Regulatory Peptides 135 (2006) 39 – 44
www.elsevier.com/locate/regpep
Hypothalamic cardiovascular effects of angiotensin-(1–7)
in spontaneously hypertensive rats
Christian Höcht a,⁎, Javier A.W. Opezzo a , Mariela M. Gironacci b ,
Clara Peña b , Carlos A. Taira a
a
Departamento de Farmacología, Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Junín 956, (C1113AAD) Buenos Aires, Argentina
b
Departamento de Química Biológica e Instituto de Química y Fisicoquímica Biológicas, Facultad de Farmacia y Bioquímica,
Universidad de Buenos Aires, Buenos Aires, Argentina
Received 20 July 2005; received in revised form 20 March 2006; accepted 24 March 2006
Available online 5 May 2006
Abstract
The objective of the present work was to study the cardiovascular actions of the intrahypothalamic injection of Ang-(1–7) and its effects on the
pressor response to Ang II in spontaneously hypertensive (SH) rats and Wistar Kyoto (WKY) animals. In anaesthetized SH and WKY rats, a carotid
artery was cannulated for mean arterial pressure (MAP) measurement and a stainless-steel needle was inserted into the anterior hypothalamus for drug
administration. The cardiovascular effects of the intrahypothalamic administration of Ang-(1–7) were determined in SH and WKY rats. In SH rats,
the effect of irbesartan and D-Ala-Ang-(1–7) on Ang-(1–7) cardiovascular effect was also evaluated. Ang II was administered in the hypothalamus of
SH and WKY rats and changes in blood pressure and heart rate were measured followed by the administration of Ang II, Ang II + Ang-(1–7) or Ang
II + D-Ala-Ang-(1–7). Ang-(1–7) did not the change basal MAP in WKY rats, but induced a pressor response in SH animals. Whilst the coadministration of D-Ala-Ang-(1–7) did not affect the response to Ang-(1–7), the previous administration of irbesartan prevented the effect of the
peptide. The intrahypothalamic injection of Ang II induced a significantly greater pressor response in SH animals compared to normotensive rats. The
co-administration of Ang-(1–7) with Ang II did not affect the pressor response to Ang II in the WKY group. In SH rats, whilst the co-administration of
Ang-(1–7) with Ang II reduced the pressor response to Ang II, the concomitant application of D-Ala-Ang-(1–7) with Ang II increased the pressor
response to the octapeptide after 5 and 10 min of intrahypothalamic administration. In conclusion, our result demonstrated that the biologically active
peptide Ang-(1–7) did not participate in the hypothalamic blood pressure regulation of WKY animals. In SH rats, Ang-(1–7) exerted pleiotropic
effects on blood pressure regulation. High dose of the heptapeptide produced a pressor response because of an unspecific action by activation of AT1
receptors. The concomitant administration of lower doses of Ang-(1–7) with Ang II reduced the pressor response to the octapeptide. Finally, the effect
of AT1–7 antagonist on Ang II pressor response suggested that hypothalamic formed Ang-(1–7) are implicated in the regulation of the cardiovascular
effects of Ang II.
© 2006 Elsevier B.V. All rights reserved.
Keywords: Angiotensin II; Angiotensin-(1–7); Spontaneously hypertensive rats; Anterior hypothalamus; AT1 receptor; AT1–7 receptor; Cardiovascular effect
1. Introduction
Most forms of experimental hypertension are associated with
a wide variety of functional changes in the hypothalamus [1].
The hypertensive state appears to be due to an increase in
medullar pressor activity due to suppression from supramedullary sources [2,3]. The medulla's excitatory center is under the
influence of the hypothalamus, the midbrain, a medullar inhib⁎ Corresponding author. Tel.: +54 11 4964 8265; fax: +54 11 4508 3645.
E-mail address: chocht@ffyb.uba.ar (C. Höcht).
0167-0115/$ - see front matter © 2006 Elsevier B.V. All rights reserved.
doi:10.1016/j.regpep.2006.03.007
itor center slightly more caudal than the excitatory center, and
the nucleus tractus solitarius [2,4].
A pressor increase in hypothalamic angiotensin activity was
shown in spontaneously hypertensive (SH) rats [5], Dahl-S rats
[6], renal hypertension [7] and DOCA-salt hypertension [8]. In
addition, there would appear to be a function interlocking of
catecholamines and angiotensin II (Ang II) in the hypothalamus
[1]. The mechanism by which Ang II regulates blood pressure
involves, at least in part, brain catecholamine pathways [9]. In
various brain nuclei relevant to cardiovascular control, AT1 receptor activation regulates the uptake, synthesis and release of
�C. Höcht et al. / Regulatory Peptides 135 (2006) 39–44
2. Materials and methods
Eight-weeks old male spontaneously hypertensive (SH) and
Wistar Kyoto (WKY) rats were used. Animal experiments were
performed in accordance with the Principles of Laboratory
Animal Care (NIH publication no. 85-23, revised 1985).
On the day of the experiment, rats were anaesthetized with a
mix of chloralose (50 mg kg− 1, i.p.) and urethane (500 mg kg− 1,
i.p.). A carotid artery was cannulated and connected to a Statham
P23ID pressure transducer (Gould Instruments, Cleveland, OH,
USA) coupled to a Grass 79D polygraph (Grass Instrument Co.,
Quincy, MA, USA). Mean arterial pressure (MAP) was calculated according to the formula diastolic pressure + (systolic
pressure − diastolic pressure) / 3. The heart rate (HR) was
calculated by means of a tachograph by counting the pulsatile
waves of arterial pressure recording.
A 32 gauge stainless-steel needle was inserted into the anterior hypothalamus according to the stereotaxic coordinates A/P
− 1.5 mm, L/M − 0.6 mm, V/D 9.0 mm, from the bregma [20].
All drugs were dissolved in Ringer's solution and 0.5 μL
solution was injected at a rate of 1 μL/min in the anterior hypothalamic area.
A stabilization period of 30 min preceded drug administration and changes in blood pressure were determined.
At the end of the experiment, the position of the needle was
verified by histology.
2.1. Experiment 1
In SH rats (n = 15), the cardiovascular effects of the intrahypothalamic administration of Ang-(1–7) (50 and 250 ng)
were determined with a stabilization period of 30 min between
both doses. After recovery of basal blood pressure values and a
stabilization period of 30 min, the rats were divided in 3 groups.
In 10 rats, Ringer's solution was administered into the anterior
hypothalamus followed, 10 min later, by an injection of Ang(1–7) (250 ng, n = 5) or Ang-(1–7) (250 ng) + D-Ala-Ang-(1–7)
(AT1–7 receptor antagonist, 250 ng) (n = 5). In the third group,
irbesartan (AT1-receptor antagonist; 250 ng; n = 5) dissolved in
Ringer solution was injected in the anterior hypothalamus. Ang(1–7) (250 ng) was re-administered 10 min later by intrahypothalamic administration.
In WKY rats the cardiovascular effects of the intrahypothalamic administration of Ang-(1–7) (50 and 250 ng, n = 5) were
determined separated by a stabilization period of 30 min.
2.2. Experiment 2
In a second set of experiments, Ang II (50 ng, n = 15) was
administered in the anterior hypothalamic area of SH rats and
changes in blood pressure and heart rate were measured. After
the recovery of basal blood pressure values, and a stabilization
A
∆ MAP (mmHg)
noradrenaline and dopamine [10,11]. Moreover, an increase in
catecholamine turnover was observed after the activation of the
high density Ang II receptors in the hypothalamus [9].
In the last decade, new biologically active components of
the renin–angiotensin system (RAS) were found. Angiotensin(1–7) (Ang-(1–7)), a metabolite of Ang II, is considered the
most pleiotropic component of the RAS [12]. Ang-(1–7) lacks
the pressor, dipsogenic and an aldosterone secretory action elicited by Ang II, but this heptapeptide increased vasopressin release,
prostaglandin synthesis and facilitates peripheral noradrenergic
neurotransmission in the same manner as Ang II [12–14].
Ang-(1–7) is also generated in the brain, especially in the
central nuclei related to blood pressure regulation such as the
medullary areas and the hypothalamus [12]. Intracerebroventricular administration of the peptide did not modify blood pressure and heart rate but produced facilitation of the baroreceptor
reflex control of heart rate [15]. On the other hand, Ang-(1–7)
inhibited the release of noradrenaline induced by Ang II in
hypothalamic nuclei [16]. However, to the best our knowledge,
studies of the cardiovascular effects of the administration of
Ang-(1–7) in the anterior hypothalamus are lacking.
Several studies have shown that the Ang-(1–7) opposite
effect to Ang II is enhanced in animal models of hypertension
[17,18]. Benter et al. [19] have demonstrated that Ang-(1–7)
attenuates Ang II vasoconstriction in SH rats but not in normotensive animals.
The aim of the present work was to study the cardiovascular
actions of the intrahypothalamic injection of Ang-(1–7) and the
effects of the heptapeptide on the pressor response to Ang II in
SH rats and time matched Wistar Kyoto (WKY) animals.
15
10
5
0
-5
-10
0
5
10
15
20
25
30
35
25
30
35
Time (min)
B
∆ MAP (mmHg)
40
15
**
10
*
5
0
-5
-10
0
5
10
15
20
Time (min)
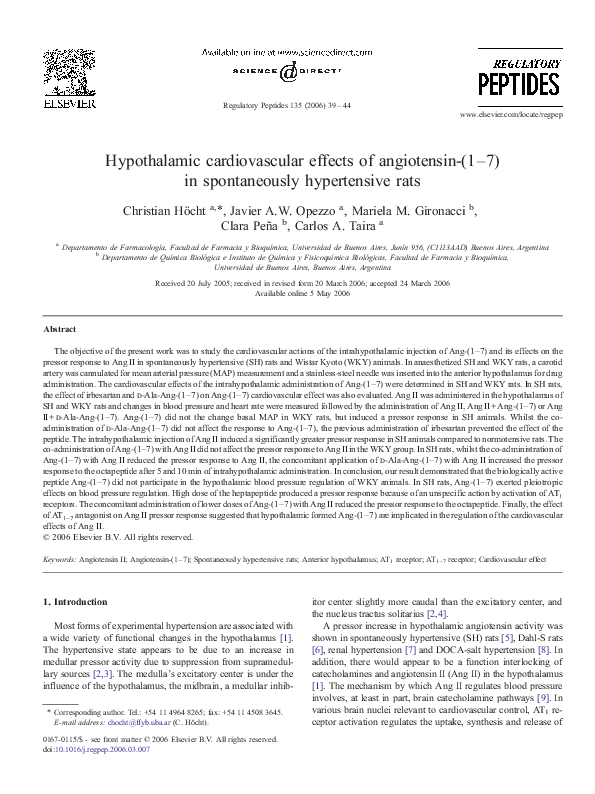
Fig. 1. Change in the mean arterial pressure (ΔMAP), after injection of 50 ng
(circles) and 250 ng (squares) of angiotensin-(1–7) in the anterior hypothalamic
area of Wistar Kyoto (WKY) animals (in A) and spontaneously hypertensive
(SH) rats (in B). Each point shows the mean ± SEM of fifteen animals. *p b 0.05
vs. Ang-(1–7) (50 ng).
�41
C. Höcht et al. / Regulatory Peptides 135 (2006) 39–44
A
after the recovery of basal blood pressure values and a stabilization period of 30 min.
15
∆ MAP (mmHg)
10
2.3. Experiment 3
5
Finally, the cardiovascular response to the intrahypothalamic
administration of D-Ala-Ang-(1–7) (250 ng) (n = 5) was evaluated in SH rats.
0
-5
2.4. Statistics
-10
0
5
10
15
20
25
30
35
Time (min)
B
15
∆ MAP (mmHg)
10
5
The normal distribution of the variables was verified using
the Kolmogorov–Smirnov (K–S) test. Data are expressed as the
mean ± SEM. Statistical analyses were performed by unpaired
Student's t test [21] or two-way ANOVA for repeated measure
followed by the Bonferroni test as a post hoc test. Statistical tests
were performed using GraphPad Prism version 3.02 for
Windows (GraphPad Software, San Diego, CA, USA). Statistical significance was defined as p b 0.05.
0
2.5. Drugs
-5
The following drugs were used: Angiotensin II (Sigma, St
Louis, MO, USA), Irbesartan (a generous gift from Sanofi,
-10
0
5
10
15
20
25
30
35
Time (min)
A
15
15
10
10
∆ MAP (mmHg)
∆ MAP (mmHg)
C
*
5
*
0
*
*
5
0
-5
-5
-10
5
10
15
20
25
30
0
35
Time (min)
Fig. 2. In A: change in mean arterial pressure (ΔMAP) in SH rats after injection
of angiotensin-(1–7) (250 ng) without pretreatment (circles) and after
pretreatment (squares) with saline solution. In B: after injection of angiotensin-(1–7) (250 ng) without pretreatment (circles) and after injection of
angiotensin-(1–7) (250 ng) + D-Ala-angiotensin-(1–7) (250 ng) after pretreatment with saline solution (250 ng) (squares). In C: after injection of angiotensin(1–7) (250 ng) without pretreatment (circles) and after pretreatment (squares)
with irbesartan. Each point shows the mean ± SEM of five animals. *p b 0.05 vs.
angiotensin-(1–7) without pretreatment.
period of 30 min, SH rats were divided in 3 groups, each group
receiving Ang II (50 ng, n = 5), Ang II (50 ng) + Ang-(1–7)
(50 ng) (n = 5) or Ang II (50 ng) + D-Ala-Ang-(1–7) (250 ng)
(n = 5) into the anterior hypothalamus. The cardiovascular
effects were recorded for a period of 30 min.
In WKY rats, Ang II (50 ng, n = 10) was administered in the
anterior hypothalamic area, followed by the administration of
Ang II (50 ng, n = 5) or Ang II (50 ng) + Ang-(1–7) (50 ng) (n = 5)
5
10
15
20
25
30
35
25
30
35
Time (min)
B
∆ MAP (mmHg)
0
15
10
5
0
-5
0
5
10
15
20
Time (min)
Fig. 3. Change in mean arterial pressure (ΔMAP), after injection of angiotensin
II (50 ng) (circles) and after second injection of angiotensin II (50 ng) (squares;
in A) or angiotensin II (50 ng) + angiotensin-(1–7) (50 ng) (squares; in B) in the
anterior hypothalamic area of Wistar Kyoto (WKY) animals. Each point shows
the mean ± SEM of five animals.
�42
C. Höcht et al. / Regulatory Peptides 135 (2006) 39–44
France). Angiotensin-(1–7) and D-Ala-Angiotensin-(1–7) were
synthesized by the Department of Biochemistry, Faculty of
Pharmacy and Biochemistry, University of Buenos Aires.
3. Results
The basal values of MAP and heart rate (HR) were 81 ±
5 mmHg and 410 ± 7 bpm (n = 35), respectively, in anaesthetized
WKY animals and 137 ± 6 mmHg (p b 0.05 vs. WKY rats) and
A
∆ MAP (mmHg)
30
20
*
10
0
0
5
10
15
20
25
30
35
25
30
35
Time (min)
∆ MAP (mmHg)
B
30
20
*
*
10
*
0
0
∆ MAP (mmHg)
C
5
10
15
20
Time (min)
30
20
4. Discussion
*
*
10
0
0
5
439 ± 6 bpm (p b 0.05 vs. WKY rats) (n = 15), respectively, in
anaesthetized SH rats.
The intrahypothalamic administration of Ang-(1–7) did not
change the basal blood pressure in WKY rats (Fig. 1A); however, the greatest dose of the heptapeptide induced a pressor
response in the hypertensive group (ΔMAP = 12.2 ± 0.6, n = 15,
p b 0.05 vs. WKY rats) (Fig. 1B). The intrahypothalamic administration of irbesartan reduced the basal blood pressure in SH rats
(ΔMAP = − 9.4 ± 1.6, n = 5). Whilst the co-administration of DAla-Ang-(1–7) did not affect the pressor effect of Ang-(1–7)
(ΔMAP = 10.6 ± 0.4, n = 5) (Fig. 2B), the previous administration of irbesartan prevented the effect of the peptide (ΔMAP =
1.1 ± 0.8, n = 5, p b 0.05 vs. Ang-(1–7) administration) (Fig. 2C).
On the other hand, the previous administration of Ringer
solution did not affect the blood pressure response to Ang-(1–7)
(ΔMAP = 11.8 ± 0.8, n = 5) (Fig. 2A). Intrahypothalamic administration of Ringer solution did not change basal MAP in SH rats.
The injection of Ang II in the anterior hypothalamic area
of WKY and SH rats induced a pressor response (Figs. 3
and 4), but the same was significantly greater in SH animals
(ΔMAP = 20.5 ±1.9, n = 15, p b 0.05 vs. WKY rats) as compared
to normotensive rats (ΔMAP = 9.6 ± 1.0, n = 10). The coadministration of Ang-(1–7) with Ang II did not affect the
pressor response to Ang II in the WKY group (ΔMAP = 9.4 ± 0.7,
n = 5) (Fig. 3B). On the other hand, the blood pressure response to
Ang II did not change by further administration of the peptide in
normotensive animals (ΔMAP = 9.2 ± 1.3, n = 5) (Fig. 3A).
The intrahypothalamic administration of D-Ala-Ang-(1–7)
did not modify the basal blood pressure in SH rats.
In SH rats, whilst the co-administration of Ang-(1–7) with
Ang II reduced the pressor response to Ang II (ΔMAP = 12.9 ±
1.7, n = 5, p b 0.05 vs. Ang II administration) (Fig. 4B), the concomitant application of D-Ala-Ang-(1–7) with Ang II increased
the pressor response to the octapeptide after 5 and 10 min of
intrahypothalamic administration (Fig. 4C). The blood pressure
response to Ang II did not change by further administration of
the peptide in SH animals (Fig. 4A).
In all experiments, the tested drugs did not modify the heart
rate of WKY and SH rats (data not shown).
10
15
20
25
30
35
Time (min)
Fig. 4. Change in mean arterial pressure (ΔMAP), after the injection of
angiotensin II (50 ng) (circles) and after second injection of angiotensin II
(50 ng) (squares; in A) or angiotensin II (50 ng) + angiotensin-(1–7) (50 ng)
(squares; in B) or angiotensin II + D-Ala-angiotensin-(1–7) (250 ng) (squares; in
B) or angiotensin II + D-Ala-angiotensin-(1–7) (250 ng) (squares; in C) in the
anterior hypothalamic area of spontaneously hypertensive (SH) rats. Each point
shows the mean ± SEM of five animals. *p b 0.05 vs. angiotensin II without
pretreatment.
In the present study, the effects of intrahypothalamic administration of Ang II and Ang-(1–7) on blood pressure were investigated in anaesthetized SH and WKY rats. It is well known
that anaesthesia influences central blood pressure regulation and
could impact on the results of the present study [22]. However,
the pressor response to intrahypothalamic application of Ang II
in anaesthetized WKY and SH rats observed in the present study
is similar to that observed in conscious normotensive and spontaneously hypertensive animals [23]. So, it seems that the anaesthetic used in the present study did not affect the cardiovascular
response to Ang II.
There is an increasing body of evidence of a compromised
hypothalamic angiotensinergic mechanism in the pathophysiology of hypertension in a diverse range of animal experimental
models [1]. Kubo et al. [23] found a greater pressor response to
�C. Höcht et al. / Regulatory Peptides 135 (2006) 39–44
anterior hypothalamic Ang II injection in SH rats than in normotensive rats. The existence of a hypothalamic angiotensinergic
compromise in SH rats was also demonstrated with the application of angiotensin-converting enzyme inhibitors or angiotensin
receptor antagonist [5,23]. However, studies about the compromise of other bioactive peptides of the hypothalamic renin–
angiotensin system on blood pressure regulation are lacking.
Ang-(1–7) is considered the most pleiotropic component of
the RAS. The heptapeptide is generated in the brain, especially
in central nuclei related to blood pressure regulation such as
medullary areas and the hypothalamus [12]. Intracerebroventricular administration of Ang-(1–7) did not modify blood pressure and heart rate but produced facilitation of the baroreceptor
reflex control of heart rate [15]. On the other hand, Ang-(1–7)
inhibited the release of noradrenaline induced by Ang II in hypothalamic nuclei [16]. However, to the best our knowledge,
studies of the cardiovascular effect of administration of Ang-(1–
7) in the anterior hypothalamus are lacking.
In the present study the intrahypothalamic administration of
Ang-(1–7) did not change basal blood pressure in WKY
normotensive animals, but increased the same in SH hypertensive animals. Taking into account that Ang-(1–7) not only acts
as an agonist on AT1–7 receptors but also activates AT receptors
[24,25], we also studied the receptor involucrate in the pressor
response to the heptapeptide. For this purpose, one group of SH
rats was treated with irbesartan 10 min before Ang-(1–7)
second administration. Kubo et al. [23] have demonstrated that
the intrahypothalamic administration of irbesartan induced a
hypotensive effect in SH animals reaching the maximal effect at
10 min after drug administration. In our experiments the
administration of irbesartan also induced a decrease of blood
pressure in hypertensive animals. For the study of the
participation of AT1–7 receptors in Ang-(1–7) pressor response,
the antagonist, D-Ala-Ang-(1–7) was concomitantly administered with Ang II. The reason for this experimental design is that
a rapid degradation of the antagonist is expected because of its
peptidergic nature. On the other hand, the administration of DAla-Ang-(1–7) did not modify the basal blood pressure in SH
rats. The effect of the blockade of AT2 receptors on blood
pressure response to Ang-(1–7) was not tested in our work,
because AT2 hypothalamic receptors are not involved in the
pressor and neuronal response to angiotensinergic peptides
[26,27].
In SH rats the administration of irbesartan, an AT1 receptor
antagonist, but not D-Ala-Ang-(1–7) prevented the pressor response to hypothalamic injection of Ang-(1–7). Thus, the pressor response to hypothalamic Ang-(1–7) administration resulted
from an unspecific action of the peptide on AT1 receptors. Ang(1–7) has only a very low affinity for AT1 receptor [28] in such a
way that only the greatest dose of Ang-(1–7) exerted a pressor
response due to AT1 receptor activation. On the other hand,
the lack of cardiovascular effect by the administration of the
lower dose of Ang-(1–7) suggested that the activation of hypothalamic AT1–7 receptors did not produce a change in basal
blood pressure, indicating the absence of a compromise of this
receptor in blood pressure regulation. The pressor response to
Ang-(1–7) is lacking in WKY rats probably because of the
43
reduced activity of hypothalamic AT1 receptors with regards to
SH animals.
In the second part of the study the effects of Ang-(1–7) on the
pressor response to Ang II were evaluated in WKY and SH rats.
There would appear to be a functional interlocking of catecholamines and Ang II in the hypothalamus [1]. The mechanism by
which Ang II regulates blood pressure involves, at least in part,
brain catecholamine pathways [9]. In addition, other authors
have found that the pressor actions of centrally injected Ang II
are prevented by antagonists of noradrenaline and dopamine
[29–31].
Effects of Ang-(1–7) on noradrenaline release in hypothalamic nuclei were previously studied. Pawlak et al. [32] have
demonstrated that intracerebroventricular injection of Ang-(1–
7) did not modify hypothalamic noradrenaline levels in normotensive animals. On the other hand, in our laboratory we found
that Ang-(1–7) inhibited the release of noradrenaline induced by
Ang II in hypothalamic nuclei of aortic coarctated hypertensive
rats. Taking into account this finding, we hypothesized that Ang(1–7) could regulate the pressor response to the hypothalamic
administration of Ang II.
In the present work the intrahypothalamic administration of
Ang II exerted a greater pressor effect in SH rats than in WKY
normotensive animals, suggesting an enhanced activity of AT1
receptors on the hypertensive group. Kubo et al. [23] have also
previously demonstrated an enhancement of the pressor response to Ang II in 16 weeks aged SH animals. Given that in the
present work 8 weeks aged SH rats were used, we could suggest
that the activity of the hypothalamic angiotensinergic system is
enhanced in different hypertensive stage of SH animals.
On the other hand, whilst the co-administration of Ang-(1–7)
and Ang II did not modify the pressor response to Ang II in
WKY animals, the administration of both peptides significantly
reduced the pressor response to the octapeptide in SH rats. In
other words, the modulatory effect of Ang-(1–7) on the pressor
response to Ang II observed in hypertensive rats is lacking in
normotensive animals. Several studies have shown that the Ang(1–7) opposite effect to Ang II is enhanced in animal models of
hypertension. Benter et al. [19] have demonstrated that Ang-(1–
7) attenuates Ang II vasoconstriction in spontaneously hypertensive rats (SHR) but not in normotensive animals. So, in this
work, Ang-(1–7) reduced the pressor response of Ang II in
SH rats probably by the inhibition of angiotensin II enhanced
noradrenaline release.
In the present study the effect of the co-administration of an
AT1–7 receptor antagonist on the pressor response to Ang II were
also evaluated. Our results demonstrated that the co-administration of D-Ala-Ang-(1–7) increased the pressor effects of Ang
II in SH animals. So, it could be suggested that the hypothalamic
levels of Ang-(1–7) are implicated in the regulation of the
cardiovascular effects of Ang II.
In conclusion, our result demonstrated that the biologically
active peptide Ang-(1–7) did not have participation in the hypothalamic blood pressure regulation in WKY normotensive
animals. In SH hypertensive rats, the intrahypothalamic administration of Ang-(1–7) exerted pleiotropic effects on blood
pressure regulation. The administration of high dose of the
�44
C. Höcht et al. / Regulatory Peptides 135 (2006) 39–44
heptapeptide produced a pressor response because of an unspecific action by activation of AT1 receptors. However, the
concomitant administration of lower doses of Ang-(1–7) with
Ang II reduced the pressor response to the octapeptide probably
by inhibition of angiotensin II enhanced noradrenaline release.
Finally, the effect of AT1–7 antagonist on Ang II pressor response
should be suggest that endogenous levels of Ang-(1–7) are implicated in the regulation of the cardiovascular effects of Ang II.
References
[1] de Wardener HE. The hypothalamus and hypertension. Physiol Rev
2001;81:1599–658.
[2] Chalmers J. Brain, blood pressure and stroke. J Hypertens 1998;16:
1849–58.
[3] Chalmers J, Pilowsky P. Brainstem and bulbospinal neurotransmitter
systems in the control of blood pressure. J Hypertens 1991;9:675–94.
[4] Reis DJ, Golanov EV, Ruggiero DA, Suhn MK. Sympatho-excitatory
neurons of the rostral ventrolateral medulla are oxygen sensors and
essential elements in the tonic and reflex control of the system and cerebral
circulation. J Hypertens 1994;12:S159–80.
[5] Yang RH, Jin H, Wyss JM, Oparil S. Depressor effect of blocking
angiotensin subtype I receptors in anterior hypothalamus. Hypertension
1992;19:475–81.
[6] Teruya H, Muratani H, Takishita S, Sesoko S, Matayoshi R, Fukiyama K.
Brain angiotensin II contributes to the development of hypertension in
Dahl–Iwai salt-sensitive rats. J Hypertens 1995;13:883–90.
[7] Faber JE, Brody MJ. Central nervous system action of angiotensin during
onset of renal hypertension in awake rats. Am J Physiol 1984;247:
H349–60.
[8] Itaya Y, Suzuki H, Matsukawa S, Kondo K, Saruta T. Central renin–
angiotensin system and the pathogenesis of DOCA-salt hypertension in
rats. Am J Physiol 1986;251:H261–8.
[9] Gelband CH, Sumners C, Lu D, Raizada MK. Angiotensin receptors and
norepinephrine neuromodulation: Implications of functional coupling.
Regul Pept 1988;73:141–7.
[10] Raizada MK. Current concepts: tissue renin–angiotensin system as local
regulators in reproductive and endocrine organs. New York: Plenum; 1994.
[11] Sumners C, Raizada MK. Angiotensin II receptor subtypes in neuronal
cells. In: Raizada MK, Phillips MI, Sumners C, editors. Cellular and
molecular biology of the renin–angiotensin system. Boca Raton: CRC
Press; 1993. p. 379–411.
[12] Santos RAS, Campagnole-Santos MJ, Andrade SP. Angiotensin-(1–7): an
update. Regul Pept 2000;91:45–62.
[13] Ardaillou R, Chansel D. Synthesis of active fragments of angiotensin II.
Kidney Int 1998;52:1458–68.
[14] Ferrario CM, Chappell MC, Tallant EA, Brosnihan KB, Diz DI.
Counterregulatory actions of angiotensin-(1–7). Hypertension 1997;30
(Part 2):535–41.
[15] Campagnole-Santos MJ, Heringer SB, Batista EN, Khosla MC, Santos
RAS. Differential baroreceptor reflex modulation by centrally infused
angiotensin peptides. Am J Physiol 1992;263:R89–94.
[16] Gironacci MM, Yujnovsky I, Gorzalcsany S, Taira C, Peña C.
Angiotensin-(1–7) inhibits the angiotensin II-enhanced norepinephrine
release in coarctated hypertensive rats. Regul Pept 2004;118:45–9.
[17] Ferrario CM. Angiotensin-(1–7) and antihypertensive mechanisms. J Nephrol
1998;11:278–83.
[18] Chappell MC, Iyer SN, Diz DI, Ferrario CM. Antihypertensive effects of
angiotensin-(1–7). Braz J Med Biol Res 1998;31:1205–12.
[19] Benter IF, Diz DI, Ferrario CM. Pressor and reflex sensitivity is altered in
spontaneously hypertensive rats treated with angiotensin-(1–7). Hypertension 1995;26:1138–44.
[20] Paxinos G, Watson CH. The rat brain in stereotaxic coordinates. 2nd edn.
New York: Academic Press; 1986.
[21] Brunning JL, Kintz BL. Computational Handbook of Statistics, 2nd edn.
Glenview:Scott, Foresman and Company, Scott, 1977.
[22] Claassen V. Anaesthesia. In: Huston JP, editor. Neglected factors in
pharmacology and neuroscience research. Amsterdam: Elsevier; 1994.
p. 382–421.
[23] Kubo T, Yamaguchi H, Tsujimura M, Hagiwara Y, Fukumori R. An
angiotensin system in the anterior hypothalamic area anterior is involved in
the maintenance of hypertension in spontaneously hypertensive rats. Brain
Res Bull 2000;52:291–6.
[24] Gironacci MM, Coba MP, Peña C. Angiotensin-(1–7) binds at the type 1
angiotensin II receptors in rat renal cortex. Regul Pept 1999;84:51–4.
[25] de Gasparo M, Whitebread S, Bottari SP, Levens NR. Medicinal chemistry
of the renin–angiotensin system. In: Timmermanns PB, Wexler RR, editors.
Heterogeneity of angiotensin receptor subtypes. Amsterdam: Elsevier;
1994. p. 269–94.
[26] Bains JS, Potyok A, Ferguson AV. Angiotensin II actions in paraventricular
nucleus: functional evidence for neurotransmitter role in efferents
originating in subfornical organ. Brain Res 1992;599:223–9.
[27] Tonic angiotensinergic inputs to neurons in the anterior hypothalamic area
of rats. Brain Res 2004;1006:207–14.
[28] Rowe BP, Saylor DL, Speth RC, Absher DR. Angiotensin-(1–7) binding at
angiotensin II receptors in the rat brain. Regul Pept 1995;56:139–46.
[29] Brody MJ, Fink GD, Biggy J, Haywood JR, Gordon FJ, Johnson AK. Role
of anteroventral third ventricle (AV3V) region in experimental hypertension. Circ Res 1978;43:102–13.
[30] Camacho A, Phillips MI. Separation of drinking and pressor responses to
central angiotensin by monoamines. Am J Physiol 1981;240:R106–10.
[31] Wright JW, Harding JW. Brain angiotensin receptor subtypes in the control
of physiological and behavioral responses. Neurosci Biobehav Rev
1994;18:21–53.
[32] Pawlak R, Napiorkowska-Pawlak, Takada Y, Urano T, Nagai N, Ihara H,
Takada A. The differential effect of angiotensin II and angiotensin-(1–7) on
norepinephrine, epinephrine, and dopamine concentrations in rat hypothalamus: the involvement of angiotensin receptors. Brain Res Bull
2001;54: 689–94.
�
 Javier Opezzo
Javier Opezzo