Rheumatology 2008;47:239–248
Advance Access publication 28 November 2007
doi:10.1093/rheumatology/kem260
Review
Rheumatoid arthritis, cardiovascular disease and physical exercise:
a systematic review
G. S. Metsios1–3, A. Stavropoulos-Kalinoglou1–3, J. J. C. S. Veldhuijzen van Zanten2,4, G. J. Treharne2,5,
V. F. Panoulas2, K. M. J. Douglas2, Y. Koutedakis1,3 and G. D. Kitas2
KEY
WORDS:
Rheumatoid arthritis, Cardiovascular disease, Dynamic exercise, Aerobic exercise, Physical activity.
facilitates management and improvements of outcome in all four
of these categories. It helps maintain a healthy life-style, reduce
CVD risk factors including obesity [19], dyslipidaemia [20, 21],
hypertension [22], diabetes mellitus [23] and possibly even
inflammation [24]; it is also effective for preventing acute coronary
syndromes [25–32]. Moreover, exercise helps the management of
established CVD: both aerobic exercise [33, 34] and resistance
training [35] improve myocardial contractility and quality of life
in patients with chronic heart failure and produce significant
functional benefits in people with intermittent claudication [36].
More importantly, cardiac exercise rehabilitation programmes are
an important part in the management of patients after an acute
coronary syndrome (ACS) [37] and lead to significantly improved
quality of life and reduced mortality rates [38–40]. Interestingly,
there is evidence that patients with RA are rarely offered the
opportunity to participate in cardiac rehabilitation programmes
even after an ACS [3]. This may be, at least in part, because of the
specific considerations required when prescribing exercise to such
patients. These include: (i) whether the individual is physically
able to perform, and psychologically likely to adhere to exercise
regimens designed for cardiovascular improvements; (ii) whether
RA health professionals are sufficiently aware of the evidence
regarding exercise in RA patients and educate their patients
accordingly; and (iii) whether existing exercise programmes and
facilities can be adapted to cater for the extra needs that people
with some degree of physical disability may have.
In the present review, we describe briefly the settings and types
of exercise used for cardiovascular improvement in the general
population. We then present systematic reviews of aerobic exercise
interventions in RA and of the factors that may influence
adherence to exercise in this disease. Finally, we give suggestions
for exercise interventions suitable for improving the cardiovascular profile of people with RA and propose areas for future
research in the field.
Introduction
Rheumatoid arthritis (RA) associates with increased morbidity
and mortality from cardiovascular disease (CVD) [1], most of
which is due to greater prevalence [2] and worse outcome [3] of
ischaemic heart disease, largely attributed to accelerated atherosclerosis. The exact processes leading to this phenomenon remain
undetermined. Much attention has been paid to the potential role
of high-grade systemic inflammation [4] and its vascular and
metabolic effects [5]. Sometimes this takes the focus away from
the indisputable fact that classical modifiable CVD risk factors—
such as hypertension [6, 7], dyslipidaemia [8], insulin resistance/
metabolic syndrome [9], obesity [10], physical inactivity [11] and
smoking [12]—are highly prevalent but under-investigated and
suboptimally managed in this group of patients [13]. Even though
these risk factors are not sufficient to explain the entire magnitude
of CVD morbidity and mortality in RA [2], they represent an
easily identifiable target for intervention, using both pharmacological [14–16] and behavioural approaches [17, 18].
Exercise is one of the most important behavioural interventions
that can have a major beneficial impact on the likelihood to
develop, suffer symptomatically or die from CVD. In the context
of CVD, people, including those who have RA, could be divided
schematically into four categories: those who have neither CVD
nor any significant risk factor burden for it; those who have risk
factors but no clinical evidence of CVD; those who have clinically
apparent vascular and cardiac disease but have not suffered a lifethreatening acute cardiovascular event such as a myocardial
infarction (MI); and those who have survived an acute cardiovascular event. There is overwhelming evidence that, in the
general population and several at risk subpopulations, exercise
provides significant physical and psychosocial benefits, and
1
University of Wolverhampton, School of Sport, Performing Arts and Leisure,
Walsall, 2Department of Rheumatology, Dudley Group of Hospitals NHS Trust,
Russells Hall Hospital, Dudley, West Midlands, UK, 3Research Institute in Physical
Performance and Rehabilitation, Centre for Research and Technology Thessaly,
Trikala, Greece, 4School of Sport and Exercise Sciences and 5School of
Psychology, University of Birmingham, UK.
Methods
After taking into consideration an evidence-based tool for literature searching specifically for RA [41], six databases [Medline,
Cochrane Library, Cumulative Index to Nursing & Allied Health
Literature (CINAHL) research database, Google Scholar,
Excerpta Medica database (EMBASE) and Physiotherapy
Submitted 6 May 2007; revised version accepted 28 August 2007.
Correspondence to: G. S. Metsios, University of Wolverhampton, Walsall, West
Midlands. E-mail: gm@wlv.ac.uk
239
ß The Author 2007. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: journals.permissions@oxfordjournals.org
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
This systematic review investigates the effectiveness of exercise interventions in improving disease-related characteristics in patients with
rheumatoid arthritis (RA). It also provides suggestions for exercise programmes suitable for improving the cardiovascular profile of RA
patients and proposes areas for future research in the field. Six databases (Medline, Cochrane Library, CINAHL, Google Scholar, EMBASE
and PEDro) were searched to identify publications from 1974 to December 2006 regarding RA and exercise interventions. The quality of the
studies included was determined by using the Jadad scale. Initial searches identified 1342 articles from which 40 met the inclusion criteria.
No studies were found investigating exercise interventions in relation to cardiovascular disease in RA. There is strong evidence suggesting
that exercise from low to high intensity of various modes is effective in improving disease-related characteristics and functional ability in RA
patients. Future studies are required to investigate the effects of exercise in improving the cardiovascular status of this patient population.
�240
G. S. Metsios et al.
Exercise for the prevention and management of
cardiovascular disease
The increasing incidence and prevalence of CVD, together with its
socioeconomic impact, have raised the need for early and effective
prevention strategies (e.g. comprehensive screening and education) regarding relevant lifestyle modifications. Exercise has been
identified as one of the most important behavioural strategies for
CVD prevention. Specific guidelines have been developed about
the required amount and intensity of daily and weekly physical
activity [43], and its importance is emphasized by several
campaigns promoting an active lifestyle, including those by the
British Heart Foundation.
Any physical activity is better than no, or little, physical
activity. The overall physiological adaptations that occur as a
result of exercise [44] provide protection against CVD mortality,
even in the presence of well-established CVD risk factors [45, 46].
CVD mortality is lower in highly fit than in moderately fit
individuals [47], while physical inactivity is an independent risk
factor for the development of CVD [48, 49].
Even though cardiorespiratory fitness may have a familial
component [50], it can be increased significantly by exercise
training, regardless of age, gender, race and initial fitness levels
[51]. The required activity levels can be accrued through formal
training programmes or leisure-time physical activities [52].
Moreover, supervised exercise programmes are more effective
compared with non-supervised exercise [53, 54], most likely due to
greater adherence.
Great controversy still exists about the optimum amount of
exercise for eliciting the greatest cardiovascular benefit. Different
exercise intensity [55, 56] and duration [57], as well as various
combinations of them [58], may have different impacts on the
magnitude of cardiorespiratory fitness improvement. Most authors
agree that there is a dose–response relation between the amount of
exercise, all-cause and cardiovascular mortality [55, 57, 59].
The greatest potential for reduced mortality is in sedentary
individuals (such as many RA patients), in whom even slight
increases in daily physical activity are beneficial [59, 60]; for more
active individuals, higher levels of intensity should be pursued [59].
Depending primarily on the starting levels of physical activity,
cardiovascular fitness has been reported to increase by 8–51%
following an exercise intervention [57, 59, 61–63].
Moderate-intensity exercise of long duration appears to elicit
the most benefit on CVD risk and mortality [55, 56, 58–60].
Current guidelines by the American College of Sports Medicine
(ACSM) suggest that an individual should engage in exercise at
least three times a week, at an intensity of 60–80% of maximum
oxygen uptake (VO2max), for at least 20–30 min, in order to
experience significant improvements in cardiorespiratory fitness
and optimum cardiovascular benefits [43]. In terms of caloric
expenditure, this can be translated to 1000–2000 kcal/week [64].
These calories can be expended in either continuous exercise
or accumulated from several short bouts of exercise during a day
[64–66]. Aerobic exercise is the most appropriate, but this can be
supplemented by low-to-moderate intensity resistance training
[65, 67]. The exercise regimen should be reconsidered regularly,
usually every 4–6 weeks, based on the principles of exercise
periodization [68] so that participants continue to improve their
performance.
Exercise in RA
RA manifestations include pain, stiffness, structural joint damage,
bone density loss and muscle weakness [69]. As a result, a large
proportion of patients exhibit decreased range of movement of the
affected joints and general functional limitation in performing
daily physical tasks: this may significantly compromise their
fitness levels compared with people of the same age and sex [70].
RA patients’ fear for disease aggravation and an indefensible
traditional approach of rheumatology health professionals to
recommend exercise restriction may account for the inactive
lifestyle of this population [70, 71]. It is now established that welldesigned physical exercise programmes promote prolonged
improvements [72–74] without inducing harmful effects on disease
activity and joint damage [71, 75–77].
Thus far, the main objectives of exercise therapy in RA have
been to maintain functional ability and improvement of physical
capacity [78]. Exercise programmes with the specific purpose of
improving cardiovascular fitness and reduced CVD mortality
have attracted only minimal attention in this population.
Resistance training
Conventional resistance exercise programmes consisting of
low-impact isometric and range-of-motion exercises have been
repeatedly utilized in RA. The application of low-to-moderate
intensity strength exercise in RA patients increased physical
capacity [79, 80] without exacerbating pain or disease activity [81].
However, high-intensity resistance exercise programmes represent
a more effective means for increasing muscular strength compared
with low-intensity training and range-of-motion exercises, without
any evidence of aggravation of joint symptoms [82]. Highintensity exercise has even been reported to decelerate joint
damage in individuals with RA compared with non-exercising RA
patients [83, 84], although this remains controversial [85, 86].
Some patients with extensive structural damage may have to
refrain from activities that include significant loading of the
damaged joints [87].
Well-constructed progressive resistance exercise is an effective
and safe intervention for stimulating muscle growth in patients
with RA and may even reverse rheumatoid cachexia [88]. This
metabolic abnormality, which affects nearly two-thirds of all
individuals with RA, is characterized by involuntary loss of
muscle mass and progressive increase of fat mass in the presence
of stable or even slightly decreased weight [89]. The exact
underlying mechanisms are not entirely clear [90]: possible
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
Evidence Database (PEDro)] were searched to identify publications from 1974 to December 2006 in English regarding RA and
exercise interventions. The Medical Subject Heading (MeSH)
terms ‘physical activity’, ‘training’ and ‘exercise’ were employed in
combination with ‘rheumatoid arthritis’. Initial searches identified
1342 articles (Supplementary Fig. S1, available at Rheumatology
Online). Full articles were retrieved for assessment if the
information in the abstract fulfilled both of the following criteria:
(i) studying any aerobic or aerobic combined with resistance
exercise intervention; and (ii) involving RA patients. Studies
incorporating only participants with various types of inflammatory arthritis, degenerative arthritis or other inflammatory or
connective tissue diseases were excluded. If the title and abstract
did not provide sufficient information for this process, then the
full-text manuscript was examined. Conference proceedings were
not included in the review. The quality of the identified
randomized controlled trials (RCTs) was assessed using standardized procedures as previously described [42]. Due to the limited
number of RCTs for certain types of exercise (e.g. dance), crosssectional and non-randomized longitudinal studies are also
presented in the tables. However, the main conclusions and
recommendations in this review are based on the results of RCTs.
For adherence to exercise in RA, keyword searches of
Medline were carried out using the terms ‘exercise’ and all root
variations on ‘adherence’ (e.g. ‘nonadherent’) and ‘compliance’
(e.g. ‘complying’) in combination with ‘rheumatoid arthritis’
(Supplementary Table S1, available at Rheumatology Online).
Half of the identified studies were interventions with a focus on
exercise component, and the majority contained only limited
information on the role of adherence/compliance.
�Exercise and rheumatoid arthritis
contributing factors not only include the overproduction of
inflammatory cytokines such as TNF-a [89] but also physical
inactivity [91, 92].
Non-RCTs investigating the effects of resistance training in
RA differ widely in training regimens, methodological approaches
and outcomes, making any conclusions difficult. The effectiveness
of strength training lies on the quality and quantity of its
application. Indeed, incorrect application of exercise frequency
and intensity may not induce improvements in muscular strength;
according to the ACSM [93], a successful muscular strength
training programme for older populations or individuals with
sedentary lifestyles should incorporate at least two sessions per
week, involve 8–10 exercises for different muscle groups and allow
completion of one set of 10–15 repetitions per exercise. RCTs
complying to these recommendations have revealed significant
increases in functional ability [74, 84, 94] and muscular strength
[75], without exacerbating existing joint damage [73, 95] in
patients with RA.
241
appears to consistently induce beneficial effects in aerobic
capacity, functional ability and muscle strength.
Dance. The effects of dance exercise have been investigated in
many non-randomized trials (Table 3), which suggest improvements in aerobic capacity, walking ability, muscular strength
[115–117] and psychological parameters, such as anxiety and
depression [115, 118]. The only randomized trial involving dance
as an intervention in RA patients revealed that despite no
significant changes in bone mineral density and disease activity,
functional capacity and physical activity were significantly
improved [119].
Aerobic training
Patients with RA are less active, and therefore less physically fit,
compared with healthy individuals of the same age [70, 96]. The
most frequently used mode of aerobic exercise training in studies
involving RA patients is cycling, followed by aquatic exercise,
aerobic dance and walking/running.
Cycling. Cycling is a non-weight-bearing aerobic activity
where participants utilize large muscle groups of the lower
extremity. It can be performed both in clinical settings as well as
outdoors, either individually or in groups [97]. Indoor cycles can
be modified to accommodate the needs of almost every RA
patient [98] and can be effective even when the patients are
minimally supervised [99]. An overview of the studies using cycling
is provided in Table 1. Although individual studies vary in exercise
frequency and overall duration of the intervention, cycling
Walking and running. Walking has been used as an
intervention for improving patients’ disease status [108, 121,
122], for the assessment of functional ability via gait analyses
[123–125] or walking tests [126], and as a method to predict
maximal oxygen uptake [127]. Walking or jogging has been
included in training programmes without specifying the exact
intensity, duration and frequency, but no RCTs based on walking
or running as the main mode of exercise have been conducted
TABLE 1. Interventional training regimens in patients with rheumatoid arthritis—cycling programmes
Cycling programmes
EG
CG
Main outcomes
Ekblom et al. [100, 101]
Author [reference]
34 RA
DS ¼ 25–40 min
Intensity ¼ 50–70% of HRmax
Frequency ¼ 5 d/wk, twice daily
PD ¼ 5 wk and 6 months
Rehabilitation programme
Acute increase in aerobic capacity,
walk test
No change in pain perception
Long term ¼ increase in aerobic
capacity, muscle strength
2
Harkcom et al. [102]
17 RA
DS ¼ 15, 25 or
35 min
Intensity ¼ 70% of HRmax
Frequency ¼ 3 d/wk
PD ¼ 12 wk
Routine activities
Acute increase in aerobic capacity,
exercise tolerance
Decrease in disease activity
2
Karper and Evans [103]
1 RA
DS ¼ 20–30 min
Intensity ¼ 50–70 Watts
Frequency ¼ 3 d/wk
PD ¼ 14 wk
Improvement of physiological and
psychological status
Case study
Lyngberg et al. [104]
18 RA
DS ¼ 15–45 min
Intensity ¼ 50–70% of HRmax
Frequency ¼ 2 d/wk
PD ¼ 8 wk
Routine activities
Acute decrease in disease activity
Strength and aerobic status not
reported
No
randomization
Baslund et al. [105]
18 RA
EG ¼ 8
CG ¼ 8
DS ¼ 15–30 min
Intensity ¼ 80% of HRmax
Frequency ¼ 4–5 d/wk
PD ¼ 8 wk
Current physical activities
Increase in aerobic capacity
No changes on the immune system
(blood mononuclear cells, proliferative response, natural killer cell
activity)
2
Lyngberg et al. [94]
24 RA
EG ¼ 12
CG ¼ 12
DS ¼ 45 min
Intensity ¼ 50–70% of HRmax
Frequency ¼ 2 d/wk
PD ¼ 3 months
Current activities
Increase in functional capacity and
strength
No significant differences were
observed in ESR, number of tender
joints and morning stiffness
2
n
Quality
d/wk, day/week; RA, rheumatoid arthritis; EG, intervention for experimental group; CG, intervention for control group; DS, duration of session in minutes; PD, programme duration; HRmax, maximal
heart rate in beats per minute; ESR, erythrocyte sedimentation rate; n, number of participants.
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
Aquatic. Different types of water-based exercises such as
aqua-aerobics and deep-water running have been applied in
people with RA (Table 2). The in-water environment is thought to
provide the ideal means for exercising in this population, as
weight-bearing is minimized due to buoyancy [106]. This is
extended by the general belief of patients that this type of exercise
improves their functional ability [107]. Most of the available
evidence suggests that aquatic exercise does improve aerobic
capacity [108–110], muscular strength [85, 111] and psychological
status [109]. The RCT with the larger number of RA patients
combining both warm water immersion and exercise revealed
significant improvements, as assessed by the Arthritis Impact
Measurement Scales 2. However, this study did not include a
laboratory-based evaluation of physical activity [109].
�G. S. Metsios et al.
242
TABLE 2. Interventional training regimens in patients with rheumatoid arthritis—aquatic programmes
Aquatic programmes
Author [reference]
EG
n
CG
8 RA
Water exercise
Stenstrom et al. [85]
60 RA
DS ¼ 30–40 min
Frequency ¼ 1 d/wk
PD ¼ 4 yrs
Hansen et al. [86]
75 RA
EG ¼ 45
CG ¼ 15
Minor and Hewett [113]
Results
Quality
Increase in maximal quadriceps strength
Increase in aerobic capacity
No randomization
Medical treatment
Increase in activity level, grip strength
No changes functional/psychological
status. Controls had significantly more
admittances for acute hospital care
No randomization
DS ¼ 45–90 min
Frequency ¼ 3 d/wk
PD ¼ 2 yrs
Normal treatment
No effect of training on disease activity and
damage progression
2
42 RA
EG ¼ 20
CG ¼ 22
DS ¼ NS
Intensity ¼ NS
Frequency ¼ 3 d/wk
PD ¼ 12 wk
Received no attention
apart from the testing
Improved aerobic capacity and exercise
tolerance
No randomization
Rintala et al. [114]
34 RA
EG ¼ 18
CG ¼ 16
DS ¼ 45–60 min
Intensity ¼ individualized
Frequency ¼ 2 d/wk
PD ¼ 24 sessions
Normal daily activities
Improved muscle strength and mobility
No increases in aerobic capacity
1
Hall et al. [109]
139 RA
DS ¼ 30 min
Intensity ¼ NS
Frequency ¼ 2 d/wk
PD ¼ 3 months
Seated immersion
Physical (AIMS2) and psychological benefits (mood and tension) were apparent in
all groups
Hydrotherapy resulted in the greatest
improvements
2
Sanford-Smith et al. [111]
24 RA
DS ¼ 25–60 min
Intensity ¼ 70% of HRmax
Frequency ¼ 3 d/wk
PD ¼ 10 wk
ROM and isometric
exercises
Increase in both grip strength and exercise
tolerance and decrease in ESR
Trend for improved HAQ
2
Bilberg et al. [107]
46 RA
EG ¼ 20
CG ¼ 26
DS ¼ 45 min
Frequency ¼ 2 d/wk
PD ¼ 12 wk
Normal activities
No changes in aerobic capacity
Increased perception of physical function
and muscular function
3
d/wk, day/week; n, number of participants; RA, rheumatoid arthritis; EG, intervention for experimental group; CG, intervention for control group; DS, duration of session in minutes; PD, programme
duration; NS, not specified; HRmax, maximal heart rate in beats per minute; ROM, range-of-motion; AIMS2, arthritis impact measurement scales 2; ESR, erythrocyte sedimentation rate; HAQ, health
assessment questionnaire.
TABLE 3. Interventional training regimens in patients with rheumatoid arthritis—dancing programmes
Dancing programmes
Author [reference]
n
EG
Perlman et al. [118]
43 RA
DS ¼ 30–60 min
Intensity ¼ 60–70% of HRmax
Frequency ¼ 2 d/wk
PD ¼ 16 wk
Noreau et al. [115]
29 RA
DS ¼ 30–60 min
Intensity ¼ 50–70% of HRmax
Frequency ¼ 2 d/wk
PD ¼ 12 wk
Noreau et al. [116]
10 RA
Neuberger et al. [117]
CG
Results
Quality
Increase in performance of 50 ft walk
Decrease in pain and depression
No randomization
Increase in performance of 50 ft walk,
aerobic power, hamstring strength and
mood state
Decrease in pain, depression and
anxiety
No randomization
DS ¼ 25–60 min
Intensity ¼ 50–70% of HRmax
Frequency ¼ 2 d/wk
PD ¼ 8 wk
Increase in 6 min walk distance and
improved psychological state
No significant changes in aerobic
capacity, disease activity
No randomization
25 RA
Low impact aerobic dance
Decreased fatigue in the patients who
participated the most
Increased aerobic fitness and grip
strength
Decreased pain and walk time
No significant increases in joint count
or ESR
No randomization
Westby et al. [119]
53 RA women
EG ¼ 23
CG ¼ 30
DS ¼ 45–60 min
Intensity ¼ NS
Frequency ¼ 3 d/wk
PD ¼ 12 months
Improved functional capacity and
activity level
BMD did not differ significantly
between groups
No change in disease activity
2
Moffet et al. [120]
10 RA
DS ¼ 45–60 min
Intensity ¼ 50–70% of HRmax
PD ¼ 8 wk
Significant improvement in locomotion
ability and walking ability
No randomization
Counselling sessions
Habitual physical activities
and therapy
n, number of participants; RA, rheumatoid arthritis; EG, intervention for experimental group; CG, intervention for control group; DS, duration of session in minutes; PD, programme duration; NS, not
specified; HRmax, maximal heart rate in beats per minute; BMD, bone mineral density; d/wk, day/week.
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
Danneskiold-Samsoe et al. [112]
�Exercise and rheumatoid arthritis
in RA. Interestingly, a case study has described a female with RA
who completed a whole marathon run following a training
programme [128].
Combination of aerobic and strength training. The com-
Adherence to exercise in RA
Consistent engagement in an exercise regimen is essential to reach
improvements in fitness and physical well-being as well as
psychological benefits in people with RA. We therefore carried
out a systematic investigation of the evidence as to whether RA
patients adhere to exercise regimens and what factors may
influence this. In general, adherence/compliance has either been
mentioned in relation to lack of long-term continuation of exercise
after an intervention [139] or has been investigated in exercise
regimes not specifically targeted at RA patients [99, 140–148].
This has made it difficult to reach any definitive conclusion [139,
149–158]. The Ottawa Panel’s meta-analysis [154] reviewing
previous RCTs of exercise regimens for RA patients demonstrated
that adherence/compliance was included as an outcome only in
two studies [148, 159]; the first was excluded from the metaanalysis for being a head-to-head study rather than a fully
controlled study (it assessed dynamic muscle training vs progressive muscle relaxation) [148]; the second was excluded for having
adherence as the sole outcome with little specific detail of the
content of the (hand only) exercise intervention [159]. Other
studies can also be criticized for inadequate-sized samples, short
follow-up, inappropriate control conditions and poor conformity
with the interventions [151]. Long-term adherence may be
particularly important as a 12-week RCT comparing dynamic
exercise with isometric and range-of-motion exercises among RA
patients found that benefits for aerobic capacity and strength were
lost another 12 weeks after the intervention [129]. O’Grady et al.
[153] also stated that long-term adherence would be required for
sustained cardiovascular benefits in RA patients, but none of the
studies they reviewed had addressed this.
General patient education has been reported to be effective in
increasing the time spent exercising [141, 142]; however, this is not
a consistent finding [146]. It seems that increased adherence to
exercise associates with lower baseline functional disability and
disease activity [160] as well as the baseline levels of physical
activity and fatigue [99]. Social factors, such as support of friends,
significantly contribute to increased adherence to exercise regimens [145]. This suggests that appropriate regimens should be
chosen for patients with more severe disease; dance sessions,
for example, have high attendance [120], which is potentially due
to the relatively low demands of this mode of exercise together
with its social component. Indeed, tailoring exercise regimens has
been suggested to improve adherence [144, 153].
In summary, adherence to exercise has not been adequately
studied in RA. High-quality evidence is rare, and appears to
suggest that well-controlled disease, better functional ability and
strong social structure may facilitate adherence to exercise by
patients with RA. Rigorous investigations are required to test
whether tailoring exercise regimens around these considerations
improves long-term adherence and goes on to improve cardiovascular outcomes for these patients.
RA, cardiovascular disease and exercise
Suggestions for future practice and research
We propose the systematic introduction of exercise training as
part of the routine multidisciplinary care of patients with RA,
with the specific aim of reducing cardiovascular risk and
preventing or managing CVD. This will require further research,
adaptation of existing knowledge and resources where available,
as well as development of new services.
Education on the cardiovascular aspects of rheumatoid disease
and the role of exercise in preventing CVD and managing RA
itself is a major area for future research and clinical practice
development; this needs to be targeted both to patients and to
healthcare professionals, aiming to achieve not just improved
knowledge but mainly sustained lifestyle changes. This may
require a combination of approaches, including behavioural
approaches, involving several healthcare professionals [161].
It can link in with the further research required into ways of
optimising long-term adherence to an active lifestyle and exercise
regimes in this population.
The short- and longer-term effects of different exercise regimens
on important metabolic factors and on vascular function need to
be specifically investigated in the RA population. These have
never been researched in any populations characterized by ‘high
grade’ systemic inflammation, where their regulation may be
under overwhelming pressure from inflammatory networks [4]
rendering them less susceptible to beneficial change through
exercise. Ultimately, long-term RCTs are needed to show whether
structured exercise programmes can be adhered to in the long
term, provide sustained cardiovascular benefits and reduce CVD
mortality in RA.
In the meantime, a pragmatic approach can be taken, building upon existing infrastructure, knowledge and expertise.
Rheumatology clinical nurse specialists [162], liaising with their
cardiology counterparts and local cardiac rehabilitation services,
can incorporate the important role of exercise in their RA patient
education programmes. Equipment and expertise available in
cardiac rehabilitation centres and community fitness clubs can be
adopted to provide exercise opportunities and classes for people
with variable (and changing) degrees of physical disability, such as
those with RA. Exercise can then be ‘prescribed’ on the basis of a
person’s exact needs.
In Fig. 1, we propose a general schema of the factors that need
to be considered in any patient with RA, and their possible
operationalization, with regard to the main objectives of their
personalized exercise regimen. This includes two main categories
of factors: (i) cardiovascular status and objectives; and (ii) overall
and specific physical ability to exercise, related to RA status. We
suggest as general principles that: (i) exercise is part of the general
management of the RA patient and can be facilitated by other
interventions (e.g. pharmacological, educational, behavioural);
(ii) its main targets are first the attainment and maintenance of
optimal (for the individual patient) function of the musculoskeletal system, which can then facilitate exercises focused on
cardiorespiratory fitness; and (iii) exercise is tailored to the
individual (although it can be delivered in a group environment),
taking into account their baseline fitness and physical ability as
well as their personal preferences and objectives, so that ideally
a concordance of objectives can be achieved between the patients
and the therapist [162].
Cardiovascular status. We suggest a schematic division into
those in whom exercise is aimed at reducing/managing CVD risk
and those in whom it is incorporated in the management of
existing CVD (before or after an acute coronary syndrome).
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
bination of intensive aerobic and strength training has been the
most widely used exercise regimen in recent research in RA and
produces an effective physical stimulus to achieve desirable
physiological adaptations (Table 4). An RCT by van den Ende
and colleagues [129] has highlighted that combining intense
aerobic and resistance training can lead to significant enhancement in both cardiorespiratory capacity and muscular strength.
Other RCTs support the beneficial effects of this type of
exercise in patients with recent-onset [95], active [129] or inactive
RA [130]. As a result of these findings, the American College of
Rheumatology updated the treatment guidelines to introduce
dynamic exercise as an effective means for the management of
RA [131].
243
�G. S. Metsios et al.
244
TABLE 4. Interventional training regimens involving the combination of dynamic aerobic and strength exercises in patients with rheumatoid arthritis
Programme
Author [reference]
n
EG
10 RA
DS ¼ 23 h/wk
Aerobic ¼ 50–70%
of VO2max
Strength ¼ NS
PD ¼ 7 months
Nordemar et al. [83]
46 RA
EG ¼ 23
CG ¼ 23
DS ¼ 30–60 min
Intensity ¼ varied
according to the patient
PD ¼ 4–8 yrs
Stenstrom [133]
42 RA
van den Ende et al. [129]
CG
Results
Quality
Small increase in muscle
fibre size
Decrease in pain
Increase in muscular strength
No changes in VO2max
No randomization
Pharmaceutical
therapy
EG less progression of joint
damage than CG
Increase in walking ability and
quadriceps torque
No changes in oxygen
consumption and heart rate
1
DS ¼ NS
Intensity ¼ NS
Frequency ¼ 5 d/wk
PD ¼ 12 wk
Same as EEG group
with different
instructions
Better self-efficacy, functional
capacity, less pain, lowered
Ritchie index and increased
mobility in the EEG group
2
100 RA 3 EG
each n ¼ 25
CG ¼ 25
DS ¼ 60 min
Intensity ¼ 70–85% of HRmax
Frequency ¼ 3 d/wk
PD ¼ 12 wk
ROM home
exercises
Intensive dynamic training is
more effective than all other
groups in increasing aerobic
fitness, joint mobility and strength
2
Komatireddy et al. [134]
49 RA
EG ¼ 25
CG ¼ 24
Circuit training
DS ¼ 20–27 min
Strength ¼ NS
Frequency ¼ 3 d/wk
PD ¼ 12 wk
Habitual activities
Increase in functional capacity
No significant change in aerobic
fitness
2
Hakkinen et al. [74]
65 RA
EG ¼ 32
CG ¼ 33
DS ¼ 45 min
Aerobic ¼ NS
Strength ¼ 50–70% of MVC
Frequency ¼ 2 d/wk
PD ¼ 12 months
Recreational physical
activities and ROM
exercises
Increases of EG in all muscle
groups examined greater than
that in CG
No effect in disease activity
No changes in BMD between
groups
2
van den Ende et al. [130]
64 RA
EG ¼ 34
CG ¼ 30
DS ¼ NS
Aerobic ¼ 60% of HRmax
Strength ¼ 70% of MVC
Frequency ¼ 3–5 d/wk
PD ¼ 24 wk
ROM and isometric
exercises
EG: physical and muscular
strength improvement, decrease
in disease activity
CG: decrease in disease activity,
muscular strength improvement
(less than EG)
3
Hakkinen et al. [135]
70 RA
EG ¼ 35
CG ¼ 35
DS ¼ 30–45 min
Aerobic ¼ NS
Strength ¼ 50–70% of MVC
Frequency ¼ 2 d/wk
PD ¼ 24 month
ROM and stretching
exercises
Increased strength, HAQ,
walking speed more pronounced
in EG
BMD increased in EG and
decreased in CG
3
de Jong et al. [73]
309 RA
EG ¼ 151
CG ¼ 158
DS ¼ 90 min
Frequency ¼ 2 d/wk
Aerobic ¼ 70–90% of HRmax
Strength ¼ NS
PD ¼ 2 yrs
Habitual physical
activity
Significant improvement in
functional ability in EG
No radiological damage in any
group
3
Hakkinen et al. [136]
70 RA
EG ¼ 35
CG ¼ 35
DS ¼ NS
Frequency ¼ 2 d/wk
Aerobic ¼ NS
Strength ¼ 50–70% of MVC
PD ¼ 24 months
ROM and stretching
exercises
Improvement in strength, HAQ
and overall function capacity
3
Hakkinen et al. [137]
23 RA
DS ¼ 45–60 min
Frequency ¼ 3 d/wk
Aerobic ¼ progressive load
Strength ¼ progressive load
PD ¼ 21 wk
The same intervention in healthy
individuals
Significant muscular strength,
walking speed, vertical jump and
aerobic capacity
No randomization
de Jong et al. [138]
RAPIT programme
309 RA
EG ¼ 151
CG ¼ 158
DS ¼ 90 min
Frequency ¼ 2 d/wk
Aerobic ¼ 70–90% of
predicted HRmax
Strength ¼ NS
PD ¼ 2 yrs
Habitual physical
activity
Exercise results in slowing down
in the loss of BMD at the hip
3
de Jong et al. [84]
RAPIT programme
309 RA
EG ¼ 151
CG ¼ 158
DS ¼ 90 min
Frequency ¼ 2 d/wk
Aerobic ¼ 70–90% of
predicted HRmax
Strength ¼ NS
PD ¼ 2 yrs
Habitual physical
activity
No progression of hand and feet
damage is not increased
3
Hakkinen et al. [75]
70 RA
EG ¼ 35
CG ¼ 35
DS ¼ 45 min
Frequency ¼ 2 d/wk
Aerobic ¼ NS
Strength ¼ 50–70% of MVC
PD ¼ 2 yrs follow-up
after 5 years
ROM and stretching
exercises
Strength gains during the 2-yr
training programme were
maintained
More favourable development of
BMD in EG group
Radiological damage remained
low
3
(continued)
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
Nordemar et al. [132]
�Exercise and rheumatoid arthritis
245
TABLE 4. Continued
Programme
Author [reference]
EG
n
CG
Results
Munneke et al. [87]
RAPIT programme 309 RA
EG ¼ 151
CG ¼ 158
DS ¼ 90 min
Habitual physical activity Dynamic training accelerates
Frequency ¼ 2 d/wk
joint damage progression in
Aerobic ¼ 70–90% of HRmax
patients with pre-existing
Strength ¼ NS
extensive damage
PD ¼ 2 yrs
Hakkinen et al. [126]
23 RA 12 healthy matched
controls
DS ¼ 30–45 min
Frequency ¼ 2–3 d/wk
Aerobic ¼ NS
Strength ¼ 50–70% of MVC
PD ¼ 21 wk
The same as EG group
Significant increases in
VO2max, muscle strength and
EMG activity in both groups
Quality
3
No randomization
Cardiovascular status
Reducing/managing CVD Risk
Little risk
Higher risk
Existing CVD
Pre-acute event
Post-acute event
Baseline cardiorespiratory fitness
Available infrastructure
Little inflammation
Little damage
Personal preferences
RA patient
Little inflammation
Much damage
Good physical ability
Active inflammation
Little damage
Active inflammation
Much damage
Limited physical ability
Rheumatoid arthritis status
FIG. 1. Major considerations in designing individualized exercise training in patients with rheumatoid arthritis.
Exercise for the latter has already been discussed in previous
sections (but will need to be adopted according to the individual
patient’s physical constraints, as discussed subsequently). For the
former, the ACSM has developed a risk stratification algorithm,
in order to optimize the safety of participation in exercise
programmes. This is based on consideration of the following
specific risk factors: total cholesterol >6.5 mmol/l; smoking;
family history of CVD; sedentary lifestyle; diabetes mellitus
(blood glucose >6.7 mmol/l); systolic blood pressure >140 mmHg
and overweight or obesity with BMI >25 kg/m2: individuals with
less than three of these components are considered at low risk for
developing CVD-related complications while exercising, whereas
those with three or more of these components are at higher risk
[43]. The thresholds for some of these risk factors may need to be
altered for the RA population: for example, total cholesterol may
be spuriously low during periods of active RA [8] and BMI
thresholds for overweight reduced to 23 kg/m2, as recently
described [10]. Based on this, exercise of appropriate mode,
intensity, duration and frequency can be designed to provide
adequate workload for cardiovascular benefits [68]. There is a
wide range of options, but current ACSM guidance for optimum
cardiovascular benefits and enhanced cardiorespiratory capacity
includes regular participation (>3 times weekly) at sufficient
intensities (60–80% of VO2max) and time (at least 20–30 min) [43].
Thus, determining the current level of fitness (usually by a graded
exercise test, during which the workload is increased at regular
intervals until self-reported exhaustion) prior to starting an
exercise intervention, will help to establish the appropriate
workload for each individual and to refine their personalized
exercise programme.
Physical ability to exercise. We have schematically divided
patients into those with good overall physical ability (mostly those
with little current inflammation and little accumulated permanent
joint damage); and those with limited physical ability (usually
patients with a lot of joint inflammation, a lot of structural joint
damage or both). This can help refine the overall multidisciplinary
approach, incorporating specific exercise regimens, to their treatment. In the former, pharmacological therapy would be aimed at
maintaining good disease control; some range of motion exercises
and resistance training could be utilized to maintain a good level of
musculoskeletal system mobility and function; and the main focus
should be aerobic training aiming at optimizing cardiovascular
fitness, to the degree determined by their current levels of fitness
and allowed by their cardiovascular risk stratification. Patients in
the group with limited physical ability to exercise due to the
impact of RA have been subdivided into three subgroups: In
those with a lot of current inflammation, but little structural
damage, we propose aggressive pharmacological therapy to
quickly reduce active inflammation and prevent muscle loss, due
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
n, number of participants; RA, rheumatoid arthritis; EG, intervention for experimental group; CG, intervention for control group; DS, duration of session in minutes; PD, programme duration;
NS, not specified; HRmax, maximal heart rate in beats per minute; ROM, range-of-motion; MVC, maximal voluntary contraction; BMD, ¼bone mineral density; VO2max, maximal oxygen uptake;
HAQ, health assessment questionnaire; EMG, Electromyography; d|wk, day|week.
�G. S. Metsios et al.
246
Conclusions. Surprisingly little has been investigated and
published on the role of exercise as a means to control risk and
manage CVD in individuals with RA. Focused research is
required to identify the optimal regimens, timing and environment
for exercise, as well as educational and behavioural interventions
that will facilitate long-term adherence to an active lifestyle and/or
structured exercise. In the meantime, a pragmatic approach is
proposed, incorporating combined range of motion, strength and
aerobic training, provided in a patient-specific context as part of
the multidisciplinary care of the individual with RA.
Rheumatology key messages
� Exercise is effective in reversing joint damage in RA patients.
� RA-specific considerations should be taken into account when
developing exercise programmes aiming to reduce CVD-risk of
this population.
Acknowledgements
Funding: G.S.M. was supported by grants received from the Greek
State Scholarships Foundation (IKY). This study was funded by
the Dudley Group of Hospitals R&D directorate cardiovascular
programme grant and a Wolverhampton University equipment
grant.
The Department of Rheumatology, Dudley Group of
Hospitals, has an infrastructure support grant from the Arthritis
Research Campaign (number: 17682).
Disclosure statement: The authors have declared no conflicts of
interest.
Supplementary data
Supplementary data are available at Rheumatology Online.
References
1 Kitas GD, Erb N. Tackling ischaemic heart disease in rheumatoid arthritis.
Rheumatology 2003;42:607–13.
2 del Rincon ID, Williams K, Stern MP, Freeman GL, Escalante A. High incidence of
cardiovascular events in a rheumatoid arthritis cohort not explained by traditional
cardiac risk factors. Arthritis Rheum 2001;44:2737–45.
3 Douglas KM, Pace AV, Treharne GJ et al. Excess recurrent cardiac events in
rheumatoid arthritis patients with acute coronary syndrome. Ann Rheum Dis
2005;65:348–53.
4 Sattar N, McCarey DW, Capell H, McInnes IB. Explaining how ‘high-grade’ systemic
inflammation accelerates vascular risk in rheumatoid arthritis. Circulation
2003;108:2957–63.
5 Stevens RJ, Douglas KM, Saratzis AN, Kitas GD. Inflammation and atherosclerosis
in rheumatoid arthritis. Expert Rev Mol Med 2005;7:1–24.
6 Erb N, Pace AV, Douglas KM, Banks MJ, Kitas GD. Risk assessment for coronary
heart disease in rheumatoid arthritis and osteoarthritis. Scand J Rheumatol
2004;33:293–9.
7 McEntegart A, Capell HA, Creran D, Rumley A, Woodward M, Lowe GD.
Cardiovascular risk factors, including thrombotic variables, in a population with
rheumatoid arthritis. Rheumatology 2001;40:640–4.
8 Situnayake RD, Kitas G. Dyslipidemia and rheumatoid arthritis. Ann Rheum Dis
1997;56:341–2.
9 Dessein PH, Tobias M, Veller MG. Metabolic syndrome and subclinical atherosclerosis in rheumatoid arthritis. J Rheumatol 2006;33:2425–32.
10 Stavropoulos-Kalinoglou A, Metsios GS, Koutedakis Y et al. Redefining overweight
and obesity in rheumatoid arthritis patients. Ann Rheum Dis 2007; in press.
11 Carnethon MR, Gulati M, Greenland P. Prevalence and cardiovascular disease
correlates of low cardiorespiratory fitness in adolescents and adults. JAMA
2005;294:2981–8.
12 Gerli R, Sherer Y, Vaudo G et al. Early atherosclerosis in rheumatoid arthritis:effects
of smoking on thickness of the carotid artery intima media. Ann NY Acad Sci
2005;1051:281–90.
13 Banks M, Kitas G. Patients’ physical disability may influence doctors’ perceptions of
suitability for risk assessment of CHD. Br Med J 1999;319:1266–7.
14 McInnes IB, McCarey DW, Sattar N. Do statins offer therapeutic potential in
inflammatory arthritis? Ann Rheum Dis 2004;63:1535–7.
15 Endres M. Statins: potential new indications in inflammatory conditions. Atheroscler
Suppl 2006;7:31–5.
16 Gonzalez-Gay MA, Garcia-Unzueta MT, De Matias JM et al. Influence of anti-TNFalpha infliximab therapy on adhesion molecules associated with atherogenesis in
patients with rheumatoid arthritis. Clin Exp Rheumatol 2006;24:373–9.
17 Myers J. Cardiology patient pages. Exercise and cardiovascular health. Circulation
2003;107:e2–5.
18 Carroll S, Dudfield M. What is the relationship between exercise and
metabolic abnormalities? A review of the metabolic syndrome. Sports Med
2004;34:371–418.
19 Bensimhon DR, Kraus WE, Donahue MP. Obesity and physical activity: a review. Am
Heart J 2006;151:598–603.
20 Svendsen OL, Hassager C, Christiansen C. Effect of an energy-restrictive diet, with
or without exercise, on lean tissue mass, resting metabolic rate, cardiovascular risk
factors, and bone in overweight postmenopausal women. Am J Med
1993;95:131–40.
21 Stefanick ML, Mackey S, Sheehan M, Ellsworth N, Haskell WL, Wood PD. Effects of
diet and exercise in men and postmenopausal women with low levels of HDL
cholesterol and high levels of LDL cholesterol. N Engl J Med 1998;339:12–20.
22 Kelemen MH, Effron MB, Valenti SA, Stewart KJ. Exercise training combined with
antihypertensive drug therapy. Effects on lipids, blood pressure, and left ventricular
mass. JAMA 1990;263:2766–71.
23 Wallberg-Henriksson H, Rincon J, Zierath JR. Exercise in the management of noninsulin-dependent diabetes mellitus. Sports Med 1998;25:25–35.
24 Kasapis C, Thompson PD. The effects of physical activity on serum C-reactive
protein and inflammatory markers: a systematic review. J Am Coll Cardiol
2005;45:1563–9.
25 Noda H, Iso H, Toyoshima H et al. Walking and sports participation and mortality
from coronary heart disease and stroke. J Am Coll Cardiol 2005;46:1761–7.
26 Shaw DI, Hall WL, Williams CM. Metabolic syndrome: what is it and what are the
implications? Proc Nutr Soc 2005;64:349–57.
27 Murtagh EM, Boreham CA, Nevill A, Hare LG, Murphy MH. The effects of 60 minutes
of brisk walking per week, accumulated in two different patterns, on cardiovascular
risk. Prev Med 2005;41:92–7.
28 Balagopal P, George D, Patton N et al. Lifestyle-only intervention attenuates the
inflammatory state associated with obesity: a randomized controlled study in
adolescents. J Pediatr 2005;146:342–8.
29 Sesso HD, Paffenbarger RS Jr, Lee IM. Physical activity and coronary heart disease
in men: The Harvard Alumni Health Study. Circulation 2000;102:975–80.
30 Blair SN, Kohl HW, Barlow CE. Physical activity, physical fitness, and
all-cause mortality in women: do women need to be active? J Am Coll Nutr
1993;12:368–71.
31 Ornish D, Brown SE, Scherwitz LW et al. Can lifestyle changes reverse coronary
heart disease? The Lifestyle Heart Trial. Lancet 1990;336:129–33.
32 Ornish D, Scherwitz LW, Billings JH et al. Intensive lifestyle changes for reversal of
coronary heart disease. JAMA 1998;280:2001–7.
33 Haykowsky M, Vonder Muhll I, Ezekowitz J, Armstrong P. Supervised exercise
training improves aerobic capacity and muscle strength in older women with heart
failure. Can J Cardiol 2005;21:1277–80.
34 Klocek M, Kubinyi A, Bacior B, Kawecka-Jaszcz K. Effect of physical training on
quality of life and oxygen consumption in patients with congestive heart failure. Int J
Cardiol 2005;103:323–9.
35 Levinger I, Bronks R, Cody DV, Linton I, Davie A. The effect of resistance training on
left ventricular function and structure of patients with chronic heart failure. Int J
Cardiol 2005;105:159–63.
36 Leng GC, Fowler B, Ernst E. Exercise for intermittent claudication. Cochrane
Database Syst Rev 2000;CD000990.
37 Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary
prevention programs for patients with coronary artery disease. Ann Intern Med
2005;143:659–72.
38 Rees K, Taylor RS, Singh S, Coats AJ, Ebrahim S. Exercise based rehabilitation for
heart failure. Cochrane Database Syst Rev 2004;CD003331.
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
to rheumatoid cachexia, as the mainstay of therapy here; the focus
of exercise should be to maintain a good level of musculoskeletal
system mobility and function with aerobic training for cardiovascular fitness instituted as soon as possible. In those with a lot of
inflammation and a lot of structural damage, pharmacological
therapy is equally important to the group above; the focus of
exercise should be initially maintenance and then improvement of
musculoskeletal system mobility and function, followed by
aerobic exercise within the patient’s physical and cardiovascular
limitations. Finally, in those with little inflammation but a lot of
structural damage, pharmacological therapy would be aimed at
maintaining control of inflammation; range of motion exercises
and resistance training could be utilized to optimize musculoskeletal system mobility and function, followed by addition of
aerobic exercise within the patient’s limitations, to improve their
cardiorespiratory fitness as much as possible. Patients with
extensive structural damage should initially utilize the nondamaged joints; load on damaged joints should happen progressively, with the intensity of exercise progressing from range of
motion exercises to low-load exercise. Sufficient pain relief will
need to be ensured throughout any exercise training programme.
�Exercise and rheumatoid arthritis
71 Scott DL, Wolman RL. Rest or exercise in inflammatory arthritis? Br J Hosp Med
1992;48:445–447.
72 Lineker SC, Bell MJ, Wilkins AL, Badley EM. Improvements following short term
home based physical therapy are maintained at one year in people with moderate to
severe rheumatoid arthritis. J Rheumatol 2001;28:165–8.
73 de Jong Z, Munneke M, Zwinderman AH et al. Is a long-term high-intensity exercise
program effective and safe in patients with rheumatoid arthritis? Results of a
randomized controlled trial. Arthritis Rheum 2003;48:2415–24.
74 Hakkinen A, Sokka T, Kotaniemi A et al. Dynamic strength training in patients with
early rheumatoid arthritis increases muscle strength but not bone mineral density.
J Rheumatol 1999;26:1257–63.
75 Hakkinen A, Sokka T, Kautiainen H, Kotaniemi A, Hannonen P. Sustained
maintenance of exercise induced muscle strength gains and normal bone mineral
density in patients with early rheumatoid arthritis: a 5 year follow up. Ann Rheum Dis
2004;63:910–6.
76 Hakkinen A. Effectiveness and safety of strength training in rheumatoid arthritis.
Curr Opin Rheumatol 2004;16:132–7.
77 Lyngberg KK, Ramsing BU, Nawrocki A, Harreby M, Danneskiold-Samsoe B. Safe
and effective isokinetic knee extension training in rheumatoid arthritis. Arthritis
Rheum 1994;37:623–8.
78 van Den Ende CH, Vliet Vlieland TP, Munneke M, Hazes JM. Dynamic
exercise therapy for rheumatoid arthritis. Cochrane Database Syst Rev
2000;CD000322.
79 Ekdahl C, Andersson SI, Moritz U, Svensson B. Dynamic versus static training in
patients with rheumatoid arthritis. Scand J Rheumatol 1990;19:17–26.
80 Ekdahl C, Ekman R, Petersson I, Svensson B. Dynamic training and circulating
neuropeptides in patients with rheumatoid arthritis: a comparative study with healthy
subjects. Int J Clin Pharmacol Res 1994;14:65–74.
81 Bearne LM, Scott DL, Hurley MV. Exercise can reverse quadriceps sensorimotor
dysfunction that is associated with rheumatoid arthritis without exacerbating
disease activity. Rheumatology 2002;41:157–66.
82 Bostrom C, Harms-Ringdahl K, Karreskog H, Nordemar R. Effects of static and
dynamic shoulder rotator exercises in women with rheumatoid arthritis: a
randomised comparison of impairment, disability, handicap, and health. Scand J
Rheumatol 1998;27:281–90.
83 Nordemar R, Ekblom B, Zachrisson L, Lundqvist K. Physical training in rheumatoid
arthritis: a controlled long-term study. I. Scand J Rheumatol 1981;10:17–23.
84 de Jong Z, Munneke M, Zwinderman AH et al. Long term high intensity exercise
and damage of small joints in rheumatoid arthritis. Ann Rheum Dis
2004;63:1399–405.
85 Stenstrom CH, Lindell B, Swanberg E, Swanberg P, Harms-Ringdahl K,
Nordemar R. Intensive dynamic training in water for rheumatoid arthritis functional
class II–a long-term study of effects. Scand J Rheumatol 1991;20:358–65.
86 Hansen TM, Hansen G, Langgaard AM, Rasmussen JO. Longterm physical training
in rheumatoid arthritis. A randomized trial with different training programs and
blinded observers. Scand J Rheumatol 1993;22:107–12.
87 Munneke M, de Jong Z, Zwinderman AH et al. Effect of a high-intensity weightbearing exercise program on radiologic damage progression of the large joints in
subgroups of patients with rheumatoid arthritis. Arthritis Rheum 2005;53:410–7.
88 Marcora SM, Lemmey AB, Maddison PJ. Can progressive resistance training
reverse cachexia in patients with rheumatoid arthritis? Results of a pilot study.
J Rheumatol 2005;32:1031–9.
89 Roubenoff R, Roubenoff RA, Cannon JG et al. Rheumatoid cachexia: cytokinedriven hypermetabolism accompanying reduced body cell mass in chronic
inflammation. J Clin Invest 1994;93:2379–86.
90 Walsmith J, Roubenoff R. Cachexia in rheumatoid arthritis. Int J Cardiol
2002;85:89–99.
91 Rall LC, Roubenoff R. Rheumatoid cachexia: metabolic abnormalities, mechanisms
and interventions. Rheumatology 2004;43:1219–23.
92 Metsios GS, Stavropoulos-Kalinoglou A, Koutedakis Y, Kitas GD. Rheumatoid
Cachexia: causes, significance and possible interventions. Hospital Chronicles
2006;1:20–6.
93 ACSM. American College of Sports Medicine Position Stand. The recommended
quantity and quality of exercise for developing and maintaining cardiorespiratory
and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc
1998;30:975–91.
94 Lyngberg KK, Harreby M, Bentzen H, Frost B, Danneskiold-Samsoe B. Elderly
rheumatoid arthritis patients on steroid treatment tolerate physical training without
an increase in disease activity. Arch Phys Med Rehabil 1994;75:1189–95.
95 Hakkinen A, Hakkinen K, Hannonen P. Effects of strength training on neuromuscular function and disease activity in patients with recent-onset inflammatory
arthritis. Scand J Rheumatol 1994;23:237–42.
96 Beals CA, Lampman RM, Banwell BF, Braunstein EM, Albers JW, Castor CW.
Measurement of exercise tolerance in patients with rheumatoid arthritis and
osteoarthritis. J Rheumatol 1985;12:458–61.
97 Westby MD. A health professional’s guide to exercise prescription for people with
arthritis: a review of aerobic fitness activities. Arthritis Rheum 2001;45:501–11.
98 Namey TC. Exercise and arthritis. Adaptive bicycling. Rheum Dis Clin North Am
1990;16:871–86.
99 Daltroy LH, Robb-Nicholson C, Iversen MD, Wright EA, Liang MH. Effectiveness of
minimally supervised home aerobic training in patients with systemic rheumatic
disease. Br J Rheumatol 1995;34:1064–9.
100 Ekblom B, Lovgren O, Alderin M, Fridstrom M, Satterstrom G. Effect of short-term
physical training on patients with rheumatoid arthritis I. Scand J Rheumatol
1975;4:80–6.
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
39 Mears S. The importance of exercise training in patients with chronic heart failure.
Nurs Stand 2006;20:41–7.
40 Ko JK, McKelvie RS. The role of exercise training for patients with heart failure. Eura
Medicophys 2005;41:35–47.
41 McGowan J. Evidence-based Rheumatology, Literature Searching. In: Tugwell P, ed.
London, UK: BMJ Publishing Group, 2005;3–18.
42 Jadad AR, Moore A, Carroll D et al. Assessing the quality of reports of randomised
clinical trials: is blinding necessary? Controlled Cl Trials 1996;17:1–12.
43 ACSM. ACSM’s Guidelines for Exercise Testing and Prescription. Seventh edn,
2005: Lippincott Williams & Wilkins, USA.
44 Bassuk SS, Manson JE. Physical activity and the prevention of cardiovascular
disease. Curr Atheroscler Rep 2003;5:299–307.
45 Farrell SW, Kampert JB, Kohl HW 3rd et al. Influences of cardiorespiratory fitness
levels and other predictors on cardiovascular disease mortality in men. Med Sci
Sports Exerc 1998;30:899–905.
46 Blair SN, Kampert JB, Kohl HW 3rd et al. Influences of cardiorespiratory fitness and
other precursors on cardiovascular disease and all-cause mortality in men and
women. JAMA 1996;276:205–10.
47 Eaton CB. Relation of physical activity and cardiovascular fitness to coronary heart
disease, Part II: Cardiovascular fitness and the safety and efficacy of physical activity
prescription. J Am Board Fam Pract 1992;5:157–65.
48 Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity
and mortality among men referred for exercise testing. N Engl J Med
2002;346:793–801.
49 Gibbons LW, Mitchell TL, Wei M, Blair SN, Cooper KH. Maximal exercise test as a
predictor of risk for mortality from coronary heart disease in asymptomatic men. Am J
Cardiol 2000;86:53–8.
50 Bouchard C, An P, Rice T et al. Familial aggregation of VO(2max) response to
exercise training: results from the HERITAGE Family Study. J Appl Physiol
1999;87:1003–8.
51 Skinner JS, Jaskolski A, Jaskolska A et al. Age, sex, race, initial fitness,
and response to training: the HERITAGE Family Study. J Appl Physiol
2001;90:1770–6.
52 Fletcher GF, Balady G, Blair SN et al. Statement on exercise: benefits and
recommendations for physical activity programs for all Americans. A statement for
health professionals by the Committee on Exercise and Cardiac Rehabilitation of the
Council on Clinical Cardiology, American Heart Association. Circulation
1996;94:857–62.
53 Bendermacher BL, Willigendael EM, Teijink JA, Prins MH. Supervised exercise
therapy versus non-supervised exercise therapy for intermittent claudication.
Cochrane Database Syst Rev 2006;CD005263.
54 Deforche B, De Bourdeaudhuij I. Differences in psychosocial determinants of
physical activity in older adults participating in organised versus non-organised
activities. J Sports Med Phys Fitness 2000;40:362–72.
55 Oguma Y, Shinoda-Tagawa T. Physical activity decreases cardiovascular disease
risk in women: review and meta-analysis. Am J Prev Med 2004;26:407–18.
56 Slentz CA, Aiken LB, Houmard JA et al. Inactivity, exercise, and visceral fat.
STRRIDE: a randomized, controlled study of exercise intensity and amount. J Appl
Physiol 2005;99:1613–8.
57 Kraus WE, Houmard JA, Duscha BD et al. Effects of the amount and intensity of
exercise on plasma lipoproteins. N Engl J Med 2002;347:1483–92.
58 Jakicic JM, Marcus BH, Gallagher KI, Napolitano M, Lang W. Effect of exercise
duration and intensity on weight loss in overweight, sedentary women: a randomized
trial. JAMA 2003;290:1323–30.
59 Duscha BD, Slentz CA, Johnson JL et al. Effects of exercise training amount and
intensity on peak oxygen consumption in middle-age men and women at risk for
cardiovascular disease. Chest 2005;128:2788–93.
60 Fletcher GF. The antiatherosclerotic effect of exercise and development of an
exercise prescription. Cardiol Clin 1996;14:85–95.
61 Gossard D, Haskell WL, Taylor CB et al. Effects of low- and high-intensity homebased exercise training on functional capacity in healthy middle-aged men. Am J
Cardiol 1986;57:446–9.
62 Crouse SF, O’Brien BC, Grandjean PW et al. Training intensity, blood lipids, and
apolipoproteins in men with high cholesterol. J Appl Physiol 1997;82:270–7.
63 O’Donovan G, Owen A, Bird SR et al. Changes in cardiorespiratory fitness and
coronary heart disease risk factors following 24 wk of moderate- or high-intensity
exercise of equal energy cost. J Appl Physiol 2005;98:1619–25.
64 Pescatello LS. Exercise and hypertension: recent advances in exercise prescription.
Curr Hypertens Rep 2005;7:281–6.
65 Pescatello LS, Guidry MA, Blanchard BE et al. Exercise intensity alters postexercise
hypotension. J Hypertens 2004;22:1881–8.
66 Mestek ML, Garner JC, Plaisance EP, Taylor JK, Alhassan S, Grandjean PW. Blood
lipid responses after continuous and accumulated aerobic exercise. Int J Sport Nutr
Exerc Metab 2006;16:245–54.
67 Pollock ML, Franklin BA, Balady GJ et al. AHA Science Advisory. Resistance
exercise in individuals with and without cardiovascular disease: benefits, rationale,
safety, and prescription: an advisory from the Committee on Exercise, Rehabilitation,
and Prevention, Council on Clinical Cardiology, American Heart Association;
Position paper endorsed by the American College of Sports Medicine. Circulation
2000;101:828–33.
68 Koutedakis Y, Metsios GS, Stavropoulos-Kalinoglou A. Periodisation of exercise
training in Sport. In: Whyte G, ed. The physiology of training, Philadelphia: Churchill
Livingstone, Elsevier, 2006:1–21.
69 Lee DM, Weinblatt ME. Rheumatoid arthritis. Lancet 2001;358:903–11.
70 Ekdahl C, Broman G. Muscle strength, endurance, and aerobic capacity in rheumatoid
arthritis: a comparative study with healthy subjects. Ann Rheum Dis 1992;51:35–40.
247
�248
G. S. Metsios et al.
131 ACR. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis
Rheum 2002;46:328–46.
132 Nordemar R, Berg U, Ekblom B, Edstrom L. Changes in muscle fibre size and
physical performance in patients with rheumatoid arthritis after 7 months physical
training. Scand J Rheumatol 1976;5:233–8.
133 Stenstrom CH. Home exercise in rheumatoid arthritis functional class II: goal setting
versus pain attention. J Rheumatol 1994;21:627–34.
134 Komatireddy GR, Leitch RW, Cella K, Browning G, Minor M. Efficacy of low load
resistive muscle training in patients with rheumatoid arthritis functional class II and
III. J Rheumatol 1997;24:1531–9.
135 Hakkinen A, Sokka T, Kotaniemi A, Hannonen P. A randomized two-year study of
the effects of dynamic strength training on muscle strength, disease activity,
functional capacity, and bone mineral density in early rheumatoid arthritis. Arthritis
Rheum 2001;44:515–22.
136 Hakkinen A, Sokka T, Lietsalmi AM, Kautiainen H, Hannonen P. Effects of dynamic
strength training on physical function, Valpar 9 work sample test, and working
capacity in patients with recent-onset rheumatoid arthritis. Arthritis Rheum
2003;49:71–7.
137 Hakkinen A, Hannonen P, Nyman K, Lyyski T, Hakkinen K. Effects of
concurrent strength and endurance training in women with early or longstanding
rheumatoid arthritis: comparison with healthy subjects. Arthritis Rheum
2003;49:789–97.
138 de Jong Z, Munneke M, Lems WF et al. Slowing of bone loss in patients with
rheumatoid arthritis by long-term high-intensity exercise: results of a randomized,
controlled trial. Arthritis Rheum 2004;50:1066–76.
139 Kettunen JA, Kujala UM. Exercise therapy for people with rheumatoid arthritis and
osteoarthritis. Scand J Med Sci Sports 2004;14:138–42.
140 April KT, Feldman DE, Platt RW, Duffy CM. Comparison between children with
juvenile idiopathic arthritis and their parents concerning perceived treatment
adherence. Arthritis Rheum 2006;55:558–63.
141 Brus HL, Taal E, van de Laar MA, Rasker JJ, Wiegman O. Patient education and
disease activity: a study among rheumatoid arthritis patients. Arthritis Care Res
1997;10:320–4.
142 Brus HL, van de Laar MA, Taal E, Rasker JJ, Wiegman O. Effects of patient
education on compliance with basic treatment regimens and health in recent onset
active rheumatoid arthritis. Ann Rheum Dis 1998;57:146–51.
143 Carpenter JO, Davis LJ. Medical recommendations–followed or ignored? Factors
influencing compliance in arthritis. Arch Phys Med Rehabil 1976;57:241–6.
144 Mahowald ML, Steveken ME, Young M, Ytterberg SR. The Minnesota Arthritis
Training Program: emphasis on self-management, not compliance. Patient Educ
Couns 1988;11:235–41.
145 Minor MA, Brown JD. Exercise maintenance of persons with arthritis after
participation in a class experience. Health Educ Q 1993;20:83–95.
146 Neuberger GB, Smith KV, Black SO, Hassanein R. Promoting self-care in clients
with arthritis. Arthritis Care Res 1993;6:141–8.
147 Rapoff MA, Lindsley CB, Christophersen ER. Parent perceptions of problems
experienced by their children in complying with treatments for juvenile rheumatoid
arthritis. Arch Phys Med Rehabil 1985;66:427–9.
148 Stenstrom CH, Arge B, Sundbom A. Home exercise and compliance in inflammatory
rheumatic diseases–a prospective clinical trial. J Rheumatol 1997;24:470–6.
149 Bradley LA. Adherence with treatment regimens among adult rheumatoid
arthritis patients: current status and future directions. Arthritis Care Res
1989;2:S33–9.
150 Brus H, van de Laar M, Taal E, Rasker J, Wiegman O. Compliance in rheumatoid
arthritis and the role of formal patient education. Semin Arthritis Rheum
1997;26:702–10.
151 Crofford LJ, Appleton BE. Complementary and alternative therapies for fibromyalgia. Curr Rheumatol Rep 2001;3:147–56.
152 Hawley DJ. Psycho-educational interventions in the treatment of arthritis. Baillieres
Clin Rheumatol 1995;9:803–23.
153 O’Grady M, Fletcher J, Ortiz S. Therapeutic and physical fitness exercise
prescription for older adults with joint disease: an evidence-based approach.
Rheum Dis Clin North Am 2000;26:617–46.
154 Ottawa Panel. Ottawa Panel evidence-based clinical practice guidelines for
therapeutic exercises in the management of rheumatoid arthritis in adults. Phys
Ther 2004;84:934–72.
155 Rapoff MA. Assessing and enhancing adherence to medical regimens for juvenile
rheumatoid arthritis. Pediatr Ann 2002;31:373–9.
156 Schrieber L, Colley M. Patient education. Best Pract. Res Clin Rheumatol
2004;18:465–76.
157 Swezey RL, Swezey AM. The physician and the arthritis patient: informed partners
in therapy. Postgrad Med 1983; Spec No: 57–63.
158 Zinna EM, Yarasheski KE. Exercise treatment to counteract protein wasting of
chronic diseases. Curr Opin Clin Nutr Metab Care 2003;6:87–93.
159 Waggoner CD, LeLieuvre RB. A method to increase compliance to exercise
regimens in rheumatoid arthritis patients. J Behav Med 1981;4:191–201.
160 Munneke M, de Jong Z, Zwinderman AH et al. Adherence and satisfaction of
rheumatoid arthritis patients with a long-term intensive dynamic exercise program
(RAPIT program). Arthritis Rheum 2003;49:665–72.
161 Hale ED, Treharne GJ, Kitas GD. The Common-sense model of self-regulation of
health and illness: how can we use it to understand and respond to our patients’
needs? Rheumatology 2007;46:944–51.
162 John H, Hale ED, Treharne GJ, Kitas GD. Patient education on cardiovascular
aspects of rheumatoid disease: An unmet need. Rheumatology 2007;46:1513–16.
Downloaded from https://academic.oup.com/rheumatology/article/47/3/239/1774371 by guest on 04 June 2022
101 Ekblom B, Lovgren O, Alderin M, Fridstrom M, Satterstrom G. Effect of short-term
physical training on patients with rheumatoid arthritis. a six-month follow-up study.
Scand J Rheumatol 1975;4:87–91.
102 Harkcom TM, Lampman RM, Banwell BF, Castor CW. Therapeutic value of
graded aerobic exercise training in rheumatoid arthritis. Arthritis Rheum
1985;28:32–9.
103 Karper WB, Evans BW. Cycling program effects on one rheumatoid arthritic. Am J
Phys Med 1986;65:167–72.
104 Lyngberg K, Danneskiold-Samsoe B, Halskov O. The effect of physical training on
patients with rheumatoid arthritis: changes in disease activity, muscle strength and
aerobic capacity. A clinically controlled minimized cross-over study. Clin Exp
Rheumatol 1988;6:253–60.
105 Baslund B, Lyngberg K, Andersen V et al. Effect of 8 wk of bicycle training on the
immune system of patients with rheumatoid arthritis. J Appl Physiol 1993;75:1691–5.
106 Melton-Rogers S, Hunter G, Walter J, Harrison P. Cardiorespiratory responses of
patients with rheumatoid arthritis during bicycle riding and running in water. Phys
Ther 1996;76:1058–65.
107 Bilberg A, Ahlmen M, Mannerkorpi K. Moderately intensive exercise in a temperate
pool for patients with rheumatoid arthritis: a randomized controlled study.
Rheumatology 2005;44:502–8.
108 Minor MA, Hewett JE, Webel RR, Anderson SK, Kay DR. Efficacy of physical
conditioning exercise in patients with rheumatoid arthritis and osteoarthritis. Arthritis
Rheum 1989;32:1396–405.
109 Hall J, Skevington SM, Maddison PJ, Chapman K. A randomized and controlled
trial of hydrotherapy in rheumatoid arthritis. Arthritis Care Res 1996;9:206–15.
110 Suomi R, Collier D. Effects of arthritis exercise programs on functional fitness and
perceived activities of daily living measures in older adults with arthritis. Arch Phys
Med Rehabil 2003;84:1589–94.
111 Sanford-Smith S, Mackay-Lyons M, Nunes-Clement S. Therapeutic benefit of
aquaerobics for individuals with Rheumatoid Arthritis. Physiother Canada
1998;50:40–6.
112 Danneskiold-Samsoe B, Lyngberg K, Risum T, Telling M. The effect of water
exercise therapy given to patients with rheumatoid arthritis. Scand J Rehabil Med
1987;19:31–5.
113 Minor MA, Hewett JE. Physical fitness and work capacity in women with rheumatoid
arthritis. Arthritis Care Res 1995;8:146–54.
114 Rintala P, Kettunen H, McCubbin JA. Effects of water exercise program for
individuals with rheumatoid arthritis. Sports Med Training Rehabil 1996;7:31–8.
115 Noreau L, Martineau H, Roy L, Belzile M. Effects of a modified dance-based
exercise on cardiorespiratory fitness, psychological state and health status of
persons with rheumatoid arthritis. Am J Phys Med Rehabil 1995;74:19–27.
116 Noreau L, Moffet H, Drolet M, Parent E. Dance-based exercise program in
rheumatoid arthritis. Feasibility in individuals with American College of
Rheumatology functional class III disease. Am J Phys Med Rehabil 1997;76:109–13.
117 Neuberger GB, Press AN, Lindsley HB et al. Effects of exercise on fatigue, aerobic
fitness, and disease activity measures in persons with rheumatoid arthritis. Res
Nurs Health 1997;20:195–204.
118 Perlman SG, Connell KJ, Clark A et al. Dance-based aerobic exercise for
rheumatoid arthritis. Arthritis Care Res 1990;3:29–35.
119 Westby MD, Wade JP, Rangno KK, Berkowitz J. A randomized controlled trial to
evaluate the effectiveness of an exercise program in women with rheumatoid
arthritis taking low dose prednisone. J Rheumatol 2000;27:1674–80.
120 Moffet H, Noreau L, Parent E, Drolet M. Feasibility of an eight-week dance-based
exercise program and its effects on locomotor ability of persons with functional class
III rheumatoid arthritis. Arthritis Care Res 2000;13:100–11.
121 Melikoglu MA, Karatay S, Senel K, Akcay F. Association between dynamic exercise
therapy and IGF-1 and IGFBP-3 concentrations in the patients with rheumatoid
arthritis. Rheumatol Int 2006;26:309–13.
122 Allen SH, Minor MA, Hillman LS, Kay DR. Effect of exercise on the bone mineral
density and bone remodelling indices in women with rheumatoid arthritis: 2 case
studies. J Rheumatol 1993;20:1247–9.
123 Keenan MA, Peabody TD, Gronley JK, Perry J. Valgus deformities of the feet and
characteristics of gait in patients who have rheumatoid arthritis. J Bone Joint Surg
Am 1991;73:237–47.
124 Platto MJ, O’Connell PG, Hicks JE, Gerber LH. The relationship of pain and
deformity of the rheumatoid foot to gait and an index of functional ambulation.
J Rheumatol 1991;18:38–43.
125 Fransen M, Edmonds J. Off-the-shelf orthopedic footwear for people with
rheumatoid arthritis. Arthritis Care Res 1997;10:250–6.
126 Hakkinen A, Pakarinen A, Hannonen P et al. Effects of prolonged combined
strength and endurance training on physical fitness, body composition and serum
hormones in women with rheumatoid arthritis and in healthy controls. Clin Exp
Rheumatol 2005;23:505–12.
127 Macsween A, Johnson NJ, Armstrong G, Bonn J. A validation of the 10-meter
incremental shuttle walk test as a measure of aerobic power in cardiac and
rheumatoid arthritis patients. Arch Phys Med Rehabil 2001;82:807–10.
128 Bluestone R. A marathon runner with high fever, arthralgia. Hosp Pract (Off Ed)
1983;18:114–9.
129 van den Ende CH, Hazes JM, le Cessie S et al. Comparison of high and low
intensity training in well controlled rheumatoid arthritis. Results of a randomised
clinical trial. Ann Rheum Dis 1996;55:798–805.
130 van den Ende CH, Breedveld FC, le Cessie S, Dijkmans BA, de Mug AW,
Hazes JM. Effect of intensive exercise on patients with active rheumatoid arthritis: a
randomised clinical trial. Ann Rheum Dis 2000;59:615–21.
�Please excuse the presence of this and the
following test pages, which have been
added to a small number of article PDFs for
a limited time as part of our process of
continual development and improvement.
academic.oup.com/cid
academic.oup.com/rheumatology
1 of 4
�Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod
tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim
veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea
commodo consequat. Duis aute irure dolor in reprehenderit in voluptate
velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat
cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id
est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed
do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim
ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip
ex ea commodo consequat. Duis aute irure dolor in reprehenderit in
voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint
occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit
anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing
elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi
ut aliquip ex ea commodo consequat. Duis aute irure dolor in
reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur.
Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia
deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet,
consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et
dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation
ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure
dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla
pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa
qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit
amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut
labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud
exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.
Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore
eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident,
sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem
ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor
incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam,
quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo
consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse
cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat
non proident, sunt in culpa qui officia deserunt mollit anim id est
laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do
academic.oup.com/cid
2 of 4
�eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad
minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex
ea commodo consequat. Duis aute irure dolor in reprehenderit in
voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint
occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit
anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing
elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi
ut aliquip ex ea commodo consequat. Duis aute irure dolor in
reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur.
Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia
deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet,
consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et
dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation
ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure
dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla
pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa
qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit
amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut
labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud
exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.
Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore
eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident,
sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem
ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor
incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam,
quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo
consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse
cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat
non proident, sunt in culpa qui officia deserunt mollit anim id est
laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do
eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad
minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex
ea commodo consequat. Duis aute irure dolor in reprehenderit in
voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint
occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit
anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing
elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
academic.oup.com/cid
3 of 4
�Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi
ut aliquip ex ea commodo consequat. Duis aute irure dolor in
reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur.
Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia
deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet,
consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et
dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation
ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure
dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla
pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa
qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit
amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut
labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud
exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.
Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore
eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident,
sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem
ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor
incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam,
quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo
consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse
cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat
non proident, sunt in culpa qui officia deserunt mollit anim id est
laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do
eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad
minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex
ea commodo consequat. Duis aute irure dolor in reprehenderit in
voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint
occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit
anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing
elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi
ut aliquip ex ea commodo consequat. Duis aute irure dolor in
reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur.
Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia
deserunt mollit anim id est laborum.
academic.oup.com/cid
4 of 4
�
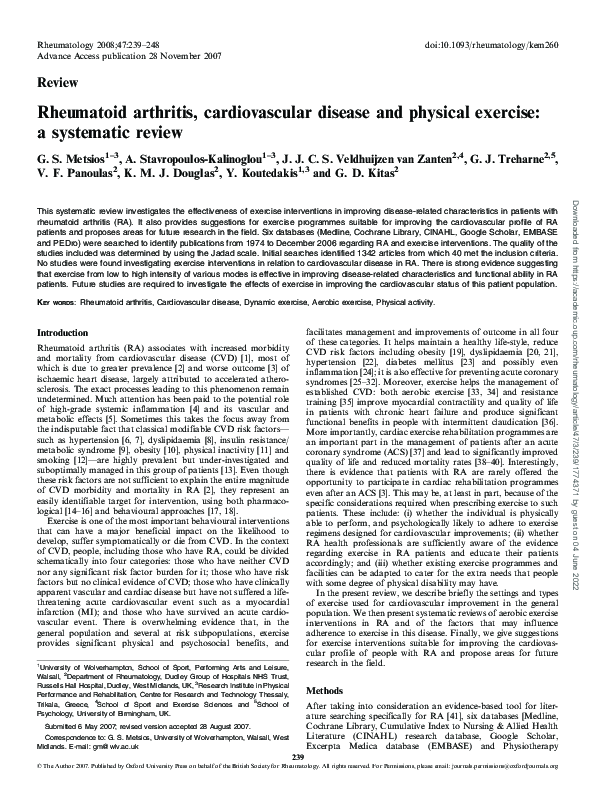
 Yiannis Koutedakis
Yiannis Koutedakis