Alberts, 2005; Voelcker-Rehage et al.,
2006).
Recently, it was shown that, compared with elderly
controls, mild to moderate Parkinson’s disease patients
without DBS produced more errors while driving a car as
part of a route following task (Uc et al., 2007). A potential
explanation for increased driving errors for Parkinson’s
disease patients’ is that they have limited cognitive
resources and when presented with an increase in cognitive
load or task demands (i.e. motor aspect of driving along
with decision-making components of driving) the patients’
performance on one or both tasks degrades. A limited
number of studies have examined the effects of Parkinson’s
disease on dual-task performance. Rochester and colleagues
(2004) studied mild and moderate Parkinson’s disease
patients and found that as overall difficulty of the dual task
increased, single-task performance declined (i.e. decreased
walking speed and step length). These data suggest the basal
ganglia may play an important role in the successful
performance of tasks with both motor and cognitive
components.
J. L. Alberts et al.
�Bilateral DBS impairs dual-task performance
Brain (2008)
compared with bilateral STN DBS (Jahanshahi et al., 2000;
Morrison et al., 2000; Saint-Cyr et al., 2000; Woods et al.,
2002). Identification of the specific effects of unilateral or
bilateral STN DBS on cognitive–motor performance is
necessary to determine the best approach for individual
patients, in particular those patients with slight cognitive
dysfunction or advancing age.
A systematic comparison of unilateral to bilateral STN
DBS on motor and cognitive performance under dual-task
conditions has not been completed. We are aware of only
one published study that examined bilateral DBS on dualtask performance of two cognitive tasks (Witt et al., 2004).
Witt and colleagues (2004) reported that bilateral STN DBS
did not improve the performance of a dual cognitive task
(i.e. random number generation task paired with a card
sorting task). Motor function was not characterized under
dual-task conditions in their study, however, the authors
suggest that the effects of STN DBS on cognitive–motor
dual-task performance should be, ‘investigated in further
studies using motor and non-motor tasks simultaneously
with more concurrent attention demanding tasks’ (p. 700).
The primary aim of this study was to determine the effects
of unilateral and bilateral STN DBS on upper extremity
motor function and cognitive performance under varying
levels of cognitive–motor dual-task complexity. Based on
previous reports of impaired cognitive functioning following bilateral STN DBS, it was hypothesized that compared
with unilateral STN DBS bilateral STN DBS would result in
greater declines in cognitive and motor function when
moving from a single- to dual-task.
Page 3 of 13
Methods
Participants
Apparatus
A 6 df force-torque transducer (Mini-40 Model, ATI Industrial
Automation, Garner, NC, USA) was used to measure normal grip
force (Fz) during a force-tracking motor task. Grip force was
Table 1 Patient demographics and UPDRS Part III motor scores
Patient
Gender Age
(years)
DBS
Left stimulation
implant parameters
duration
(months)
Right stimulation
parameters
UPDRS total
Unilateral stimulation
Off/Uni/Bi-DBS Contralateral Ipsilateral
(%)
improvement improvement
(%)
(%)
1
M
2
M
3
F
4
M
5
F
6
F
7
M
8
M
Mean (SD)
70
16
45/31/26
(31/42)
59
12
2+/135 Hz/90 ms/2.0 V
2+/135 Hz/90 ks/2.2 V 52/34/24
(35/54)
48
14
3 + 2�/135 Hz/60 ks/3.2 V 3 + 2�/135 Hz/60 ms/2.8 V 56/39/32
(30/43)
49
12
2 � 3+/135 Hz/60 ms/3.2 V
2+/135 Hz/60 ks/2.8 V 63/42/36
(33/43)
56
13
2+/180 Hz/60 ms/3.2 V
2+/180 Hz/60 ks/2.8 V 62/41/37
(34/40)
59
22
2+/135 Hz/60 ks/3.5 V
2+/135 Hz/60 ms/3.0 V
59/35/26
(41/56)
54
14
2+/185 Hz/90 ks/2.5 V
2+/135 Hz/90 ms/2.5 V
56/41/31
(27/45)
57
12
2+/185 Hz/90 ks/3.1V
2+/135 Hz/90 ms/3.0 V
60/39/32
(35/47)
56.5 (6.8) 14.4 (3.4)
(33/46)
2+/185 Hz/60 ks/3.2 V
Bold parameters were used during unilateral stimulation.
2+/185 Hz/60 ms/3.0 V
58
21
55
19
47
15
50
20
51
16
52
22
48
17
43
21
50.5 (4.7)
18.9 (2.6)
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
A total of eight participants with advanced Parkinson’s disease
between the ages of 48 and 70 years (mean 56.5) years participated
in this study. Table 1 contains patient demographics, time since
DBS, stimulation parameters for the left and right stimulators and
clinical ratings for all patients. Bolded stimulation parameters in
Table 1 refer to parameters used during the unilateral stimulation
condition. All patients had undergone simultaneous bilateral STN
DBS at least 12 months prior to data collection. Surgical
procedures for DBS implantation have been reported in detail
previously (Starr et al., 1998a, b). The dorsal–ventral, anterior and
lateral borders of the STN were identified electrophysiologically
during DBS surgery. The DBS lead was placed such that contact
2 was at the dorsal border of the STN. Placement of electrodes was
verified using Cicerone visualization software described previously
(Miocinovic et al., 2007). Stimulation parameters for DBS devices
were clinically determined using the methods described by Moro
and colleagues (2006) and were stable for at least 6 months prior
to study participation. Because participants needed to make verbal
responses, patients with dysarthria or speech impairments were
excluded from the study. Each patient was compensated $100
for his/her time. Participants signed an informed consent
approved by the Georgia Institute of Technology and Cleveland
Clinic Institutional Review Boards prior to study enrolment.
Four patients were implanted at Emory University in Atlanta and
four patients were implanted at the Cleveland Clinic.
�Page 4 of 13
Brain (2008)
measured with a resolution of 0.06 N at a sampling rate of 256 Hz.
A customized LabView program was used to collect and display
the force data to the participant.
The n-Back task
Force-maintenance task
Participants used a precision grip (thumb and index finger only)
to exert an isometric force against the force transducer.
The transducer was oriented in a comfortable position relative
to the patient and then affixed to the table to prevent any
movement. Three maximum precision grip efforts, 5 s each, were
collected with the most affected hand as determined through
clinical evaluation and the patient’s self-report. For all patients,
the self-reported more affected limb was also rated as the more
affected side during the clinical examination. Participants were
given at least 2 min rest between maximum efforts. The greatest
force achieved from the three efforts was considered the maximum
and was used in calculating a 20% target force level. The 20%
target force level was selected as Galganski and colleagues (1993)
found no differences in younger adults’ and older adults’ SD at
this force level and based on our previous studies with younger
and older adults, this force level could be maintained relatively
easily with minimal fatigue (Voelcker-Rehage and Alberts, 2006,
2007). The target force level and actual grip force produced by
the most affected hand of the patient were displayed on a 21 in.
LCD monitor located �18–24 in. (44–59 cm) directly in front of
the participants. Participants were instructed to match their grip
force to the target force line as accurately as possible. An auditory
stimulus ‘ready, go’ signalled the participants to start matching
their force to the target force. Participants performed one to five
practice repetitions prior to test blocks to be certain all task
requirements were understood. Ten force-maintenance blocks for
each limb, 30 s each, were performed with at least 30 s of rest
between each block.
Dual task: n-back and force maintenance
simultaneously
Participants performed 15 dual-task blocks in which they were
asked to simultaneously perform the n-back task and forcemaintenance task. The force-maintenance task was performed in
random combination with each of the three n-back conditions
(0-, 1-, 2-back; five repetitions each). Participants were instructed
to perform both tasks as accurately as possible and to devote half
of their attention to the cognitive task and half of their attention
to the motor task. Participants were given at least 30 s of rest
between each block.
Procedure
All data were collected during two visits to the Neural Control
Laboratory at Georgia Tech or the Cleveland Clinic. Individual
patient experimental sessions were separated by not more than
7 days. All patients reported to the laboratory in the clinically
defined off phase in terms of anti-parkinsonian medication (e.g. at
least 12 h since last medication) and On DBS (both stimulators
On). After completing the informed consent process, patients were
evaluated clinically using the UPDRS Part III Motor Exam
administered by an experienced movement disorders neurologist.
The neurologist was blinded as to DBS status. The order of testing
for Day 1 during bilateral STN DBS was: (i) clinical evaluation;
(ii) force-maintenance task; (iii) n-back testing (three levels of
difficulty) and (iv) dual-task conditions with three levels of
difficulty. The order of the dual-task conditions (i.e. force
maintenance with 0-, 1- or 2-back) was randomized for each
patient. Upon completing the initial bilateral DBS testing session,
patients were randomized to either one or both of the DBS
systems to be turned Off. During unilateral DBS the stimulator
contralateral to the most affected side, determined clinically and
through patient self-report, remained On while the stimulator
ipsilateral to the most affected side was turned Off. Therefore, the
unilateral stimulation condition replicated the scenario in which
the patient would undergo if unilateral DBS were to be performed
i.e. the most affected side was treated (Slowinski et al., 2007).
After turning one or both stimulators Off, the patient rested in the
laboratory for 3 h to minimize any residual stimulation effects
(Temperli et al., 2003; Alberts et al., 2004). Following the 3 h rest
period clinical, cognitive and biomechanical testing were repeated.
Upon completion of this testing session the patient’s stimulator(s)
was/were turned On and patients took their anti-parkinsonian
medication. Total time spent in the laboratory was �5–6 h (testing
time �2 h and 3 h rest during the washout period). Following each
single- and dual-task condition, patients rated their level of mental
and physical fatigue on a scale of 1–10; 1 = no fatigue and
10 = exhausted.
Within 7 days of the initial experimental session patients
returned to the laboratory to complete the second data
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
A number of variations of the n-back task have been utilized in
previous studies (Owen et al., 2005). The n-back task utilized in
the current study was based on the methods originally used in its
development; this version requires the participant to repeat the
n-th item back (e.g. 0-, 1-, 2-back) in a sequentially presented list
of items (Dobbs and Rule, 1989). Task difficulty is manipulated by
requiring the participants to remember items further back in the
list. In the current study, the number of intervening letters varied
from zero to two. The letters were presented at a rate of one item
per �1.5 s. Using this method of n-back testing requires encoding,
maintenance, updating and output, however, is does not require
comparison or decision making like other versions of the task.
Two English-speaking experimenters conducted the n-back task.
Experimenter 1 read aloud the randomized letter sets of the
n-back task while experimenter 2 monitored the participant’s
responses for accuracy. Participants were asked to respond by
articulating the letter presented directly before (0-back), 1 cycle
before (1-back) or 2 cycles before (2-back). If the participant
made an error or failed to respond within �1.5 s, experimenter
2 said ‘start over’; and experimenter 1 began a new set of letters.
Approximately 19–23 trials (letters) were presented during a
30 s block. After performing the n-back task for 30 s participants
rested for 15–45 s and then repeated the n-back task under the
same level of difficulty (0, 1- or 2-back). Participants performed
five 30 s blocks at each n-back condition (0, 1- and 2-back). These
five blocks were collected sequentially and were randomized across
participants. To control for practice effects, all participants
completed three practice blocks (30 s each) at each n-back
difficulty level prior to data collection. All participants reported
task comprehension and demonstrated stable performance
between the second and third familiarization blocks. All practice
and test blocks consisted of a unique list of randomized letters to
prevent any memorization of letters.
J. L. Alberts et al.
�Bilateral DBS impairs dual-task performance
Data analysis
Force tracking
All force data were filtered with a phase-symmetric low-pass filter
using Woltring’s algorithm (detailed in previous studies, VoelckerRehage et al., 2006; Voelcker-Rehage and Alberts, 2007) using
existing Matlab analysis programs developed in our laboratory.
Force data were assessed for accuracy from 3 s after the start of the
block until completion of the block; this period allowed the
patient sufficient time to achieve the target force. The primary
motor outcome variables for the force-tracking task were time
within the target range (TWR) and relative root mean square
error (RRMSE). The TWR is calculated by determining the time
the patient’s force trace is within �2.5% of the target line. The
TWR provides an overall accuracy measure of force tracking. To
account for differences in the amplitude of the target force
(e.g. inter- and intra-patient variability due to stimulation status),
the RRMSE, as defined in equation (1), was used as a method of
normalizing performance relative to force amplitude. The RRMSE
is considered to reflect the overall variability of force-tracking
performance; a lower RRMSE suggests control of distal musculature and hand functionality (Kriz et al., 1995; Kurillo et al.,
2004). In equation (1), FT(t) is the target force provided to the
patient, F0(t) is the force produced by the patient and T is the
time of the block.
vffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi
u T
u 1 X ðF0 ðt Þ � FT ðt ÞÞ2
RRMSE ¼ t
ð1Þ
T t¼0
maxðFT Þ2
The n-Back performance
The n-back performance was measured by determining the
percentage of correct letters recalled during a 30 s block and the
total number of errors (NE) committed during a block (VoelckerRehage et al., 2006).
Dual-task analysis
To examine participants’ performance under the dual-task
conditions, the dual-task loss (DTL) was computed using a
standard measure to compare performance on single- and dualtask conditions (Lindenberger et al., 2000). The DTLs were
computed as the percentage of loss in motor and cognitive
Page 5 of 13
performance during dual-task conditions relative to performance
in the single-task conditions in the following manner:
DTLforce = [(mean dual taskforce – mean baselineforce)/mean
baselineforce] � 100.
DTLn-back = [(mean dual taskn-back – mean baselinen-back)/mean
baselinen-back] � 100.
Statistical analysis
Motor (RRMSE, TWR) and cognitive [percentage of correctly
repeated letters (PRL), NE] performance data were analysed with
repeated measures ANOVAs. Greenhouse Geyser adjustment was
reported when the sphericity assumption was violated. Post hoc
contrasts (Bonferroni adjustment) were used to determine
differences between the DBS status and level of task difficulty to
determine the conditions that were most affected by the different
states of DBS. Analyses were conducted separately for the motor
and cognitive task.
Two 3 (stimulation: Off DBS, unilateral DBS, bilateral DBS) � 3
(task difficulty: 0-, 1-, 2-back) � 2 (context: single task, dual task)
repeated measure ANOVAs were used to determine differences
between different states of DBS in n-back difficulty and between
single- and dual-task context using PRL and NE. Additionally, two
3 (stimulation) � 4 (task difficulty: force only, force at 0-, 1- and
2-back difficulty) repeated measure ANOVAs were carried out
using the RRMSE and TWR scores.
To examine whether DTLs for the force task and the n-back
difficulties were significantly different from zero, a series of onesample t-tests (test value = 0) were conducted separately for each
DBS condition. Repeated measures ANOVAS with corresponding
post hoc tests were used to compare the DTLs for task difficulties
(0-, 1-, 2-back) and DBS status.
Results
Clinical ratings
Table 1 contains total and symptom related UPDRS motor
scores for each patient during Off, unilateral and bilateral
DBS. While there was a tendency for patients to rate their
level of cognitive and motor fatigue levels slightly higher
(i.e. more fatigue) as the testing session progressed, no
statistically significant differences were present between
stimulation conditions. In terms of clinical motor function,
the UPDRS-III scores decreased significantly as a result of
unilateral and bilateral DBS. Unilateral DBS resulted in a
33% improvement in clinical rating while bilateral DBS
improved ratings by 46% compared with Off DBS.
Statistical analysis (t-tests for paired samples) revealed
that the additional 13% improvement in UPDRS motor
score with bilateral DBS was statistically better than unilateral DBS [t(7) = 9.11, P50.01]. Both bilateral and unilateral were significantly better than Off DBS [tbi-off(7) =
18.40, P50.01; tuni-off(7) = 15.52, P50.01].
Cognitive functioning and DBS during
single- and dual-task conditions
Percentage of correct letters
The results from the repeated measures ANOVA (cf. Fig. 1)
revealed that overall n-back performance decreased with
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
collection session. Identical to the initial visit, patients
arrived Off anti-parkinsonian medication and On bilateral
stimulation. To account for potential practice effects on the
second day of testing, the patients repeated the bilateral On DBStesting protocol that was performed on Day 1 (e.g. clinical
evaluation, n-back testing, force-maintenance testing and dualtask conditions). Statistical analysis of bilateral On DBS
indicated that cognitive and motor performance did not differ
from Day 1 and Day 2 experimental sessions. Therefore, cognitive
and motor performance was stable across experimental
sessions. Because performance was stable across the experimental
sessions data were collapsed across days for the bilateral On
DBS condition. On Day 1, the order of testing for four patients
was: bilateral DBS followed by unilateral DBS, Day 2 order
of testing was bilateral DBS followed by Off DBS. For the
remaining four patients, after bilateral STN DBS, the order was
reversed.
Brain (2008)
�Page 6 of 13
Brain (2008)
J. L. Alberts et al.
Percentage of correct repeated letters
A
B
single-task
dual-task
105
105
100
100
95
95
90
90
85
*
**
85
1-back
2-back
off DBS
uni DBS
bi DBS
0-back
1-back
2-back
Fig. 1 (A) Results of the n-back task in the single-task condition at Off DBS, unilateral DBS and bilateral DBS (means and standard errors).
(B) Results of the n-back task in the dual-task condition at Off DBS, unilateral DBS and bilateral DBS (means and standard errors). A cross
marks a significant differences between Off and unilateral DBS, an asterisk marks a significant difference between Off and bilateral DBS,
and a double asterisk marks a significant difference between unilateral and bilateral DBS.
increasing task difficulty [F(1.12,7.85) = 192.97, P50.01,
Z2 = 0.96]. The main effect of DBS status was significant
[F(2,14) = 18.52, P50.01, Z2 = 0.73]. Post hoc contrasts
revealed a significantly lower n-back performance
for bilateral DBS as compared with Off and unilateral
DBS (always P50.01). Importantly, also the task difficulty � stimulation interaction was significant [F(4,14) = 13.96,
P = 0.01, Z2 = 0.67], resulting from a greater performance
decrease with increasing n-back difficulty for bilateral DBS
than for the Off and unilateral DBS. In addition, 2-back
performance at bilateral DBS was significantly lower than
performance at unilateral DBS in single- and dual-task
context. Thus, in the most complex condition (2-back at
dual task) bilateral DBS led to significantly lower performances compared with unilateral DBS or the Off state
(cf. Fig. 1).
Number of errors
Errors in cognitive function were primarily due to
responding with the incorrect letter and the participant
reporting to experimenter 1 that they did not remember the
letter to be recalled. Less than 0.5% of the errors were the
result of the patient not responding within the �1.5 s time
period. Bilateral DBS led to a higher amount of errors
as compared with Off DBS (for the 1- and 2-back task) and
as compared with unilateral DBS (2-back only) in the
single-task context. For the NE the effect of task difficulty
[F(2,14) = 178.18, P50.01, Z2 = 0.96] and stimulation
[F(1.06,7.43) = 11.95, P50.01, Z2 = 0.63] was significant,
whereas the context effect [F(1,14) = 1.70, P = 0.23] was not.
Participants produced more errors as the difficulty of the
n-back task increased, but not as the context changed from
single- to dual-task. The NE, however, significantly differed
between the DBS states. Bilateral DBS resulted in the
greatest amount of errors (P = 0.01).
Motor function and DBS during single- and
dual-task conditions
Relative root mean square error
Variability in force tracking increased significantly as task
difficulty increased [F(3,42) = 30.94, P50.01, Z2 = 0.82].
Additionally, the force variability differed between the three
DBS conditions [F(2,42) = 44.62, P50.01, Z2 = 0.86], with
unilateral DBS showing the highest force-tracking performance and with Off DBS showing the lowest performance
(always P50.03). The deterioration in force-maintenance
performance across the task difficulties, however, was
different between the DBS states [F(6,42) = 3.54, P = 0.01,
Z2 = 0.34] (cf. Fig. 2A). As shown in Fig. 2A bilateral DBS
revealed a tremendous performance decrease across the task
conditions. Whereas in the force only condition bilateral
DBS showed performance levels comparable with unilateral
DBS [Off DBS was significantly worse than unilateral and
bilateral DBS (P50.01)], in the 2-back condition bilateral
DBS performance level was comparable with the Off DBS
state and significantly worse than unilateral DBS (P50.05)
(cf. Fig. 2A).
Time within target range
Results from the TWR confirmed results of RRMS. During
the Off DBS condition, performance was essentially the
same across all task condition (e.g. fairly low accuracy for
all conditions), performance during bilateral stimulation
decreased dramatically across all task difficulties and was
similar to performance levels of Off DBS during the most
difficult condition, 2-back.
DTLs different from zero
Bilateral stimulation resulted in a significant decline in
cognitive function when moving from single- to dual-task
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
0-back
80
*
**
�Bilateral DBS impairs dual-task performance
A
6
single-task
Brain (2008)
dual-task
B
30
single-task
Page 7 of 13
dual-task
5
RRMSE
TWR (sec.)
25
4
**
+
3
2
*
+
0
force
0-back
force
1-back
**
+
10
force
2-back
fore
only
force
0-back
force
1-back
force
2-back
Fig. 2 (A) Results of the RRMSE force in the single- and dual-task conditions at Off DBS, unilateral DBS and bilateral DBS (means
and standard errors). (B) Results of the TWR force in the single- and dual-task conditions at Off DBS, unilateral DBS and bilateral
DBS (means and standard errors). A plus marks a significant differences between Off and unilateral DBS, an asterisk marks a significant
difference between Off and bilateral DBS and a double asterisk marks a significant difference between unilateral and bilateral DBS.
A
B
DTLs n-back
20
550
500
450
* *
* *
DTL
*
−5
−15
*
*
−20
250
*
*
*
150
*
*
*
2-back
*
−35
50
−40
off DBS
uni DBS
bi DBS
1-back
2-back
*
*
*
−45
0-back
*
*
−30
100
0
−20
*
−25
200
1-back
*
−10
*
300
0
0-back
DTLs TWR
0
* *
400
350
off DBS
uni DBS
bi DBS
C
DTLs RRMSE
off DBS
uni DBS
bi DBS
0-back
1-back
*
2-back
Fig. 3 DTLs and standard errors for (A) the n-back task, (B) the force-maintenance task (RRMSE) and (C) the force maintenance task
(TWR) task at Off DBS, unilateral DBS and bilateral DBS. An asterisk marks DTLs significantly greater than zero and significant differences
between the states of stimulation (�P50.05). Positive DTLs for force TWR and n-back indicate gains in dual-task performance, negative
DTLs for force TWR and n-back indicate DTLs. Positive values for force RRMSE indicate DTLs, negative values indicate dual-task gains.
conditions, while no change in cognitive performance was
present for Off or unilateral DBS during this same
transition from single- to dual-task conditions. Results
from the one-sample t-tests indicated that Parkinson’s
disease patients showed no significant DTLs for n-back task
performance during Off DBS [t0-back(7) = 1.53, P = 0.17;
t1-back(7) = 0.19, P = 0.86; t2-back(7) = �1.04, P = 0.33] or
P = 0.06;
with
unilateral
DBS
[t0-back(7) = �2.27,
t1-back(7) = 1.66, P = 0.14; t2-back(7) = 1.46, P = 0.19], however, during bilateral DBS [t0-back(7) = �2.55, P = 0.04;
t1-back(7) = �4.99, P50.01; t2-back(7) = �2.73, P = 0.03]
significant cognitive DTLs were present (cf. Fig. 3A); the
DTLs were not different between the 1- and 2-back
conditions [t(7) = �1.56, P = 0.16].
As expected, force-tracking performance did decline as
task complexity increased from single- to dual-task
conditions while Off DBS and with unilateral and bilateral
stimulation conditions. However, the greatest declines in
motor performance were associated with bilateral DBS.
The DTLs in force-tracking performance (RRMSE) at Off
DBS were significant for the 2-back condition [t0-back(7) =
1.29, P = 0.24; t1-back(7) = 2.17, P = 0.17; t2-back(7) = 2.89,
P = 0.02]. Results under unilateral and bilateral DBS
revealed significant DTLs in force-maintenance performance for all three n-back difficulties [unilateral DBS:
t0-back(7) = 3.30, P = 0.01; t1-back(7) = �4.42, P50.01;
t2-back(7) = 5.01, P50.01; bilateral DBS: t0-back(7) = 3.54,
P = 0.01;
t1-back(7) = 3.33,
P = 0.01;
t2-back(7) = 7.42,
P50.01] (cf. Fig. 3B). Also for TWR, the greatest performance decrements occurred during the 2-back dualtask condition and the smallest with the 0-back difficulty
(cf. Fig. 3C).
Task difficulty and stimulation differences in DTLs
DTLsn-back, did not significantly change with increasing task
difficulty [F(2,14) = 0.50, P = 0.58], but with the type of
stimulation [F(2,14) = 17.47, P50.01, Z2 = 0.71]. DTLs were
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
fore
only
*
+
15
off DBS
uni DBS
bi DBS
1
20
�Page 8 of 13
Brain (2008)
Discussion
The aim of this study was to determine the effects of
unilateral and bilateral STN DBS on cognitive and motor
function under dual-task conditions. The use of a dual-task
paradigm with varying levels of cognitive difficulty better
replicates the performance of activities of daily living
(ADLs), which typically consist of cognitive and motor
components performed concurrently. Under relatively
simple dual-task conditions there were no differences in
cognitive or motor performance between unilateral and
bilateral stimulation. However, as dual-task complexity
increased, cognitive and motor performance was significantly worse with bilateral compared with unilateral
stimulation. In fact, in the most complex dual-task
condition (i.e. 2-back + force maintenance), bilateral
stimulation resulted in a level of motor performance that
was similar to no stimulation at all. This pattern of
results was present in all eight patients studied. Overall,
these data suggest that under modestly complex cognitive–
motor task conditions, unilateral DBS was associated
with better cognitive and motor performance than bilateral
DBS.
DBS and working memory during
single-task conditions
Bilateral STN DBS led to a significant decline in working
memory under the most difficult n-back condition
compared with unilateral and Off DBS conditions. These
data are consistent with a previous study indicating that
bilateral STN DBS results in decreased memory performance when memory load demands were highest (Hershey
et al., 2004). At first glance, the current data are in conflict
with two studies that have shown STN stimulation
improves working memory (Pillon et al., 2000; RivaudPechoux et al., 2000). However, an important difference
between the studies showing a decline in working
memory and those showing improvements is the level of
task difficulty. Impairments in working memory during
the most demanding n-back condition (2-back) provides
support for the hypothesis that bilateral STN DBS
interferes with patients’ ability to handle higher demands
placed on cognitive control processes (Hershey et al., 2004).
The fact that unilateral STN DBS did not lead to the
same level of decline in working memory may indicate
that the non-stimulated basal ganglia may be able to
compensate for the disruption of activity caused by
stimulation. Alternatively, disruption from activation of
an adjacent white matter tract may not be enough to
disrupt function during unilateral stimulation. Based on
recent data suggesting that DBS contralateral to the
more affected side of the body may result in greater
impairments in spatial working memory compared with
stimulation contralateral to the less affected side (Hershey
et al., 2007), additional studies are necessary to determine if
the same pattern of results occurs under dual-task
conditions.
DBS and motor function during
single-task conditions
Unilateral and bilateral DBS resulted in a significant
improvement in clinical ratings and in force-maintenance
performance compared with Off DBS. The mean improvement in UPDRS Part III motor scores was 33% and 46%
for unilateral and bilateral DBS, respectively. This level of
improvement in clinical ratings associated with unilateral
STN DBS is consistent with our earlier findings (Alberts
et al., 2004) and more recent data (Chung et al., 2006;
Slowinski et al., 2007). The contralateral improvement
(51%) in motor symptoms was greater than the ipsilateral
(19%) improvement under unilateral stimulation. The
degree of improvement in ipsilateral clinical ratings is
within the range recently reported (Chung et al., 2006;
Slowinski et al., 2007). Force-maintenance performance was
significantly improved during unilateral and bilateral
stimulation compared with Off DBS. Few data are available
in which unilateral and bilateral DBS have been compared
in terms of upper extremity function (Bastian et al., 2003).
During fast reaching movements Bastian and colleagues
(2003) found there was no additive effect of bilateral STN
DBS compared with unilateral. The current data are
consistent with these findings as force-tracking performance
for the most affected limb was similar under unilateral and
bilateral stimulation. The lack of an additive effect of
bilateral stimulation on discrete unimanual upper extremity
task performance suggests that contralateral basal ganglia
thalamocortical pathways are largely responsible for mediating contralateral upper extremity motor performance or
whatever ipsilateral pathway is required to obtain maximal
benefit is also fully activated during contralateral
stimulation.
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
significantly higher with bilateral DBS as compared with Off
and unilateral DBS (P50.03). The task difficulty � stimulation interaction was also significant [F(4,28) = 7.14, P50.01,
Z2 = 0.51] (cf. Fig. 3A).
DTLsforce (RRMSE) displayed a significant main effect of
task difficulty [F(2,14) = 26.10, P50.01, Z2 = 0.79], DTLs in
force-maintenance performance were smallest for the
0-back condition, and highest for the 2-back condition, a
significant main effect of stimulation [F(1.17,8.22) = 12.14,
P50.01, Z2 = 0.63], and a significant task difficulty � stimulation interaction [F(4,28) = 8.71, P50.01,
Z2 = 0.55]. Differences between DBS states were significant
in the 1-back condition (significantly lower DTLs while Off
DBS than unilateral DBS; P = 0.02) and the 2-back
condition (always P50.05), with highest DTLs at bilateral
DBS. Results of the TWR confirmed results of RRMSE
(cf. Fig. 3B and C).
J. L. Alberts et al.
�Bilateral DBS impairs dual-task performance
DBS and dual-task performance
Page 9 of 13
follow-up questions regarding attention allocation across
the two tasks). The n-back is known to place demands on
executive processes as information must be processed,
requires online monitoring and manipulation of remembered information; therefore, it is assumed to place great
demands on key processes within working memory
(McElree, 2001; Blokland et al., 2008). Previous imaging
studies have shown that the frontal cortex, in particular, the
dorsolateral prefrontal cortex is activated during a working
memory task such as the n-back task (Jansma et al., 2000;
Owen et al., 2005). Disruption of information processing in
the non-motor regions of STN and adjacent areas that
project to the frontal cortex may be responsible for the
varying levels of decline reported in cognitive functioning
during STN DBS.
Recent data collected using a rat model of Parkinson’s
disease, indicate that bilateral stimulation of the STN leads
to an inhibition of 5-hydroxytrptamine neurons, which
resulted in depression related behavioural changes (Temel
et al., 2007). Given its small size, stimulation within the
STN, even with leads located within the sensorimotor
territory, can result in spread of current to limbic and
associative areas as well as to surrounding structures and
fibre systems that may also affect cognition. Until recently,
the pattern of current spread and its effects on neuronal
activity on target nuclei associated with STN DBS was not
well characterized. Theoretical (McIntyre et al., 2004a, b)
and experimental data (Hashimoto et al., 2003), however,
suggest that the therapeutic mechanisms of DBS may work
by activating axons surrounding the electrode. This axonal
activation is non-discriminately applied to fibres leaving,
passing through or adjacent to the stimulated nucleus.
Activation of these fibre systems is proposed to produce a
regularization of neural activity patterns in the pallidum
during STN DBS (Montgomery and Baker, 2000; Vitek,
2002b; Hashimoto et al., 2003; Grill et al., 2004; Rubin and
Terman, 2004). These stimulation effects are subsequently
transmitted throughout the basal ganglia and thalamocortical networks, modulating neural activity throughout the
brain (Fukuda et al., 2001; Hershey et al., 2003; Phillips
et al., 2006). Recently, finite element modelling of tissue
and DBS current was used to determine the volume of
tissue activated (VTA) during therapeutic and nontherapeutic stimulation parameters with STN DBS
(Butson et al., 2007). With therapeutically effective DBS
parameters, a significant portion of the VTA with
stimulation was outside the STN and spread to the zona
incerta and Fields of Forel. This article did not further parse
the STN into motor and non-motor regions and calculate
that amount of VTA within each region so it is unknown
what segments of STN were being stimulated. These data
do, however, support the hypothesis that non-motor
pathways are likely activated during STN DBS and may
contribute to the present observations.
The transmission of pathological information within the
basal ganglia thalamocortical circuits is hypothesized to
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
In general, cognitive and motor performance declined as
task complexity increased across stimulation conditions.
These results were expected as previous studies indicate that
even in healthy older adults declines in cognitive and motor
function occur when moving from single- to dual-task
conditions (Chen et al., 1996; Lindenberger et al., 2000;
Morris et al., 2000; Marchese et al., 2003; Rochester et al.,
2004; Voelcker-Rehage et al., 2006). The overall performance decrements during bilateral DBS with increasing
dual-task difficulty are comparable to the pattern of
performance decrements observed in older adults.
Voelcker-Rehage et al. (2006) showed in a study with
older adults that motor and cognitive performance decrease
with increasing task difficulty under dual-task conditions.
However, the relative loss in cognitive and motor
performance when moving from single- to dual-task
conditions was greater during bilateral DBS than the DTL
older adults experienced. It should be noted that only one
of the patients in the current study would be considered an
‘older adult’; seven of eight patients were under 60 years of
age and yet their loss in cognitive functioning with bilateral
STN DBS was greater under dual-task conditions. Also,
healthy young adults exhibit no decrease in cognitive or
motor performance during dual-task conditions, neither in
the cognitive or motor domain.
Motor performance did not change dramatically under
dual-task conditions while Off DBS, until the most difficult
condition. Relatively stable motor performance while Off
DBS is likely a reflection of a floor effect as patients’
performance was relatively poor under single-task conditions and there was little room for further decline. Motor
performance during dual-task conditions was significantly
worse compared with single-task conditions under both
unilateral and bilateral DBS. The overall accuracy of force
tracking (TWR) declined while the variability of force
output (RRMSE) increased as task complexity increased.
During the 0-back dual-task condition only a slight decline
in motor performance was displayed by patients. However,
as the cognitive demands increased, the difference between
unilateral and bilateral stimulation on motor performance
became apparent. During the 1-back dual-task condition,
motor performance under bilateral stimulation was only
slightly better than no stimulation. During the most
difficult condition, 2-back dual task, overall motor
performance, TWR and RRMSE, was significantly worse
than unilateral DBS. In fact, during the 2-back dual-task
condition with bilateral stimulation motor performance was
nearly identical to performance levels while Off stimulation.
A decline in motor performance with bilateral DBS under
dual-task conditions, in particular during the 2-back
condition, may have been an imbalance in the level of
attention allocated for the performance of the cognitive task
(e.g. greater emphasis placed on n-back compared with
force task despite experimental instructions and response to
Brain (2008)
�Page 10 of 13
Brain (2008)
Importance of cognitive^motor assessment
At first glance, the current data indicating a decline in
cognitive–motor performance associated with bilateral STN
DBS under dual-task conditions appears paradoxical in
light of reported improvements from other studies in
clinical measures of quality of life and performance of ADLs
following STN DBS. It is acknowledged that the vast
majority of studies indicate bilateral STN DBS results in
significant improvements in the patient’s perception of
their quality of life (Drapier et al., 2005; Erola et al., 2005;
Lyons and Pahwa, 2005; Fraix et al., 2006; Gronchi-Perrin
et al., 2006; Kleiner-Fisman et al., 2006; Siderowf et al.,
2006; Martinez-Martin and Deuschl, 2007). However, an
analysis of the change in individual subscales of the
PDQ-39 indicated that only physical aspects of quality of
life improved significantly following bilateral STN DBS
(Drapier et al., 2005), while the subscales characterizing
emotional well-being, social support and cognition
improved slightly (but not significantly) and communication actually worsened after bilateral STN DBS. Although
the PDQ-39 has been validated (Peto et al., 1995), it has
been shown to be susceptible to placebo effects, especially
in the context of a surgical intervention (McRae et al.,
2004). More recently, preliminary data suggest patients’
perceptions of their day-to-day function to be improved
subtly, however, caregivers perceived the patients’ as
exhibiting subtle declines in day-to-day functioning (DuffCanning et al., 2008). Collectively, these studies indicate
that the PDQ-39 is limited and may not adequately capture
patients’ quality of life following DBS.
Despite the overall excellent motor and quality of life
improvements using clinical measures, there is a contrast
between the improvement in motor disability and the
difficulties experienced by patients as they try to reintegrate
into a more normal life (Agid et al., 2006). Schupbach and
colleagues (2006) recently examined a group of relatively
young Parkinson’s disease patients, average age = 52,
following bilateral STN DBS. Clinical measures of
motor function and quality of life improved significantly,
however, patients experienced difficulties in psychosocial
function, personal relationships and functioning in a socioprofessional environment. A striking finding from their
study was the relatively large percentage of patients who did
not return back to work following DBS. Of the 29 patients
studied, 16 were working prior to DBS. However, after DBS
surgery, in spite of improvements on clinical measures of
motor function and quality of life, 7 of those 16 patients
(44%) did not return to work following DBS. It was noted
that after surgery, ‘patients experienced slight and subtle
intellectual symptoms that became apparent in the course
of repeated and thorough unstructured interviews’,
(p. 1814) (Schupbach et al., 2006). For those not returning
to the workplace, they reported, ‘I don’t have the same
ability to concentrate as before’, and they had difficulty
‘ordering complex actions and thoughts, anticipating and
planning ahead’ and ‘limited attention, and working
memory’ and were ‘easily distracted’ (Schupbach et al.,
2006). These features of cognitive function are not assessed
in the self-report measures of the PDQ-39. Rather, the
PDQ-39, for the most part, asks patients to rate their
performance on a discrete motor task over the past month,
the context in which this task is performed is, in general,
not taken into consideration during the administration of
this exam. We propose that these conditions do not
adequately reflect the context in which most ADLs are
performed (i.e. concurrent performance of a cognitive and
motor task). Better replicating the context in which ADLs
are performed during the programming and adjustment of
stimulation parameters is necessary to further improve
cognitive and motor outcomes of those patients currently
undergoing DBS surgery. This may be particularly relevant
in the near future if it is demonstrated that DBS is capable
of altering the course of Parkinson’s disease (Schupbach
et al., 2007; Wallace et al., 2007). An earlier application of
DBS would likely result in a younger group of patients
being implanted; patients who are still active in the
workforce. For these patients in particular, the detection
and prevention of subtle cognitive and cognitive–motor
declines during DBS programming may allow them to
maintain their level of performance and remain in the
workforce longer. Thereby, maintaining their quality of life
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
underlie the symptoms of Parkinson’s disease (Albin et al.,
1989; DeLong, 1990; Llinas et al., 1999; Vitek and Giroux,
2000; Timmermann et al., 2003). Analysis of globus pallidus
internus (GPi) neuronal activity during STN DBS in
parkinsonian primates has led to the hypothesis that DBS
masks this intrinsic activity by replacing the pathological
activity associated with Parkinson’s disease with a more
regular pattern of activity in the GPi. This regularized
activity is then transmitted throughout the motor circuit
producing an ‘informational lesion’ and prevents the
passage of pathological information from the pallidum
(Hashimoto et al., 2003; Grill et al., 2004). While DBS may
prevent the transmission of pathological information within
the motor circuit, current spread to non-motor regions of
STN is likely to create the same type of informational
lesion, thus disrupting potentially non-pathological information processing. Such a ‘lesion’ may not produce a
detectable deficit in cognitive function following unilateral
procedures or even with bilateral DBS when the patients are
able to focus their attention on the performance of a
cognitive or motor task; as it is the case during most
clinical examinations. However, as the cognitive demands
of the task increase and information-processing demands
increase, function of redundant non-motor circuits may be
compromised and during bilateral stimulation the redundancy of non-motor circuits may be decreased. Thus,
patients are unable to draw on cognitive resources as they
are now compromised as a result of bilateral disruption of
non-motor circuits.
J. L. Alberts et al.
�Bilateral DBS impairs dual-task performance
Page 11 of 13
DBS current to non-motor regions of STN or alteration
of neuronal activity patterns from the sensorimotor portion
of the STN could be responsible for emerging cognitive side
effects, especially under bilateral DBS or during the
performance of motor tasks under complex conditions.
Current methods of assessing cognitive and motor function
in a clinical environment may not be sufficiently demanding to reveal changes in cognitive performance that occur
under dual-task conditions and can result in diminished
motor function. We are currently investigating the effectiveness of using an abridged version of dual-task paradigm
in the selection of DBS parameters in a clinical setting.
Funding
National Institute
NS037959).
of
Health
(R03
AG022178
and
References
Agid Y, Schupbach M, Gargiulo M, Mallet L, Houeto JL, Behar C, et al.
Neurosurgery in Parkinson’s disease: the doctor is happy, the patient
less so? J Neural Transm Suppl 2006; 70: 409–14.
Alberts JL, Elder CM, Okun MS, Vitek JL. Comparison of pallidal and
subthalamic stimulation on force control in patient’s with Parkinson’s
disease. Motor Control 2004; 8: 484–99.
Alberts JL, Okun MS, Vitek JL. The persistent effects of unilateral pallidal
and subthalamic deep brain stimulation on force control in advanced
Parkinson’s patients. Parkinsonism Relat Disord 2008; 14: 481–8.
Albin RL, Young AB, Penney JB. The functional anatomy of basal ganglia
disorders. Trends Neurosci 1989; 12: 366–75.
Bastian AJ, Kelly VE, Revilla FJ, Perlmutter JS, Mink JW. Different effects
of unilateral versus bilateral subthalamic nucleus stimulation on walking
and reaching in Parkinson’s disease. Mov Disord 2003; 18: 1000–7.
Benabid AL, Krack PP, Benazzouz A, Limousin P, Koudsie A, Pollak P.
Deep brain stimulation of the subthalamic nucleus for Parkinson’s
disease: methodologic aspects and clinical criteria. Neurology 2000; 55:
S40–4.
Blokland GA, McMahon KL, Hoffman J, Zhu G, Meredith M, Martin NG,
et al. Quantifying the heritability of task-related brain activation and
performance during the N-back working memory task: a twin fMRI
study. Biol Psychol 2008; 79: 70–9.
Butson CR, Cooper SE, Henderson JM, McIntyre CC. Patient-specific
analysis of the volume of tissue activated during deep brain stimulation.
Neuroimage 2007; 34: 661–70.
Chen H-C, Schultz AB, Ashton-Miller JA, Giordani B, Alexander NB,
Guire KE. Stepping over obstacles: dividing attention impairs performance of old more than young adults. J Gerontol 1996; 51A: M116–22.
Chung SJ, Jeon SR, Kim SR, Lee MC. Bilateral effects of unilateral
subthalamic nucleus deep brain stimulation in advanced parkinson’s
disease. Eur Neurol 2006; 56: 127–32.
DeLong MR. Primate models of movement disorders of basal ganglia
origin. Trends Neurosci 1990; 13: 281–5.
Dobbs AR, Rule BG. Adult age differences in working memory. Psychol
Aging 1989; 4: 500–3.
Drapier S, Raoul S, Drapier D, Leray E, Lallement F, Rivier I, et al. Only
physical aspects of quality of life are significantly improved by bilateral
subthalamic stimulation in Parkinson’s disease. J Neurol 2005; 252:
583–8.
Duff-Canning SJ, Poon YY, Chang T, Mailis N, Lozano AM, Hodaie M,
et al. He said, she said: differences between self and caregiver ratings
of postoperative behavioral changes in Parkinson’s disease patients
undergoing bilateral subthalamic nucleus deep brain stimulation.
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
and decreasing non-treatment related costs (i.e. lost worker
productivity) associated with Parkinson’s disease and DBS
for Parkinson’s disease.
One limitation of this study is that we only tested
patients who had undergone STN DBS. Though the STN is
the most commonly targeted site for treatment of advanced
Parkinson’s disease, we do not know if these same effects
are present with bilateral GPi DBS. Fewer reports of
cognitive dysfunction have been reported with GPi DBS,
however, this may be a function of the relatively smaller
number of GPi cases rather than the effect of stimulation
site (Vitek, 2002a). The patients’ level of attention to the
cognitive and motor task under dual-task conditions may
also have influenced the results. While they were instructed
to focus attention on both tasks equally, it is possible they
attended more to the cognitive or motor task. When asked
about the focusing of attention after the experiment, all
patients responded that they tried to weigh each task
equally. Learning and fatigue certainly impact cognitive and
motor performance. However, we were careful to provide
adequate rest breaks between blocks, thus minimizing the
effects of fatigue. Furthermore, fatigue is not likely to have
affected patients’ performance during bilateral DBS conditions as they were always tested in this condition before the
unilateral or Off DBS conditions. The lingering effects of
medication on cognitive and motor performance between
the stimulation conditions are unknown, since patients
were first tested while On bilateral DBS. However, these
potential beneficial effects would be expected to lead to a
greater retention of motor benefits during bilateral DBS,
thus potentially decreasing the effects of the dual-task on
cognitive and motor performance. This was not the case as
cognitive–motor performance was, in general, better during
unilateral compared with bilateral STN DBS, even though
the patients were off medication longer during the
unilateral DBS condition. In terms of learning effects, in
general the n-back task is not subject to learning effects
once the task requirements have been comprehended by the
patient. Nevertheless, practice blocks were given at each
level of task difficulty and all the patients reported
understanding task requirements. In terms of motor
learning impacting performance on the force-maintenance
task, the task is relatively simple as the patient produces a
constant force and is provided real-time feedback regarding
their performance thus patients can learn the task relatively
quickly. If motor learning or task experience were to impact
force-maintenance performance, data collected later in the
day under unilateral DBS would be expected to be better
than with bilateral DBS. This was not the case as
performance during force maintenance only blocks was
similar during unilateral and bilateral DBS.
The fundamental goal of DBS is to alter pathological
neural activity within the basal ganglia to provide
maximum motor response with minimal side effects. The
alteration of pathological motor information leads to
improvements in motor function. However, the spread of
Brain (2008)
�Page 12 of 13
Brain (2008)
Marchese R, Bove M, Abbruzzese G. Effect of cognitive and motor tasks on
postural stability in Parkinson’s disease: a posturographic study. Mov
Disord 2003; 18: 652–8.
Martinez-Martin P, Deuschl G. Effect of medical and surgical interventions
on health-related quality of life in Parkinson’s disease. Mov Disord
2007; 22: 757–65.
McElree B. Working memory and focal attention. J Exp Psychol Learn
Mem Cogn 2001; 27: 817–35.
McIntyre CC, Grill WM, Sherman DL, Thakor NV. Cellular effects of deep
brain stimulation: model-based analysis of activation and inhibition.
J Neurophysiol 2004a; 91: 1457–69.
McIntyre CC, Mori S, Sherman DL, Thakor NV, Vitek JL. Electric field
and stimulating influence generated by deep brain stimulation of the
subthalamic nucleus. Clin Neurophysiol 2004b; 115: 589–95.
McRae C, Cherin E, Yamazaki TG, Diem G, Vo AH, Russell D, et al.
Effects of perceived treatment on quality of life and medical outcomes
in a double-blind placebo surgery trial. Arch Gen Psychiatry 2004; 61:
412–20.
Miocinovic S, Noecker AM, Maks CB, Butson CR, McIntyre CC. Cicerone:
stereotactic neurophysiological recording and deep brain stimulation
electrode placement software system. Acta Neurochir Suppl 2007; 97:
561–7.
Montgomery EB Jr, Baker KB. Mechanisms of deep brain stimulation and
future technical developments. Neurol Res 2000; 22: 259–66.
Moro E, Poon YY, Lozano AM, Saint-Cyr JA, Lang AE. Subthalamic
nucleus stimulation: improvements in outcome with reprogramming.
Arch Neurol 2006; 63: 1266–72.
Morris M, Iansek R, Smithson F, Huxham F. Postural instability in
Parkinson’s disease: a comparison with and without a concurrent task.
Gait Posture 2000; 12: 205–16.
Morrison CE, Borod JC, Brin MF, Raskin S, Germano I, Weisz D, et al. A
program for neuropsychological investigation of deep brain stimulation
(PNIDBS) in movement disorder patients: development, feasibility, and
preliminary data. Neuropsychiatry Neuropsychol Behav Neurol 2000; 13:
204–19.
Owen AM, McMillan KM, Laird AR, Bullmore E. N-back working
memory paradigm: a meta-analysis of normative functional neuroimaging studies. Hum Brain Mapp 2005; 25: 46–59.
Parsons TD, Rogers SA, Braaten AJ, Woods SP, Troster AI. Cognitive
sequelae of subthalamic nucleus deep brain stimulation in Parkinson’s
disease: a meta-analysis. Lancet Neurol 2006; 5: 578–88.
Peto V, Jenkinson C, Fitzpatrick R, Greenhall R. The development and
validation of a short measure of functioning and well being for
individuals with Parkinson’s disease. Qual Life Res 1995; 4: 241–8.
Phillips MD, Baker KB, Lowe MJ, Tkach JA, Cooper SE, Kopell BH, et al.
Parkinson disease: pattern of functional MR imaging activation during
deep brain stimulation of subthalamic nucleus – initial experience.
Radiology 2006; 239: 209–16.
Pillon B, Ardouin C, Damier P, Krack P, Houeto JL, Klinger H, et al.
Neuropsychological changes between ‘off’ and ‘on’ STN or GPi
stimulation in Parkinson’s disease. Neurology 2000; 55: 411–8.
Piper M, Abrams GM, Marks WJ Jr. Deep brain stimulation for the
treatment of Parkinson’s disease: overview and impact on gait and
mobility. NeuroRehabilitation 2005; 20: 223–32.
Rivaud-Pechoux S, Vermersch AI, Gaymard B, Ploner CJ, Bejjani BP,
Damier P, et al. Improvement of memory guided saccades in
parkinsonian patients by high frequency subthalamic nucleus stimulation. J Neurol Neurosurg Psychiatry 2000; 68: 381–4.
Rochester L, Hetherington V, Jones D, Nieuwboer A, Willems AM,
Kwakkel G, et al. Attending to the task: interference effects of functional
tasks on walking in Parkinson’s disease and the roles of cognition,
depression, fatigue, and balance. Arch Phys Med Rehabil 2004; 85:
1578–85.
Rodriguez-Oroz MC, Obeso JA, Lang AE, Houeto JL, Pollak P,
Rehncrona S, et al. Bilateral deep brain stimulation in Parkinson’s
disease: a multicentre study with 4 years follow-up. Brain 2005; 128:
2240–9.
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
Twelfth international congress of Parkinson’s disease and movement
disorders. Vol. 23. Chicago, Illinois: Wiley-Blackwell, 2008, S127.
Erola T, Karinen P, Heikkinen E, Tuominen J, Haapaniemi T,
Koivukangas J, et al. Bilateral subthalamic nucleus stimulation improves
health-related quality of life in Parkinsonian patients. Parkinsonism
Relat Disord 2005; 11: 89–94.
Fraix V, Houeto JL, Lagrange C, Le Pen C, Krystkowiak P, Guehl D, et al.
Clinical and economic results of bilateral subthalamic nucleus stimulation in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2006; 77:
443–9.
Fukuda M, Mentis M, Ghilardi MF, Dhawan V, Antonini A,
Hammerstad J, et al. Functional correlates of pallidal stimulation for
Parkinson’s disease. Ann Neurol 2001; 49: 155–64.
Galganski ME, Fuglevand AJ, Enoka RM. Reduced control of motor
output in a human hand muscle of elderly subjects during submaximal
contractions. J Neurophysiol 1993; 69: 2108–15.
Germano I, Gracies JM, Weisz D, Tse W, Koller W, Olanow C. Unilateral
stimulation of the subthalamic nucleur in Parkinson’s disease: a doubleblind 12-month evaluation study. J Neurosurg 2004; 101: 36–42.
Gironell A, Kulisevsky J, Rami L, Fortuny N, Garcia-Sanchez C, PascualSedano B. Effects of pallidotomy and bilateral subthalamic stimulation
on cognitive function in Parkinson disease. A controlled comparative
study. J Neurol 2003; 250: 917–23.
Grill WM, Snyder AN, Miocinovic S. Deep brain stimulation creates an
informational lesion of the stimulated nucleus. Neuroreport 2004; 15:
1137–40.
Gronchi-Perrin A, Viollier S, Ghika J, Combremont P, Villemure JG,
Bogousslavsky J, et al. Does subthalamic nucleus deep brain stimulation
really improve quality of life in Parkinson’s disease? Mov Disord 2006;
21: 1465–8.
Hashimoto T, Elder CM, Okun MS, Patrick SK, Vitek JL. Stimulation of
the subthalamic nucleus changes the firing pattern of pallidal neurons.
J Neurosci 2003; 23: 1916–23.
Hershey T, Revilla FJ, Wernle A, Gibson PS, Dowling JL, Perlmutter JS.
Stimulation of STN impairs aspects of cognitive control in PD.
Neurology 2004; 62: 1110–4.
Hershey T, Revilla FJ, Wernle AR, McGee-Minnich L, Antenor JV,
Videen TO, et al. Cortical and subcortical blood flow effects of
subthalamic nucleus stimulation in PD. Neurology 2003; 61: 816–21.
Hershey T, Wu J, Weaver PM, Perantie DC, Karimi M, Tabbal SD, et al.
Unilateral vs. bilateral STN DBS effects on working memory and motor
function in Parkinson disease. Exp Neurol 2007; 210: 402–8.
Jahanshahi M, Ardouin CM, Brown RG, Rothwell JC, Obeso J, Albanese A,
et al. The impact of deep brain stimulation on executive function in
Parkinson’s disease. Brain 2000; 123: 1142–54.
Jansma JM, Ramsey NF, Coppola R, Kahn RS. Specific versus nonspecific
brain activity in a parametric N-back task. Neuroimage 2000; 12:
688–97.
Kleiner-Fisman G, Herzog J, Fisman DN, Tamma F, Lyons KE, Pahwa R,
et al. Subthalamic nucleus deep brain stimulation: summary and metaanalysis of outcomes. Mov Disord 2006; 21 (Suppl 14): S290–304.
Kriz G, Hermsdorfer J, Marquardt C, Mai N. Feedback-based training of
grip force control in patients with brain damage. Arch Phys Med
Rehabil 1995; 76: 653–9.
Kurillo G, Zupan A, Bajd T. Force tracking system for the assessment of
grip force control in patients with neuromuscular diseases. Clin
Biomech 2004; 19: 1014–21.
Lindenberger U, Marsiske M, Baltes PB. Memorizing while walking:
increase in dual-task costs from young adulthood to old age. Psychol
Aging 2000; 15: 417–36.
Llinas RR, Ribary U, Jeanmonod D, Kronberg E, Mitra P. Thalamocortical
dysrhythmia: a neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proc Natl Acad Sci USA 1999; 96:
15222–7.
Lyons KE, Pahwa R. Long-term benefits in quality of life provided by
bilateral subthalamic stimulation in patients with Parkinson disease.
J Neurosurg 2005; 103: 252–5.
J. L. Alberts et al.
�Bilateral DBS impairs dual-task performance
Page 13 of 13
Temperli P, Ghika J, Villemure JG, Burkhard PR, Bogousslavsky J,
Vingerhoets FJ. How do parkinsonian signs return after discontinuation
of subthalamic DBS? Neurology 2003; 60: 78–81.
The Deep Brain Stimulation Study Group. Deep-brain stimulation of the
subthalamic nucleus or the pars interna of the globus pallidus in
Parkinson’s disease. N Engl J Med 2001; 345: 956–63.
Timmermann L, Gross J, Dirks M, Volkmann J, Freund HJ, Schnitzler A.
The cerebral oscillatory network of parkinsonian resting tremor. Brain
2003; 126: 199–212.
Uc EY, Rizzo M, Anderson SW, Sparks JD, Rodnitzky RL, Dawson JD.
Impaired navigation in drivers with Parkinson’s disease. Brain 2007;
130: 2433–40.
Vitek JL, Giroux M. Physiology of hypokinetic and hyperkinetic movement
disorders: model for dyskinesia. Ann Neurol 2000; 47: S131–40.
Vitek JL. Deep brain stimulation for Parkinson’s disease: a critical
re-evaluation of STN versus GPi DBS. Stereotact Funct Neurosurg
2002a; 78: 119–31.
Vitek JL. Mechanisms of deep brain stimulation: excitation or inhibition.
Mov Disord 2002b; 17 (Suppl 3): S69–72.
Voelcker-Rehage C, Alberts JL. Age-related changes in grasping force
modulation. Exp Brain Res 2005; 166: 61–70.
Voelcker-Rehage C, Alberts JL. Effect of motor practice on dual-task
performance in older adults. J Gerontol B Psychol Sci Soc Sci 2007; 62:
P141–8.
Voelcker-Rehage C, Stronge AJ, Alberts JL. Age-related differences in
working memory and force control under dual-task conditions.
Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 2006; 13: 366–84.
Voon V, Saint-Cyr J, Lozano AM, Moro E, Poon YY, Lang AE. Psychiatric
symptoms in patients with Parkinson disease presenting for deep brain
stimulation surgery. J Neurosurg 2005; 103: 246–51.
Wallace BA, Ashkan K, Heise CE, Foote KD, Torres N, Mitrofanis J, et al.
Survival of midbrain dopaminergic cells after lesion or deep brain
stimulation of the subthalamic nucleus in MPTP-treated monkeys. Brain
2007; 130: 2129–45.
Witt K, Pulkowski U, Herzog J, Lorenz D, Hamel W, Deuschl G, et al.
Deep brain stimulation of the subthalamic nucleus improves cognitive
flexibility but impairs response inhibition in Parkinson disease. Arch
Neurol 2004; 61: 697–700.
Woods SP, Fields JA, Troster AI. Neuropsychological sequelae of
subthalamic nucleus deep brain stimulation in Parkinson’s disease: a
critical review. Neuropsychol Rev 2002; 12: 111–26.
Woollacott M, Shumway-Cook A. Attention and the control of posture
and gait: a review of an emerging area of research. Gait Posture 2002;
16: 1–14.
Downloaded from http://brain.oxfordjournals.org/ at Pennsylvania State University on April 28, 2014
Rubin JE, Terman D. High frequency stimulation of the subthalamic
nucleus eliminates pathological thalamic rhythmicity in a computational
model. J Comput Neurosci 2004; 16: 211–35.
Saint-Cyr JA, Trepanier LL, Kumar R, Lozano AM, Lang AE.
Neuropsychological consequences of chronic bilateral stimulation of
the subthalamic nucleus in Parkinson’s disease. Brain 2000; 123:
2091–108.
Schupbach M, Gargiulo M, Welter ML, Mallet L, Behar C, Houeto JL,
et al. Neurosurgery in Parkinson disease: a distressed mind in a repaired
body? Neurology 2006; 66: 1811–6.
Schupbach WM, Chastan N, Welter ML, Houeto JL, Mesnage V,
Bonnet AM, et al. Stimulation of the subthalamic nucleus in
Parkinson’s disease: a 5 year follow up. J Neurol Neurosurg Psychiatry
2005; 76: 1640–4.
Schupbach WM, Maltete D, Houeto JL, du Montcel ST, Mallet L,
Welter ML, et al. Neurosurgery at an earlier stage of Parkinson disease: a
randomized, controlled trial. Neurology 2007; 68: 267–71.
Siderowf A, Jaggi JL, Xie SX, Loveland-Jones C, Leng L, Hurtig H, et al.
Long-term effects of bilateral subthalamic nucleus stimulation on
health-related quality of life in advanced Parkinson’s disease. Mov
Disord 2006; 21: 746–53.
Skidmore FM, Rodriguez RL, Fernandez HH, Goodman WK, Foote KD,
Okun MS. Lessons learned in deep brain stimulation for movement and
neuropsychiatric disorders. CNS Spectr 2006; 11: 521–36.
Slowinski JL, Putzke JD, Uitti RJ, Lucas JA, Turk MF, Kall BA, et al.
Unilateral deep brain stimulation of the subthalamic nucleus for
Parkinson disease. J Neurosurg 2007; 106: 626–32.
Starr PA, Vitek JL, Bakay RA. Ablative surgery and deep brain stimulation
for Parkinson’s disease. Neurosurgery 1998a; 43: 989–1013; discussion
1013–5.
Starr PA, Vitek JL, Bakay RA. Deep brain stimulation for movement
disorders. Neurosurg Clin N Am 1998b; 9: 381–402.
Tabbal SD, Ushe M, Mink JW, Revilla FJ, Wernle AR, Hong M, et al.
Unilateral subthalamic nucleus stimulation has a measurable ipsilateral
effect on rigidity and bradykinesia in parkinson disease. Exp Neurol
2008; 211: 234–42.
Temel Y, Blokland A, Ackermans L, Boon P, van KranenMastenbroek VH, Beuls EA, et al. Differential effects of subthalamic
nucleus stimulation in advanced Parkinson disease on reaction time
performance. Exp Brain Res 2006a; 169: 389–99.
Temel Y, Kessels A, Tan S, Topdag A, Boon P, Visser-Vandewalle V.
Behavioural changes after bilateral subthalamic stimulation in advanced
Parkinson disease: a systematic review. Parkinsonism Relat Disord
2006b; 12: 265–72.
Brain (2008)
�
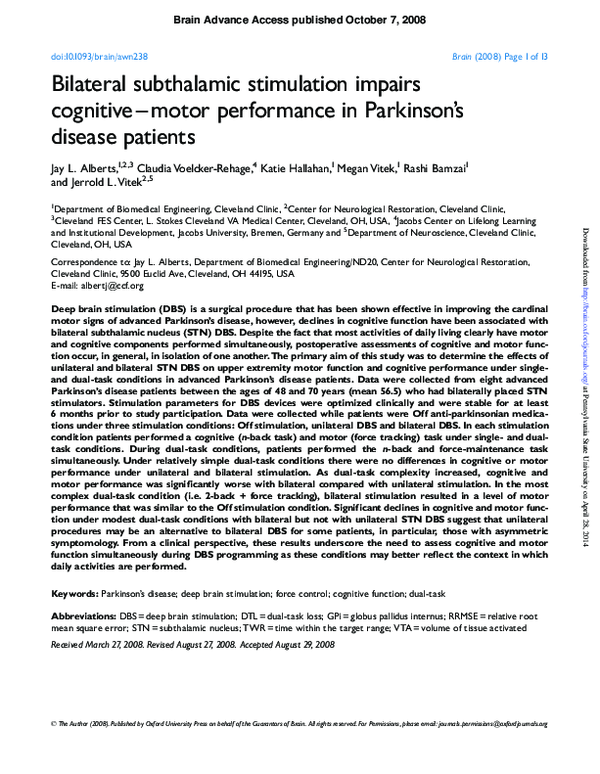
 Jay Alberts
Jay Alberts