Int Urol Nephrol (2011) 43:925–928
DOI 10.1007/s11255-011-0019-6
NEPHROLOGY – CASE REPORT
Acute kidney injury from pyelonephritis in an elderly man:
case report
Sayed Husain • Manaf Alroumoh •
Prince Mohan • Gabriel El-Kass •
Surya V. Seshan • Marilyn Galler
Received: 27 December 2010 / Accepted: 29 April 2011 / Published online: 8 July 2011
Ó Springer Science+Business Media, B.V. 2011
Abstract Pyelonephritis is rarely considered in the
differential diagnosis of acute kidney injury [1–5].
Acute non-obstructed bacterial pyelonephritis is an
infrequent and rarely considered cause of rapidly
progressive acute kidney injury. A diagnostic challenge thus develops as it is difficult to clinically
differentiate acute kidney injury secondary to ischemic or toxic acute tubular necrosis or papillary
necrosis versus acute interstitial nephritis secondary
to drugs or infectious pyelonephritis. We describe a
case of acute kidney injury due to suppurative
pyelonephritis in an elderly immunocompetent man
who presented with dysuria, vomiting, and fever and
later found to have histologic and radiologic proven
pyelonephritis as the cause of acute kidney injury in
the absence of hypotension, nephrotoxic agents,
non-steroidal analgesics, immunosuppression, urinary
tract obstruction, or other structural anomalies.
S. Husain (&) � P. Mohan
Department of Internal Medicine,
New York Hospital of Queens, NY, USA
e-mail: hus9007@hotmail.com
M. Alroumoh � G. El-Kass � M. Galler
Department of Nephrology,
New York Hospital of Queens, NY, USA
S. V. Seshan
Department of Pathology, New York-Presbyterian
Hospital and Weill Cornell Medical College,
New York, USA
The patient was managed with antimicrobial therapy,
hemodialysis, and a short course of corticosteroids.
Keywords
Pyelonephritis � Acute kidney injury
Case report
A 69-year-old man presented to the emergency
department of New York Hospital of Queens complaining of dysuria for 3 days with fever of 101°F/
38.3°C, chills, intermittent lower back pain, and
vomiting for 2 days with some loose bowel movements. He noted no change in his urine output,
hematuria, or rash. He denied analgesic use. His past
medical history included hypertension, gout, and mild
intermittent asthma for which he was taking Norvasc
5 mg, Lisinopril 5 mg, and Albuterol inhaler.
On admission, his blood pressure was 130/71 mm/
Hg, pulse 69/min, respiration 12/min, and oral
temperature 100.2 F/37.8°C. The patient was alert
and comfortable. His skin was without rashes, and
mucous membranes were moist. His lungs were clear
to auscultation, and heart sounds were normal sinus
rhythm without murmurs or rubs audible. His abdomen was obese with normal bowel sounds, nontender with no palpable masses. No costovertebral
angle tenderness was appreciated. His extremities had
1 ? peripheral edema.
Initial laboratory values were as follows: hemoglobin 13 mg/dL, hematocrit 38.1%, and platelet
123
�926
count 145,000/per cubic millimeter. The white cell
count was 30,600 per cubic millimeter with 40.9%
bands and 0% eosinophils. The metabolic panel showed
a sodium of 127 mmol/L, potassium 4.2 mmol/L,
chloride 91 mmol/L, bicarbonate 18 mmol/L, urea
nitrogen 59 mg/dL, creatinine 5.3 mg/dL, glucose
169 mg/dL, calcium 7.3 mg/dL, albumin 2.5 g/dL,
phosphorous 3.0 mg/dL, magnesium 2.2 mg/dL, lactic
acid 1.3 mmol/L, AST 55 IU/L, ALT 41 IU/L, and
ALP 89 IU/L. The urinalysis showed WBC of 1,529 per
high power field, RBC of 50 per high power field,
protein 500 mg/dL, nitrites negative, leukocyte esterase
positive, pH 5.5, and specific gravity 1.015.
Other laboratory findings revealed HIV, IPEP,
ANA, ANCA, rheumatoid factor, and hepatitis B and
C antigen and antibody to be negative and C3 and C4—
within normal range. Blood and urine specimens
collected on the day of admission were positive for
Escherichia coli (E. coli) 105 col/ml that was sensitive
to Cefepime and Levofloxacin. Random urine electrolytes were sodium 39 mmol/L, potassium 59.5 mmol/
L, chloride 24 mmol/L, osmolality 306 mosm/kg,
creatinine 179 mg/dL, protein 336 mg/dL, and a urine
protein creatinine ratio (UPC) of 1.0 urine. Wright
stain was positive for eosinophils.
A renal sonogram showed the right kidney measuring 13 cm and the left kidney 12.5 cm. There was
no hydronephrosis, renal stones, or masses. A noncontrast CT of the abdomen and pelvis showed
bilateral perinephric and periureteral fat stranding
of uncertain significance without hydronephrosis or
nephrolithiasis. The prostate gland measures 4.7 cm
in transverse dimension.
At the time of admission, the patient was started
on aggressive hydration and Lisinopril was discontinued as prerenal azotemia was in the differential
for acute kidney. Empiric antibiotic treatment with
Vancomycin and Levaquin was started, and later
was changed to Cefepime according to the culture
and sensitivity results. Repeat urine culture on the
4th day of admission was negative and the urinalysis
on the 10th day of admission showed improvement
in the WBC count to 134 per high power field.
Despite hydration and appropriate antibiotic therapy,
the patient’s blood urea nitrogen and creatinine
continued to trend upward to 158 mg/dL and
10.9 mg/dL, respectively. The patient was nonoliguric. On the 5th hospital day, he was started
on hemodialysis. A renal biopsy was performed on
123
Int Urol Nephrol (2011) 43:925–928
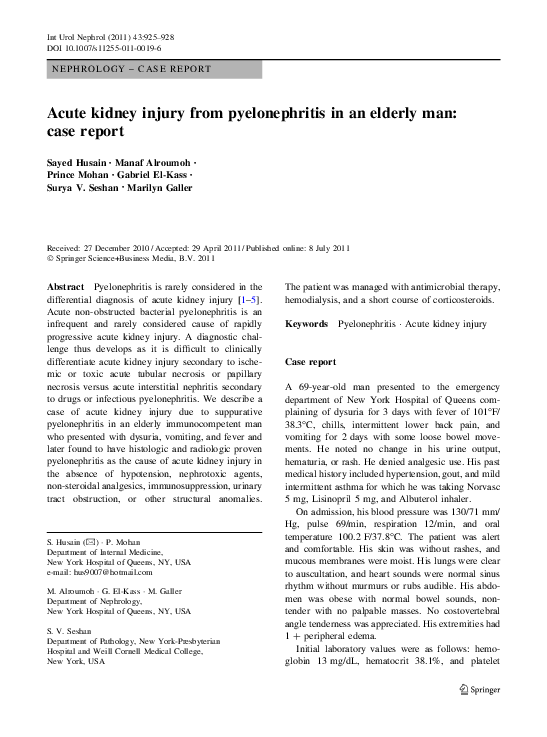
Fig. 1 Renal cortical tissue showing diffuse, active and focal
subacute inflammation, interstitial edema, and inflammatory cell
casts within the tubules. Most of the tubules show evidence of
tubular cell injury, focal sloughing of the lining cells. No
significant changes are noted within the glomerulus (H&Ex100)
the 9th day of hospitalization once his urine culture
was negative.
The biopsy showed diffuse active and chronic
pyelonephritis, moderate to severe; minimal glomerular changes diffuse tubular injury with inflammatory
cell casts, focal tubular atrophy with minimal interstitial fibrosis, and no microabscesses (Fig. 1).
The findings were consistent with E. coli associated
urinary tract infection with involvement of the renal
parenchyma.
After three hemodialysis treatment sessions, the
interdialytic urea nitrogen and creatinine levels began
to decline indicating improvement in his endogenous
renal function. Hemodialysis was discontinued on day
11 when his creatinine level was stable at 6.3 mg/dL.
Three days after the last hemodiaylsis treatment, the
patient developed an attack of Gout and was started on
a course of prednisone 60 mg/day for a total of 3 days.
His urea nitrogen and creatinine continued to slowly
improve and on the day of discharge, day 19 of his
hospitalization, his urea nitrogen was 66 mg/dL and
creatinine 3.73 mg/dL. The patient was prescribed an
outpatient course of Cefepime 500 mg IV BID for
1 week followed with Levaquin 250 mg PO QD for
7 days per ID recommendation. Three weeks post
discharge, he was seen in follow up at which time
he was well, afebrile, without dysuria, back pain, or
associated constitutional symptoms. His urea nitrogen
level was 34 mg/dL and creatinine of 2.9 mg/dL.
Six weeks postdischarge, his urea nitrogen level was
�Int Urol Nephrol (2011) 43:925–928
31 mg/dL and creatinine 1.8 mg/dL, and 8 months
postdischarge, his creatinine improved to 1.4 mg/dL.
Discussion
Acute bacterial pyelonephritis is a rare and unusual
cause of acute kidney injury in patients without any
evidence of anatomical anomaly or other predisposing factors. It has been described more often in the
pediatric population [6] but less frequently seen in the
adult population, reported at an incidence of 2–3%
[6, 7]. Most of the patients had some predisposing
conditions such as the presence of an indwelling
catheter, use of immunosuppressives, pregnancy, renal
stones, solitary kidney, or non-steroidal analgesic use.
A review of the literature showed 16 cases of
biopsy proven acute kidney injury secondary to acute
bacterial pyelonephritis. Most patients showed interstitial and peritubular inflammation with polymorph
neutrophils and microabcesses. There was no evidence of obstructive uropathy or vasculitic changes.
In some of the cases, toxicity was associated with non
steroidal anti-inflammatory drugs (NSAIDS) and
alcohol (ETOH) use. Both chronic and acute moderate alcohol use can increase host susceptibility to
infections caused by bacterial pathogens due to
impairment of host defense and cellular immune
responses [8]. Of the 16 cases, 13 were due to E. coli
and two due to Klebsiella pneumoniae. Only one
patient showed no growth on culture. Prompt diagnosis with antibiotic coverage had a favorable effect
on the prognosis of pyelonephritis-induced acute
kidney injury in most of the patients. However, three
died from pyelonephritis and two required hemodialysis [9–19]. A severe form of pyelonephritis,
emphysematous pyelonephritis, is characterized by
gas within the renal parenchyma and/or the collecting
ducts. Khair et al. described 19 cases of emphysematous pyelonephritis and noted that diabetes, female
gender, and poor glycemic control were risk factors
for this disease. Eighteen of 19 patients required
dialysis, and 13 of the 15 patients who survived had
renal recovery and dialysis discontinuation. No renal
pathology was described [20].
Xanthogranulomatous pyelonephritis is a rare
chronic inflammatory condition that is characterized
by destruction and replacement of renal parenchyma
with lipid laden macrophages causing poor functioning
927
or non-function of the affected kidney. Patients can
present with typical symptoms of bacterial pyelonephritis and renal impairment beyond expected with one
diseased non-functioning kidney [21].
This case was a diagnostic challenge to the renal
team as there was no history of prior renal dysfunction, radiologic evidence for Xanthogranulomatous or
Emphysematous pyelonephritis, urologic anatomical
abnormalities, nephrotoxic agent exposure, or hypotension, and was occurring in an immunocompetent
host with a negative serological work up and positive
blood and urine cultures for E. coli. Despite prompt
treatment with hydration, discontinuation of the
angiotensin converting enzyme inhibitors (ACEI)
and appropriate antibiotics, the patient’s renal function continued to worsen necessitating the initiation
of hemodialysis. Due to the unusual severity of the
renal impairment and the prolonged course of acute
kidney injury, a renal biopsy was performed for
diagnosis and treatment confirmation. It was possible
that acute tubular necrosis secondary to a gram
negative infection without hypotension caused the
acute kidney injury secondary to cytokine and
endotoxins stimulation leading to vasoconstriction
and mesangial cell contraction. However, the biopsy
report was more compatible with acute bacterial
pyelonephritis.
Gradual recovery of our patient’s renal function
occurred over weeks with appropriate antibiotic
therapy. The infection was cleared as evident by
urine and blood culture negativity and improvement
of the urinalysis. Several reports have shown more
complete recovery of renal function and decreased
renal scarring in severe acute pyelonephritis when
steroids were added to the anti-microbial therapy.
We do not think that the incidental addition of
prednisone in our patient contributed to the renal
recovery. The patient’s renal function began to
recover and dialysis was discontinued prior to the
initiation of only 3 days of steroid therapy. Furthermore, postdiscontinuation of steroids, his renal function continued to improve.
This case report emphasizes that physicians should
consider acute bacterial pyelonephritis in the differential diagnosis of acute renal failure. Since this
disease entity may cause permanent renal damage, it
is crucial to promptly begin appropriate and adequate
anti-microbial treatment to prevent the long-term
consequences of renal scarring.
123
�928
References
1. Baker LRI, Cattell WR, Fry IKF, Mallinson WJW (1979)
Acute renal failure due to bacterial pyelonephritis. Q J Med
48:603–612
2. Woolley PD, Wyman A, Nicholls AJ, Shortland JR, Brown
CB (1986) Acute renal failure due to bacterial pyelonephritis. Br J Urol 58:733
3. Greenhill AH, Norman ME, Cornfield D, Chatten J, Buck
B, Witzleben CL (1977) Acute renal failure secondary to
acute pyelonephritis. Clin Nephrol 8:400–4034
4. Thompson C, Verani R, Evanhoff G, Weinman E (1986)
Suppurative bacterial pyelonephritis as a cause of acute
renal failure. Am J Kidney Dis 8:271–273
5. Turney JH, Marshall DH, Brownjohn AM, Ellis CM,
Parsons FM (1990) The evaluation of acute renal failure,
1956–1988. Q J Med 74:83–104
6. Turner ME, Weinstein J, Kher K (1996) Acute renal failure
secondary to pyelonephritis. Pediatrics 97:742–743
7. Baker LR, Cattell WR, Fry IK, Mallinson WJ (1979) Acute
renal failure due to bacterial pyelonephritis. Q J Med
48:603–612
8. Szabo G, Mandrekar P (2009) A recent perspective on
alcohol, immunity, and host defense. Alcohol Clin Exp Res
33(2):220–232
9. Nahar A, Akom M, Hanes D, Briglia A, Drachenberg CB,
Weinman EJ (2004) Pyelonephritis and acute renal failure.
Am J Med Sci 328(2):121–123
10. Jones SR (1992) Acute renal failure in adults with
uncomplicated acute pyelonephritis. Clin Infect Dis
14(1):243–246
11. Kooman JP et al (2000) Acute pyelonephritis: a cause of
acute renal failure Neth J Med 57(5):185–189
123
Int Urol Nephrol (2011) 43:925–928
12. Nunez JE, Perez E, Gunasekaran S, Narvarte J, Ramirez G
(1992) Acute renal failure secondary to acute bacterial
pyelonephritis. Nephron 162(2):240–241
13. Trivedi HL, Kumar S, Minielly JA (1977) Renal cortical
microabscesses as cause of reversible acute renal failure.
Urology 9(2):177–179
14. Adler SN (1978) Nonobstructive pyelonephritis initially
seen as acute renal failure. Arch Intern Med 138(5):816–817
15. Woolley PD, Wyman A, Nicholls AJ, Shortland JR, Brown
CB (1986) Acute renal failure due to bacterial pyelonephritis. Br J Urol 58(6):733
16. Olsson PJ, Black JR, Gaffney E, Alexander RW, Mars DR,
Fuller TJ (1980) Reversible acute renal failure secondary
to acute pyelonephritis. South Med J 73(3):374–376
17. Woodrow G, Patel S, Berman P, Morgan AG, Burden RP
(1993) Asymptomatic acute pyelonephritis as a cause of
acute renal failure in the elderly. Postgrad Med J69(809):
211–213
18. Kuiper JJ (1993) Group III acute bacterial pyelonephritis.
Am J Med 95:450–451
19. Jones BF, Nanra RS, Grant AB, Ferguson NW, White KH
(1989) Xanthogranulomatous pyelonephritis in a renal
allograft: a case report. J Urol 141(4):926–927
20. Khaira A, Gupta A, Rana DS, Gupta A, Bhalla A, Khullar
D (2009) Retrospective analysis of clinical profile prognostic factors and outcomes of 19 patients of emphysematous pyelonephritis. Int Urol Nephrol 41(4):959–966
[Epub 2009 Apr 30]
21. Kuo CC, Wu CF, Huang CC, Lee YJ, Lin WC, Tsai CW,
Wu VC, Chen YM, Wu MS, Chu TS, Wu KD (2010)
Xanthogranulomatous pyelonephritis: critical analysis of
30 patients. Int Urol Nephrol Jun 11
�
 Prince Mohan
Prince Mohan