ARTICLE IN PRESS
Psychoneuroendocrinology (2007) 32, 322–330
Available at www.sciencedirect.com
journal homepage: www.elsevier.com/locate/psyneuen
Coffee, stress and cortisol in nursing staff
Anette Harrisa,b,c, Holger Ursina,b, Robert Murisond, Hege R. Eriksena,b,�
a
Unifob health, Christiesgt 13, N-5015 Bergen, Norway
Department of Education and Health Promotion, 13, N-5015 Bergen, Norway
c
Faculty of Health and Social Sciences, Bergen University College, Haukelandsbakken 45, N-5009 Bergen, Norway
d
Department of Biological and Medical Psychology, University of Bergen, Jonas Liesvei 91, N-5009 Bergen, Norway
b
Received 4 May 2006; received in revised form 7 January 2007; accepted 9 January 2007
KEYWORDS
Salivary cortisol;
Job stress;
Work load;
Subjective health
complaints;
Health-related quality
of life;
Coffee
Summary
According to cognitive activation theory, long-lasting work demands without rest or lack of
coping may lead to sustained activation and pathology. Cortisol is one of the most
important stress hormones in humans and increased basal levels of cortisol are considered
a valid marker for sustained activation. In order to investigate this association further, we
investigate the relationships between salivary cortisol profiles, job stress, work load
(effort/reward, demand/control) and health (subjective health complaints and healthrelated quality of life) in a population of health care workers. Forty-four women filled in a
questionnaire and collected five saliva samples on two consecutive working days (1: wakeup time, 2: wake-up time+30 min, 3: wake-up time+45 min, 4: 1500 h and 5: 2200 h). There
was no relationship between psychosocial factors at work and cortisol levels in the morning
(cortisol level at wake-up time and awakening cortisol response (ACR)). Only the
confounding variable tobacco reached a significant level in the hierarchical regressions
analyses. Our significant findings are limited to the afternoon decline and the evening
values. The decrease during the day relates to decision authority, physical functioning,
general health, and vitality in the single, unadjusted regression analyses. The decrease
also relates to coffee intake, which we included originally as a confounding variable. In the
final hierarchical regression of the evening values, only decision authority and coffee were
significantly related to cortisol levels in the evening.
& 2007 Published by Elsevier Ltd.
1. Introduction
The cognitive activation theory of stress (CATS) states that
the stress response is synonymous with activation and should
�Corresponding author. Department of Education and Health
Promotion, University of Bergen, 13, N-5015 Bergen, Norway.
Tel.: +47 55586234/55589975; fax: +47 55589872.
E-mail address: hege.eriksen@psych.uib.no (H.R. Eriksen).
0306-4530/$ - see front matter & 2007 Published by Elsevier Ltd.
doi:10.1016/j.psyneuen.2007.01.003
be regarded as a general alarm system (Ursin and Eriksen,
2004). Activation (the stress response) occurs whenever
there is a discrepancy between what the organism is
expecting, and what really exists (Ursin, 1988; Levine and
Ursin, 1991; Ursin and Eriksen, 2004). The stress response
affects the biochemistry of the brain, the endocrine,
vegetative, and immune systems (Levine and Ursin, 1991).
The main components of the stress response are the
hypothalamic–pituitary–adrenal axis (the HPA axis) and the
�ARTICLE IN PRESS
Coffee, stress and cortisol in nursing staff
sympathetic part of the vegetative nervous system. It is an
essential element in the total adaptive system of the body.
Hormones associated with the stress response protect the
body in the short term and promote adaptation, but in the
long run may cause changes in the body that lead to disease
(McEwen and Seeman, 1999; Ursin, 2000). According to
CATS, long-lasting work demands without rest, or lack of
coping, may lead to sustained activation and pathology
(Levine and Ursin, 1991; Ursin and Eriksen, 2004).
Cortisol is one of the most important stress hormones in
humans and increased basal levels of cortisol are considered
to be a valid marker for sustained activation (Pruessner
et al., 1997; Wüst et al., 2000). Cortisol exhibits a marked
circadian rhythm, with peak levels usually found in the early
morning hours with decreasing concentrations thereafter
(Weitzman et al., 1971). The awakening cortisol response
(ACR) can be defined as the period of cortisol secretory
activity in the first 45–60 min immediately post-awakening
(Clow et al., 2004). Pruessner et al. (1997) have shown that
ACR is a reliable biological marker of HPA activity with high
intra-individual stability and therefore it can be used to
measure the level of psychological strain in daily life.
Previous studies have shown relationships between cortisol
and job stress (for literature review, see Hjortskov et al.,
2004), workload (Steptoe et al., 2000; Lundberg and
Hellstrøm, 2002; Steptoe et al., 2004) and subjective health
and well being (Lindfors and Lundberg, 2002). A high ACR
has been related to depressive symptoms (Pruessner et al.,
2003a), however and attenuated ACR have been found to be
related to ‘‘burnout’’ (Pruessner et al., 1999), A recent
study has shown that high levels of time pressure, effort and
effort/reward imbalance were significantly associated with
higher levels of cortisol in women (Eller et al., 2006).
Many factors influence cortisol levels (Wüst et al., 2000;
Clow et al., 2004; Hjortskov et al., 2004). Characteristics of
individuals like age and gender are important, as well as the
method used for determining the cortisol levels. Some
studies have found a relationship between age and cortisol
levels in the morning (Seeman et al., 2001; Kudielka and
Kirschbaum, 2003) while others did not find this association
(Pruessner et al., 1997; Wüst et al., 2000). Researchers have
found a relationship between gender and cortisol (Pruessner
et al., 1997; Steptoe et al., 2000; Wüst et al., 2000; Clow
et al., 2004). This is complicated further by the use of oral
contraceptives which may attenuate ACR, while there does
not seem to be any association between phase of the
menstrual cycle and cortisol (Kudielka and Kirschbaum,
2003). Factors like coffee, tobacco and alcohol may also
influence cortisol levels (Pruessner et al., 1997; Clow et al.,
2004; Hjortskov et al., 2004; Kunz-Ebrecht et al., 2004;
Steptoe and Ussher, 2006). Further clarification requires
homogenous materials and control of confounding factors.
We have therefore, studied a homogenous sample of female
health care workers.
Previous studies have been concerned mainly with the
cortisol response in the morning or total 24 h cortisol
secretion as measured in urine. The cortisol decline during
the day and the cortisol levels in the evening appear to be
related to strain in daily life and health. Sluiter et al. (1998,
1999, 2003) investigated how working conditions may lead
to health complaints. Their studies showed that sufficient
restitution was an important factor for health. In these
323
studies, recovery from work was measured as the return to
base line levels of cortisol after work (Sluiter et al., 1998).
A recent study has shown that in a population of women
working within the public health care sector, self-rated
recovery from work stress was related to allostatic load (von
Thiele et al., 2006). We suggest that high cortisol levels in
the evening indicate lack of restitution (recovery) and may
be an indicator for sustained activation (Eriksen and Ursin,
2004). Studies have shown that women’s stress seems to be
more reflected in elevated arousal not only during, but also
after work (Lundberg and Frankenhauser, 1999). In the
present study we investigated the relationship between
salivary cortisol profile, self-reported job stress, work load
and health in a sample of female health care workers. Their
working situation is known to be taxing (Engstrom et al.,
2006). We collected five saliva samples on two consecutive
working days. Work load was measured with the demand/
control model (Karasek and Theorell, 1990) and the effort/
reward imbalance model (Siegrist, 1996). Job stress was
measured with the Cooper Stress Index (CSI) (Cooper, 1981)
and health was measured with subjective health complaints
(SHC) inventory (Eriksen et al., 1999) and health-related
quality of life (SF-36) (Ware et al., 1994; Loge et al., 1998).
Based on the concept of need for recovery after work
(Sluiter et al., 1998, 1999, 2003), we hypothesised that
there would be a relationship between high scores on
workload and/or job stress and a flat cortisol profile (high
cortisol at wake-up time, attenuated response to stress
stimuli and high cortisol in the evening). We also expected
to find that participants with high scores on SHC and/or low
health-related quality of life would have high cortisol levels
in the evening.
2. Methods
2.1. Subjects
The participants were forty-four women mean aged 48 years
(SD ¼ 8.16) working in three nursing homes for the elderly in
Bergen. The data were collected as part of an integrated
health programme that combined exercise and health
information. Two hundred and twenty-seven employees
initially were invited to the program and 135 (59.5%)
accepted the invitation to take part in the intervention.
Only those that worked daytime shifts when they collected
saliva were included in this study (n ¼ 54). Out of these 54
employees, nine subjects were excluded because of
problems with sample collection, and one participant was
excluded because the questionnaires were completed
inadequately. The project was approved by the ethics
committee and all participants gave written informed
consent.
2.2. Study protocol
Diurnal cortisol was measured from saliva using Salivette
collection tubes (DPC Norway, Brakerøya, Drammen), which
consists of a small cotton swab inside a standard centrifugation tube. Five saliva samples were collected on two
consecutive working days: at wake-up time, 30 and 45 min
after wake-up time, at 1500 and 2200 h. All participants at
�ARTICLE IN PRESS
324
the workplace were instructed in how to use the salivette.
They were instructed to chew gently on the cotton swab for
1 min to obtain the desired amount of saliva. Participants
were asked to avoid meals, drinks and nicotine for 15 min
before sample collection and to take the first sample while
still lying in bed. They were instructed to keep the samples
frozen until they were returned to the laboratory for further
analyses. In the laboratory they were subsequently stored in
a freezer until they were thawed for the biochemical
analysis. Participants were asked to note their time of
awakening and the exact time they collected the saliva
samples. Compliance with the waking sampling protocol
was judged by computing the difference between the
time participants stated they had woken up and the
time they stated that the first saliva sample had been
taken. Participants showing a difference of more than
10 min were excluded.
2.3. Instruments
All participants filled in a comprehensive questionnaire
covering a broad range of factors including demographic
variables, number of cigarettes, cups of coffee and units of
alcohol (one unit alcohol ¼ a half bottle of beer or one glass
of wine or one drink), use of oral contraceptives, weight and
height were measured to calculate BMI, health status/
problems, physical and psychological variables at work,
factors related to work organisation and leadership, social
support and family relationships, and individual coping
resources.
2.3.1. Quality of life
Health-related quality of life was measured by the generic
health status measure SF-36 for health situations during the
last 4 weeks (Loge et al., 1998; Ware et al., 1994, 2000).
Eight subscales were computed; physical functioning (10
items), role limitations due to physical problems (4 items),
bodily pain (2 items), general health (5 items), vitality
(4 items), social functioning (2 items), role limitations
due to emotional problems (3 items) and mental health
(5 items). The scoring of the items varied from dichotomous
scales (yes/no) to six-point ordinal scales. The questionnaire
has been tested and has satisfactory reliability and validity
(Loge et al., 1998).
2.3.2. Subjective health complaints
SHC were measured by 29 items on subjective somatic and
psychological complaints experienced during the last 30
days, using the SHC inventory (Eriksen et al., 1999). Severity
was scored on a four-point scale, from 0 (no complaints) to 3
(severe complaints). Five sub-scales and a total health score
(SHC-total) were computed; musculoskeletal pain (8 items:
headache, neck pain, upper back pain, low back pain, arm
pain, shoulder pain, migraine and leg pain), pseudoneurology (7 items: palpitation, heat flushes, sleep problems,
tiredness, dizziness, anxiety and sadness), gastrointestinal
problems (7 items: heartburn, epigastric discomfort, ulcer/
non-ulcer dyspepsia, stomach pain, gas discomfort, diarrhoea and constipation), allergy (5 items: asthma, breathing
difficulties, eczema, allergy, and chest pain) and flu
(2 items: cold flu and coughing). The questionnaire has
A. Harris et al.
been tested and has satisfactory reliability and validity
(Eriksen et al., 1999).
2.3.3. Job stress
The job stress factor was measured by the CSI (Cooper, 1981,
Endresen et al., 1991). Questions were scored on a six-point
scale ranging from 0 to 5 (0 ¼ no stress and 5 ¼ considerable
stress). Four sub-scales were computed; communication
(8 items) is related to lack of communication and influence,
conflicts with management, co-workers, and different
groups of employees. Leadership (4 items) is related to
the employee’s relationship to management and subordinates, a feeling of being undervalued, and pay. Relocation
(4 items) is related to stress caused by promotion prospects,
relocation, managing people, and taking work home. Workload (3 items) as a source of job stress is related
to workload, time pressure and deadlines, and workrelated demands influencing private life. The questionnaire
has satisfactory validity and reliability (Endresen et al.,
1991).
2.3.4. Coping
Coping was measured by the instrumental mastery oriented
coping (IMOC) factor from the CODE (Eriksen et al., 1997),
based on the short version of the Utrecht Coping List (UCL)
(Schreurs et al., 1988, 1993). IMOC implies an instrumental,
active, goal-oriented coping style. To get a high score
on IMOC, the score on active problem solving from UCL
must be high, and the score on avoidance and passive
expectancy, and depressive reaction pattern from the UCL
must be low (Eriksen et al., 1997). Scores are based on
active problem solving (7 items), avoidance and passive
expectancy (8 items), depressive reactions (7 items).
The questionnaire has satisfactory reliability and validity
(Eriksen et al., 1997).
2.3.5. Effort/reward imbalance
The effort/reward imbalance at work questionnaire was
used to measure workload, effort and reward (Siegrist,
1996). The questionnaire consists of 17 questions rated on a
four-point scale. The effort scale (6 items) measures an
intrinsic personal, coping-related component of stressful
experience at work, while the reward scale (11 items)
measures an extrinsic perceived work situation component.
The total workload score (effort/reward) is a measure of the
imbalance between these two components. A high score
indicates high workload, effort or reward. The questionnaire
has satisfactory reliability and validity (Siegrist, 1996).
2.3.6. Job demands
Job demands were measured by five questions from the
demand dimension in the short Swedish version (Theorell
et al., 1993) of the demand/control model (Karasek and
Theorell, 1990). The job demands subscale is the sum of five
items inquiring about excessive work, conflicting demands,
insufficient time to work, fast pace, and working hard
(5 items). Questions were scored on a four-point scale
ranging from strongly disagreeing to strongly agreeing.
The questionnaire has satisfactory validity and reliability
(Theorell et al., 1993).
�ARTICLE IN PRESS
Coffee, stress and cortisol in nursing staff
2.3.7. Job control
Job control (decisions latitude) was measured by six
questions from the decision latitude dimension in the short
version of the demand/control model (Theorell et al.,
1993). The job control (decision latitude) scale (6 items) is
the sum of two subscales; skill discretion (4 items) and
decision authority (2 items). Questions were scored on a
four-point scale ranging from strongly disagreeing to
strongly agreeing and were related to creativity, skills, task,
variety, learning new things, and the amount of repetitive
work. The questionnaire has satisfactory validity and
reliability (Theorell et al., 1993).
2.3.8. Social support
Social support was measured by six questions from the
Swedish version of The Job Content Questionnaire (6 items)
(Theorell et al., 1993). The social support scales include
support from co-workers and supervisors. For each item the
respondents could choose from one of four responses ranging
from strongly disagreeing to strongly agreeing.
2.4. Cortisol analysis
Salivary cortisol was assayed with Coat-a-Count RIA kit from
Diagnostic Products Corporation (DPC, Los Angeles, CA).
Intra-assay variability was 3.0–5.1 and inter-assay variability
was 4.0–6.4. The distribution of cortisol level at each time
point was positively skewed, so a logarithmic transformation
(log 10) was conducted to ensure that scores approximated a
normal distribution (Tabachnick and Fidell, 1996).
2.5. Statistics
SPSS 13.0 for Windows was used for the statistical analyses.
Outcome variables were cortisol level at wake-up time, ACR,
cortisol decline from morning to evening and cortisol level in
the evening (2200 h). The ACR was measured using the
integrated area under the curve (AUC). This was calculated
by first subtracting the 0-min awakening value from the 30 and
45 values, to obtain baseline-corrected values, and then using
the
trapezoidal
method
(Pruessner
et al., 2003b). Cortisol decline from morning to evening was
measured by calculating changes between levels obtained
(awake+0045 h.) and the evening sample (2200 h). Pearson
correlation coefficients were used to calculate the relationship
between the two collecting days, and mean cortisol levels over
the two collection days were used for the analyses. Pearson
product–moment correlations were also used to examine the
relationship between health-related factors, psychosocial
factors, coping, potential covariates and measures of cortisol.
Due to low sample size, only those variables which correlated
significantly with the different cortisol measures were taken
into further analyses. Multiple linear regression analyses were
performed to examine the contributions of each of the
significant variables to the different cortisol measures. The
regression analyses were carried out manually as follows.
Single regression analyses were executed for each variable
that showed a significant correlation with that particularly
cortisol measure. Then one variable at a time was entered into
the hierarchical regressions model, starting with the potential
covariates, followed by health-related factors and psychoso-
325
cial factors as independent variables and the different cortisol
measures as dependent variables. Tolerances were checked to
control for multicollinearity. P values of less than .05 were
considered statistically significant.
3. Results
3.1. Simple statistics
Twenty-eight participants collected all five saliva samples, 36
participants collected the first sample at wake-up time, 28
participants collected the three samples we used for
calculating the ACR and 40 participants collected the evening
sample. The relationship between the first and second
sampling day was investigated using Pearson product–moment
correlation coefficient. There was a strong positive correlation between the cortisol samples on the two collecting days:
at wake-up time (r ¼ .67, n ¼ 20, po.01), 30 min after wakeup time (r ¼ .71, n ¼ 24, po.01), 45 min after wake-up time
(r ¼ .69, n ¼ 23, po.01), at 15.00 (r ¼ .40, n ¼ 30, po.05)
and at 2200 h (r ¼ .54, n ¼ 25, po.01).
For descriptive statistics and correlations between potential covariates, health-related factors, psychosocial factors
and measures of cortisol, see Table 1. There was a positive
correlation between physical functioning (SF-36), general
health (SF-36), vitality (SF-36) and cortisol decline and a
negative correlation between vitality (SF-36) and cortisol
levels in the evening. There were no significant correlations
between the other factors in the SF-36 scale or the SHC
inventory and any of the cortisol outcome variables. The
population reported good health-related quality of life (mean
score on SF-36 ¼ 77.8, SD ¼ 20.8) compared to the Norwegian
population where the mean score is 50 (Loge et al., 1998).
The factors from the demand control model showed a
significant correlation with the different cortisol measurement in this population (Table 1). Decision latitude was
positively correlated to cortisol levels at wake-up time and
decision authority was positively correlated to cortisol levels
at wake-up time and cortisol decline during the day but
negatively correlated to ACR and cortisol levels in the
evening. Social support was positively correlated to ACR.
Effort/reward imbalance and self-reported job stress had no
significant influence on cortisol in this population. Furthermore, there was a positive correlation between coping and
cortisol decline during the day and a negative correlation
between coping and cortisol level in the evening.
When examining the association between potential
confounding variables and the different cortisol measures,
we found a negative correlation between coffee and cortisol
level at wake-up time and cortisol decline during the day
and a positive correlation between coffee and cortisol levels
in the evening. Tobacco was negatively correlated to cortisol
level at awakening and positively correlated to the ACR.
There was a negative correlation between BMI and ACR.
3.2. Regression analyses of the different cortisol
measurements
3.2.1. Cortisol levels at wake-up time and ACR
Table 2 shows the result of the single unadjusted regression
analyses and the hierarchical multiple regression analyses
�ARTICLE IN PRESS
326
A. Harris et al.
Table 1 Descriptive statistics and Pearson product–moment correlations between potential covariates, health related
factors, psychosocial factors and measures of cortisol.
1.Age
2. Coffee
3. Tobacco
4. Alcohol
5. BMI
6. Subjective health complaints total (SHC)
7. Musculoskeletal complaints (SHC)
8. Pseudoenurological complaints (SHC)
9. Gastrointestinal complaints (SHC)
10. Allergy (SHC)
11. Flu (SHC)
12. Physical functioning (SF-36)
13. Role physical (SF-36)
14. Bodily pain (SF-36)
15. General health (SF-36)
16. Vitality (SF-36)
17. Social functioning (SF-36)
18. Role emotional (SF-36)
19. Mental health (SF-36)
20. Job stress total (CSI)
21. Communication (CSI)
22. Leadership (CSI)
23. Workload (CSI)
24. Relocation (CSI)
25. Effort/reward imbalance (ERI)
26. Effort
27. Reward
28. Workload (demand/control)
29. Physical demands
30. Decision latitude (control)
31. Skill discretion
32. Decision authority
33. Social support
34. Coping (IMOC)
N
Mean (SD)
Awakening
ACR
Decline
44
44
41
40
44
44
44
44
44
44
44
42
43
44
43
42
44
42
42
43
41
43
43
42
39
39
39
44
44
44
44
44
44
43
48.8
2.3
3.7
1.5
24.7
10.8
4.7
2.9
1.8
.8
.6
87.7
81.8
71.3
75.6
56.8
81.8
87.7
79.7
24.8
1.2
1.1
2.2
.7
.1
16.3
46.0
.8
13.8
17.7
11.2
17.7
19.5
3.1
.004
�.359*
�.485**
.118
.237
�.082
�.189
�.176
.077
.135
.073
�.078
.181
.119
.090
.302
.310
�.125
.160
.145
.062
.204
.257
.002
�.061
�.343
�.050
�.224
�.039
.338*
.192
.365*
�.294
.076
.141
.278
.531**
�.060
�.406*
�.001
.154
.130
�.201
�.228
�.088
.209
�.180
�.155
�.189
�.317
�.267
.123
�.193
�.234
�.149
�.340
�.348
�.010
�.107
.173
.213
.170
.000
�.286
�.119
�.387*
.379*
�.025
.118
�.376*
.072
�.013
�.161
�.266
�.187
�.276
�.097
�.262
�.276
.363*
.139
.267
.337*
.420*
.171
.101
.105
�.068
�.135
.052
.103
�.034
�.252
�.127
.116
�.224
�.238
.061
�.195
.390*
.130
.389*
(8.2)
(.9)
(6.4)
(1.7)
(3.9)
(8.9)
(4.5)
(2.5)
(2.5)
(1.4)
(1.1)
(11.4)
(31.1)
(24.6)
(16.1)
(19.1)
(21.8)
(27.8)
(14.3)
(17.6)
(1.1)
(1.1)
(1.4)
(.8)
(.3)
(5.0)
(6.8)
(.2)
(2.5)
(2.5)
(1.9)
(2.5)
(2.7)
(.2)
Cortisol
2200 h
�.140
.426**
.000
.048
.074
.156
.149
.204
�.023
.056
.185
�.181
�.170
�.223
�.299
�.331*
�.064
.004
�.090
�.079
.005
�.228
�.193
�.033
.246
.145
�.103
.232
.224
�.085
.216
�.459**
�.020
�.316*
*Po.05 (Pearsons correlations coefficient).
**Po.01 (Pearsons correlations coefficient).
predicting the cortisol levels at wake-up time. In an
unadjusted model coffee, tobacco, decision latitude and
decision authority was significantly associated with the
cortisol level at wake-up time, but none of the variables
reached a significant level in the hierarchical analyses.
Table 3 shows the result of the single unadjusted
regression analyses and the hierarchical multiple regression
analyse predicting the ACR. In an unadjusted model tobacco,
BMI, decision authority, and social support were significantly
associated with the ACR. Among the potential confounding
variables, tobacco was the only variable that reached
significant levels in the hierarchical analyse (see Table 3).
3.2.2. Cortisol decline during the day and cortisol levels
in the evening (2200 h)
Table 4 shows the result of the single unadjusted regression
analyses and the hierarchical multiple regression analyses
predicting the cortisol decline during the day. In an
unadjusted model coffee, physical functioning (SF-36),
general health (SF-36), vitality (SF-36), decision authority
and coping was significantly associated with cortisol level at
wake-up time, but only coffee reached a significant level in
the hierarchical model. Coffee alone accounted for 8.4% of
the variance in the cortisol decline during the day
(b ¼ �.34, po.05).
Table 5 shows the result of the single unadjusted
regression analyses and the hierarchical multiple regression
analyses predicting the cortisol levels in the evening.
Unadjusted coffee, vitality (SF-36), decision authority and
coping were significantly associated with the cortisol level in
the evening (2200 h). Coffee reached a significant level
at step one and two but not in step three. Only decision
authorities reached a significant level in step three (see
Fig. 1). Coffee alone accounted for 15.2% of the variance in
cortisol levels in the evening (b ¼ .42, po.01), while
�ARTICLE IN PRESS
Coffee, stress and cortisol in nursing staff
327
Table 2 Single and hierarchical multiple linear regression analyses of age, coffee, tobacco, decision latitude (control) and
decision authority with cortisol level at wake-up time as dependent variable.
Not adjusted
1.
2.
3.
4.
5.
Age
Coffee
Tobacco
Decision latitude (control)
Decision authority
Step one
Step two
b
P
b
P
.004
�.359
�.357
.338
.365
.982
.032
.032
.044
.029
�.270
�.267
.114
.117
Adjusted R
R change
Step three
b
P
�.211
�.241
.226
.220
.154
.175
.143
.192
b
P
�.192
�.227
.129
.157
.274
.183
.546
.471
.167
.046
.154
.013
Table 3 Single and hierarchical multiple linear regression analyses of age, tobacco, BMI, decision authority and social
support with awakening cortisol response (ACR) as dependent variable.
Not adjusted
1.
2.
3.
4.
5.
Age
Tobacco
BMI
Decision authority
Social support
Step one
b
P
.141
.531
�.406
�.387
.379
.475
.004
.032
.042
.047
Adjusted R
R change
Step two
Step three
b
P
b
P
b
P
.446
�.250
.018
.170
.364
�.255
�.155
.091
.166
.440
.317
�.203
�.200
.296
.126
.251
.302
.088
.282
.337
.270
.017
.333
.082
Table 4 Single and hierarchical multiple linear regression analyses of age, coffee, physical functioning (SF-36), general
health (SF-36), vitality (SF-36), decision authority and coping with cortisol decrease as dependent variable.
Not adjusted
1.
2.
3.
4.
5.
6.
7.
Age
Coffee
Physical functioning
General health
Vitality
Decision authority
Coping (IMOC)
Adjusted R
R change
b
P
.118
�.376
.363
.337
.420
.390
.389
.492
.024
.032
.047
.012
.019
.019
Step one
Step two
b
P
�.335
.053
.084
.112
coffee, vitality, decision authority and coping together
accounted for 22.2% of the variance in cortisol levels in
the evening.
The tolerance figures were between .63 and .89 for all the
independent variables.
4. Discussion
There was no relationship between psychosocial factors at
work and cortisol levels in the morning (cortisol level at
b
P
�.258
.297
�.004
.228
.196
.127
.985
.238
.188
.174
Step three
Step four
b
b
P
�.149
.234
.039
.197
.067
.181
.506
.256
.858
.318
.727
.342
�.207
.266
.005
.219
.117
.171
.010
.337
.189
.981
.263
.526
.169
.024
wake-up time and ACR). Only the confounding variable
tobacco, reached a significant level in the hierarchical
analyses. Our significant findings are limited to the afternoon decline and the evening values of cortisol. The
decrease during the day relates to decision authority,
physical functioning, general health, and vitality in the
single, unadjusted regression analyses. The decrease also
related to coffee intake, which we included originally as a
confounding variable. In the final hierarchical regression of
the evening values, only decision authority and coffee were
significant.
�ARTICLE IN PRESS
328
A. Harris et al.
Table 5 Single and hierarchical multiple linear regression analyses of age, coffee, vitality (SF-36), decision authority and
coping with cortisol level in the evening (2200 h) as dependent variable (n ¼ 39).
Not adjusted
1.
2.
3.
4.
5.
Age
Coffee
Vitality
Decision authority
Coping (IMOC)
Step one
b
P
�.140
.426
�.331
�.459
�.316
.390
.006
.040
.003
.047
Adjusted R
R change
Step two
Step four
b
P
b
P
b
P
b
P
.418
.008
.340
�.194
.043
.238
.246
�.147
�.329
.135
.351
.038
.222
�.140
�.315
�.075
.201
.382
.052
.643
.152
.175
.162
.032
low score
25
Step three
.240
.093
.222
.004
high score
Cortisol nmol/l
20
15
10
5
0
Awakenig
Awake+0030h
awake+0045h
Timepoint
1500h
2200h
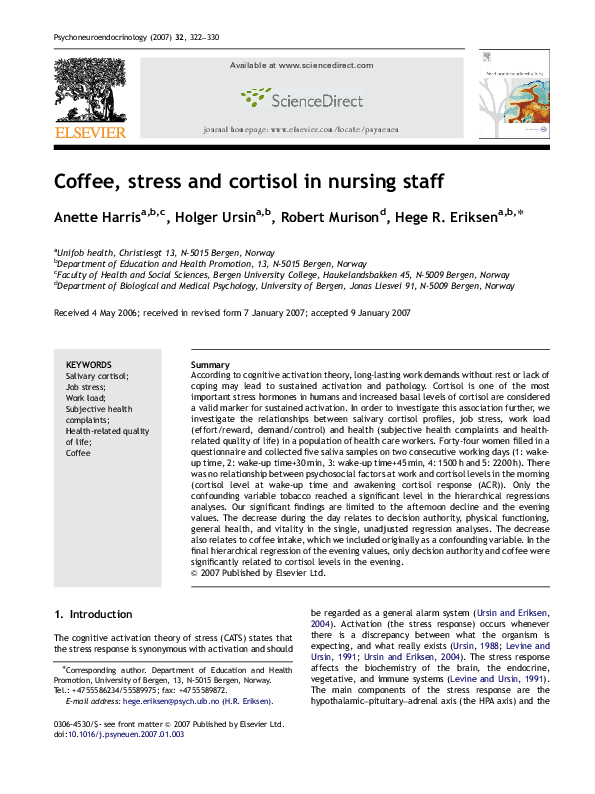
Figure 1 Cortisol levels at each time point in participants with high versus low score on decision authority. The graph shows the
mean value over time, with error bars representing the standard error of the mean. Participants with high score on decision authority
had significantly lower cortisol levels in the evening (2200 h) (po.05).
The surprising effect in this study is the effect of the
coffee intake. Coffee alone accounted for 8.4% of the
cortisol decline during the day and 15.2% of the cortisol
level in the evening (2200 h). This may be more than just an
irritating confounding factor. Coffee is a strongly activating
and stimulating drink. It is well known that the caffeine in
coffee activates the human stress axis but the underlying
mechanisms are not yet fully delineated (Al ‘Absi and
Lovallo, 2004). The caffeine’s stimulatory effects influence
sleep and it is well known that the effect of coffee last for
hours (Shilo et al., 2002). Drinking coffee during the day may
lead to longer time before the general activation goes down,
and may interfere with the restitution process.
Some previous studies have not found any relationship
between caffeine and cortisol in healthy volunteers (Spindel
et al., 1984; Uhde et al., 1985; Zanoboni and Zanaboni
Muciaccia, 1987), while other studies have found that
caffeine may elevate cortisol secretion in humans at rest
and during mental stress (Lovallo et al., 1996; Lane et al.,
2002). There is also evidence of adaptation to coffee intake.
Lovallo et al. (2005) found that healthy consumers taking
repeated doses of caffeine during the day have statistically
significant increases in cortisol secretion during the afternoon hours. The study also showed that cortisol responses to
caffeine are reduced, but not eliminated, in healthy young
men and women who consumed caffeine on a daily basis. In
a recent animal study, injections of caffeine led to
prolonged elevations in corticosterone, the highest doses
yielding elevations for up to two hours (Patz et al., 2006).
Low-to-moderate doses failed to modulate the corticosterone response to loud white noise, but modulatory effects of
high caffeine doses were not tested. The interaction
between stress factors and caffeine effect suggested from
our studies is supported by findings from medical students.
They got more effect from oral doses of caffeine (coffee or
caffeine tablets) during an examination period than in
periods without examination (Shepard et al., 2000).
Clinically, persons with high risk of hypertension have more
�ARTICLE IN PRESS
Coffee, stress and cortisol in nursing staff
rapid and prolonged cortisol responses to caffeine than do
low-risk persons (Al’Absi et al., 1998). The interaction
between caffeine and stress or activation may improve
performance but may also have negative health effects on
blood pressure (Al’Absi et al., 1998; Shepard et al., 2000), or
restitution, as in our study. However, other studies found
that moderate consumption of both caffeinated and
decaffeinated coffee may lower risk of type 2 diabetes in
younger and middle-aged women (van Dam et al., 2006).
This study showed that constituents other than caffeine may
have a positive effect on health. In the present study we
only have data on coffee but not other caffeine sources like
tea or caffeinated soft drinks, so we cannot calculate the
total caffeine intake.
Situations where individuals are faced with strong
stressors and only few possibilities to influence situations
may lead to ‘‘sustained activation’’ and an inability to
recover (Ursin and Eriksen, 2004). The need for recovery
after a working day is one possibility to operationalise
‘‘sustained activation’’ (Kristenson et al., 2004). In our study
there was a relationship between high score on ‘‘decision
authority’’ (influence on the job, how to perform work and
the freedom to make decisions) and low cortisol levels in the
evening. This may be an indication of insufficient recovery
and insufficient restitution (Sluiter et al., 1999). Insomnia
gives an increased risk for permanent work disability
(Sivertsen et al., 2006). Our findings support Theorell’s
(Theorell et al., 2001) findings of a relationship between
decision authority (control) and low cortisol in the evening.
The results are also supported by the findings of Sluiter et al.
(1999) showing low control and lack of recovery after work
and Bollini et al. (2004) showing that more internal locus of
control was related to a reduced cortisol response.
The conclusions from the present study are limited by the
small sample size, which reduces statistical power. However,
the data was performed in a relative homogeneous healthy
sample, collected at the same time of the year, almost in
the same time in the morning on two consecutive working
days. These facts reduced the influence of potential
confounders and increase the reliability of the findings.
5. Conclusion
In conclusion, the present study showed that high cortisol
levels in the evening were related to coffee and to low
scores on decision authority. Coffee consumption should
therefore be controlled in future studies. The present study
provides preliminary support for the idea that poor recovery
may be an important factor for the relationship between
sustained activation and pathology.
Role of funding source
The study was funded by grants from the University of
Bergen, the Norwegian Research Council, and the Ministry of
Health and Social Affairs through the Research Unit of the
Norwegian Back Pain Network. They have had no further role
in study design, data collection, analysis and interpretation
of data, in the writing of the report or in the decision to
submit the paper for publication.
329
Conflict of interest
None declared.
Acknowledgements
The authors would like to thank Eli Nordeide and Randi F.
Espelid for analysis of cortisol, Aud Skogen for administration of the data collection, Nina Konglevoll and Linda Sandal
for technical assistance and Stein Atle Lie for assistance with
the statistical analyses.
References
Al ‘Absi, M., Lovallo, W.R., 2004. Caffeine effects on the human
stress axis. In: Nehlig, A. (Ed.), Coffee, Tea, Chocolate and the
Brain. CRC Press, Boca Raton, FL, pp. 113–131.
Al’Absi, M., McKey, B., Sung, B.H., Whitsett, T.L., Wilson, M.F.,
1998. Hypothalamic–pituitary–adrenocortical responses to psychological stress and caffeine in men at high and low risk for
hypertension. Psychosom. Med. 60, 521–527.
Bollini, A.M., Walker, E.F., Hamann, S., Kestler, L., 2004. The
influence of perceived control and locus of control on the
cortisol and subjective responses to stress. Biol. Psychol. 67,
245–260.
Clow, A., Thorn, L., Evans, P., Hucklebridge, F., 2004. The
awakening cortisol response: methodological issues and significance. Stress 7, 29–37.
Cooper, C.L., 1981. The Stress Check. Prentice Hall, New York.
Eller, N.H., Netterstrøm, B., Hansen, Å.M., 2006. Psychosocial
factors at home and at work and levels of salivary cortisol. Biol.
Psychol., July 7 (Epub ahead of print).
Endresen, I.M., Ellertsen, B., Endresen, C., Hjelmen, A.M., Matre,
R., Ursin, H., 1991. Stress at work and psychological and
immunological parameters in a group of Norwegian female bank
employees. Work Stress 5, 217–227.
Engstrom, M., Ljunggren, B., Lindqvist, R., Carlsson, M., 2006. Staff
satisfaction with work, perceived quality of care and stress
in elderly care: psychometric assessments and associations.
J. Nurs. Manage. 14 (4), 318–328.
Eriksen, H.R., Ursin, H., 2004. Subjective health complaints,
sensitization, and sustained cognitive activation (stress).
J. Psychosom. Res. 56, 445–448.
Eriksen, H.R., Olff, M., Ursin, H., 1997. The CODE: a revised battery
for coping and defence and its relations to subjective health.
Scand. J. Psychol. 38, 175–182.
Eriksen, H.R., Ihlebæk, C., Ursin, H., 1999. A scoring system for
subjective health complaints (SHC). Scand. J. Public. Health 1,
63–72.
Hjortskov, N., Garde, A.H., Ørbæk, P., Hansen, Å.M., 2004.
Evaluation of salivary cortisol as a biomarker of self-reported
mental stress in field studies. Stress Health 20, 91–98.
Karasek, R., Theorell, T., 1990. Healthy Work: Stress, Productivity,
and the Reconstruction of Working Life. Basic Books Inc.
Publishers, New York.
Kristenson, M., Eriksen, H.R., Sluiter, J.K., Starke, D., Ursin, H.,
2004. Psychobiological mechanisms of socioeconomic differences in health. Soc. Sci. Med. 58, 1511–1522.
Kudielka, B.M., Kirschbaum, C., 2003. Awakening cortisol responses
are influenced by health status and awakening time but not by
menstrual cycle phase. Psychoneuroendocrinology 28, 35–47.
Kunz-Ebrecht, S., Kirschbaum, C., Marmot, M., Steptoe, A., 2004.
Differences in cortisol awakening response on work days and
weekends in women and men from the Whitehall II cohort.
Psychoneuroendocrinology 29, 516–528.
�ARTICLE IN PRESS
330
Lane, J.D., Piepier, C.F., Phillips-Bute, B.G., Bryant, J.E., Kuhn,
C.M., 2002. Caffeine affects cardiovascular and neuroendocrine
activation a work and home. Psychosom. Med. 64, 595–603.
Levine, S., Ursin, H., 1991. What is stress? In: Brown, M.R., Rivier,
C., Koob, G. (Eds.), Stress, Neurobiology and Neuroendocrinology. Marcel Dekker, New York, pp. 3–21.
Lindfors, P., Lundberg, U., 2002. Is low cortisol release an indicator
of positive health? Stress Health 18, 153–160.
Loge, J.H., Kaasa, S., Hjermstad, M.J., Kvien, T.K., 1998. Translation and performance of the Norwegian SF-36 Health Survey in
patients with rheumatoid arthritis. I. Data quality, scaling
assumptions, reliability, and construct validity. J. Clin. Epidemiol. 5, 1069–1076.
Lovallo, W.R., Al’Absi, M., Blick, K., Whitsett, T., Wilson, M.F., 1996.
Stress-like adrenocorticotropin responses to caffeine in young
healthy men. Pharmacol. Biochem. Behav. 55, 365–369.
Lovallo, W.R., Whitsett, T.L., Al’Absi, M., Sung, B.H., Vincent, A.S.,
Wilson, M.F., 2005. Caffeine stimulation of cortisol secretion
across the waking hours in relation to caffeine intake levels.
Psychosom. Med. 67, 734–739.
Lundberg, U., Frankenhauser, M., 1999. Stress and workload of men
and women in high ranking positions. J. Occup. Health Psychol.
4, 142–151.
Lundberg, U., Hellstrøm, B., 2002. Workload and morning salivary
cortisol in women. Work Stress 16, 356–363.
McEwen, B.S., Seeman, T., 1999. Protective and damaging effects of
mediators of stress: Elaborating and testing the concepts of
allostasis and allostatic load. Ann. NY Acad. Sci. 896, 30–47.
Patz, M.D., Day, H.E., Burow, A., Campeau, S., 2006. Modulation of
the hypothalamo-pituitary-adrenocortical axis by caffeine.
Psychoneuroendocrinology 31, 493–500.
Pruessner, J.C., Wolf, O.T., Hellhammer, D.H., Buske-Kirschbaum,
A., von Auer, K., Jobst, S., Kaspers, F., Kirschbaum, C., 1997.
Free cortisol levels after awakening: a reliable biological marker
for the assessment of adrenocortical activity. Life. Sci. 61,
2539–2549.
Pruessner, J.C., Hellhammer, D.H., Kirschbaum, C., 1999. Burnout,
perceived stress and cortisol responses to awakening. Psychosom. Med. 61, 197–204.
Pruessner, M., Hellhammer, D.H., Pruessner, J.C., Lupien, S.J.,
2003a. Self-reported depressive symptoms and stress levels in
healthy young men: associations with the cortisol response to
awakening. Psychosom. Med. 65, 92–99.
Pruessner, J.C., Kirschbaum, C., Meinlschmid, G., Hellhammer,
D.H., 2003b. Two formulas for computation of the area under
the curve represent measures of total hormone concentration
versus time-dependent change. Psychoneuroendocrinology 28,
916–931.
Schreurs, P.J.G., Tellegen, B., Van De Willige, G., Brosschot, J.F.,
1988. De Utreschtse Coping Lijst: Handleiding. Lisse, Swets en
Zeitlinger.
Schreurs, P.J.G., Van De Willige, G., Brosschot, J.F., Grau, G., 1993.
De Utrechtse Copinglijst: UCL. Handleiding, second ed. Lisse,
Swets en Zeitlinger.
Seeman, T.E., Singer, B., Wilkinson, C.W., McEwen, B., 2001.
Gender differences in age-related changes in HPA axis reactivity.
Psychoneuroendocrinology 26, 225–240.
Shepard, J.D., AlÀbsi, M., Whitsett, T.L., Passay, R.B., Lovallo,
W.R., 2000. Additive pressor effects of caffeine and stress in
male medical students at risk for hypertension. Am. J.
Hypertens. 13, 475–481.
Shilo, L., Sabbah, H., Hadari, R., Kovatz, S., Weinberg, U., Dolev, S.,
Dagan, Y., Shenkman, L., 2002. The effects of coffee consumption on sleep and melatonin secretion. Sleep Med. 3, 271–273.
Siegrist, J., 1996. Adverse health effects of high-effort/low-reward
conditions at work. J. Occup. Health Psychol. 1, 27–43.
Sivertsen, B., Overland, S., Neckelmann, D., Glozier, N., Krokstad,
S., Pallesen, S., Nordhus, I.H., Bjorvatn, B., Mykletun, A., 2006.
View publication stats
A. Harris et al.
The long-term effect of insomnia on work disability. The HUNT-2
Historical Cohort Study. Am. J. Epidemiol. 163 (11), 1018–1024.
Sluiter, J.K., Van der Beek, A.J., Frings-Dresen, M.H.W., 1998.
Workstress and recovery measured by urinary catecholamines
and cortisol excretion in long distance coach drivers. Occup.
Environ. Med. 55, 407–413.
Sluiter, J.K., Van der Beek, A.J., Fring-Dresen, M.H.W., 1999. The
influence of work characteristics on the need of recovery and
experienced health: a study on coach drivers. Ergonomics 42,
573–583.
Sluiter, J.K., Croon, E., Meijman, T., Frings-Dresen, M., 2003. Need
for recovery from work related fatigue and its role in the
development and prediction of subjective health complaints.
Occup. Environ. Med. 60, 62–70.
Spindel, E.R., Wurtman, R.J., McCall, A., Carr, D.B., Conlay, L.,
Griffith, L., Arnold, M.A., 1984. Neuroendocrine effects of
caffeine in normal subjects. Clin. Pharmacol. Ther. 36, 402–407.
Steptoe, A., Ussher, M., 2006. Smoking, cortisol and nicotine. Int. J.
Psychophysiol. 59 (3), 228–235.
Steptoe, A., Cropley, M., Griffith, J., Kirschbaum, C., 2000. Job
strain and anger expression predict early morning elevations in
salivary cortisol. Psychosom. Med. 62, 286–292.
Steptoe, A., Siegrist, J., Kirschbaum, C., Marmot, M., 2004.
Effort–reward imbalance, overcommitment, and measures of
cortisol and blood pressure over the working day. Psychosom.
Med. 66, 323–329.
Tabachnick, B.G., Fidell, L.S., 1996. Using Multivariate Statistics,
third ed. Harper Collins, New York.
Theorell, T., Michèlsen, H., Nordemar, R., Music 1 study group,
1993. Validitetsprøvning av psykososiala indexbildningar. In:
Hagberg, M., Hogstedt, C. (Eds.), Stockholmsundersøkningen 1.
Music Books, Stockholm, pp. 163–177.
Theorell, T., Emdad, R., Arnetz, B., Weingarten, A.M., 2001.
Employee effects of and educational program for managers at
an insurance company. Psychosom. Med. 63, 724–733.
Uhde, T.W., Bierer, L.M., Post, R.M., 1985. Caffeine-induced escape
from dexamethasone suppression. Arch. Gen. Psychiatry 42 (7),
737–738.
Ursin, H., 1988. Expectancy and activation: an attempt to systematize stress theory. In: Hellhammer, D., Florin, I., Weiner, H.
(Eds.), Neurobiological Approaches to Human Disease. Hans
Huber, Toronto, pp. 313–334.
Ursin, H., 2000. Psychosomatic medicine: state of the art. Ann.
Med. 32, 323–328.
Ursin, H., Eriksen, H.R., 2004. The cognitive activation theory of
stress. Psychoneuroendocrinology 29, 567–592.
van Dam, R.M., Willett, W.C., Manson, J.E., Hu, F.B., 2006.
Coffee, caffeine, and risk of type 2 diabetes. Diabetes Care
29, 398–403.
Von Thiele, U., Lindfors, P., Lundberg, U., 2006. Self-rated recovery
from work stress and allostatic load in women. J. Psychosom.
Res. 61, 237–242.
Ware, J.E., Gandek, B., IQOLA Project Group, 1994. The SF-36
health survey: development and use in mental health research
and the IQOLA Project. Int. J. Ment. Health 23 (2), 49–73.
Ware, J.E., Snow, K.K., Kosinski, M., Gandek, B., 2000. SF-36 Health
Survey: Manual and Interpretation Guide. QualityMetric Incorporation, Lincoln, RI.
Weitzman, E.D., Fukushima, D., Nogeire, C., Roffwarg, H.,
Gallagher, T.F., Hellman, L., 1971. Twenty-four hour pattern of
the episodic secretion of cortisol in normal subjects. J. Clin.
Endocrinol. Metab. 33 (1), 14–22.
Wüst, S., Wolf, J., Hellhammer, D.H., Federenko, I., Schommer, N.,
Kirschbaum, C., 2000. The cortisol awakening response—normal
values and confounds. Noise Health 2 (7), 79–88.
Zanoboni, A., Zanaboni Muciaccia, W., 1987. Effects of naloxone and
coffee on anterior pituitary hormones. Drugs Exp. Clin. Res. 13
(7), 443–446.
�
 Hege Eriksen
Hege Eriksen