437
L. monocytogenes Brain Abscesses in Pediatrics
4. Gellin BG, Broome CV. Listeriosis.JAMA 1989,261, 131%1320.
without isolation and identification of the causative agent [ 11.
5. Fleming DW, Cochio SL, MacDonald KL, ef al. Pasteurized milk
This is particularly important in light of the poor intrinsic
as a vehicle of infection in an outbreak of lister. N EnglJ Med
activity of the cephalosporins and of the lack of intracerebral
1985,312,404-407.
6. Linnan MJ, Mascola L, Xiao DL, et a/. Epidemic listeriosis
penetration of the aminoglycosides, a combination that is curassociated with Mexican-style cheese. N EnglJ Med 1988, 319,
rently used as empirical treatment of fever and suspected
823-828.
infection in neutropenic cancer patients. Optimal treatment of
7. Schlech WF, Lavigne PM, Bortolusse R, et al. Epidemic listeriosis:
listerial infections remains controversial. A combination of
evidence for transmission by food. N Engl 3 Med 1983, 308,
ampicillin and gentamicin is generally recommended, but other
203-206.
8. Hantel A, Dick JD, Karp JE. Listeriosis in the setting of malignant
options are possible, including cotrimoxazole, rifampin and
disease. Changing issues in an unusual infection. Cancer 1989, 64,
vancomycin [4].
51&520.
L.
In conclusion, the occurrence of brain abscesses due to zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFED
9. Khardori N, Berkey P, Hayat S, Rosenbaum B, Bodey GP.
monocytogenes in this 6-year-old girl should alert pediatricians
Spectrum and outcome of microbiologically documented Listeria
against this entity. Despite the severity of the clinical course,
monocytogenes infections in cancer patients. Cancer 1989, 64,
1968-1970.
this infection was treated successfully without any neurological
Viscoli C, Van der Auwera P, Meunier F. Gram-positive infections
10.
sequela and did not preclude the continuation of the antineoplasin granulocytopenic patients: an important issue? 3 Antimicrob
tic treatment, including allogeneic bone marrow transplantation.
Chemother 1989,21,149-156.
11. Armstrong D, Polsky B. Central nervous system infections in the
compromised host. In: Rubin LH, Young LS. ClinicalApproach to
Infections in the Compromised Host, 2nd ed. New York, Plenum
1. Dee RR, Lorber B. Brain abscess due to Listeria monocytogenes:
Medical, 1988,165-191.
Rev InfectDis 1986,8,968-977.
case report and literature review. zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
12. Oren-Harris J, Marquez J, Swerdloff MA, Magana IA. Listeria
2. Pollock SS, Pollock TM, Harrison MJG. Infection of the central
brain abscess in the acquired immunodeficiency syndrome. Arch
nervous system by Listeria monocytogenes: a review of 54 adult and
Neurol 1989,46,250.
juvenile cases. QJ Med 1984,53,331-340.
13. Ochs J, Mulhern RK. Late effects ofantileukemic treatment. Pediat
3. Dykes A, Baraff LJ, Herzog P. Listeria abscess in an immunocomClin North Am 1988,35,815-834.
promised chi1d.J Pediaa 1979,94,72-74. zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
Eur J
Pnnt ed
Cancer ,
m Gr eor
Vol.
27,
No.
4 , pp.4 374 4 1,
0277-5379191$3.00
1991
0
Bnmn
1991
Pqamm
i
0.00
lJrerrpk
Postremission Chemotherapy in Adult Acute Nonlymphoblastic Leukaemia Including Intensive or
Non-intensive Consolidation Therapy
Monica Giordano, Albert0 Riccardi, Margherita Girino, Silvia Brugnatelli,
Paolo Scivetti, Renata Luoni, Rosangela Invernizzi and Edoardo Ascari
From October 1983 to December 1988, 84 consecutive adult patients with acute non-lymphoblastic leukaemia
(ANLL; median age = 51 yr) were uniformly treated to induce remission (CR) with intravenous vincristine and
cytarabine sequentially followed by daunomycin and infusion cytarabine. From October 1983 to December 1985
consolidation was non-intensive (2 courses with the same drugs used for induction) (protocol ANLL83: 27
patients, median age = 45). From January 1986 to December 1988 consolidation was intensive (4 courses of
vincristine and cytarabine sequentially followed by etoposide plus thioguanine or amsacrine) (protocol ANLL86:
57 patients, median age = 57). Excluding early deaths, the CR rate was 71.6%. Median CR, responsive patient
survival and overall survival were 11.1, 15.3 and 8.5 mo, respectively. For protocol ANLL83 and ANLL86,
median CR was 8.7 and 13.2 mo (P < 0.05) and median survival was 13.1 and 16.9 mo (P < 0.05) for responders
and 8.0 and 9.2 mo (Pnot significant) for all patients. Intensive consolidation including drugs not previously used
for induction seems to prolong CR duration and responder survival in adult ANLL.
EurJ Cancer, Vol. 27, No. 4, pp. 437441,
1991
INTRODUCTION
induction can be used or new cytostatics may be added) and
A zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
WAY OF administering
postinduction therapy to adult acute
their dosage [ 11. The prerequisites which define a consolidation
non-lymphoblastic leukaemia (ANLL) patients after remission
course as being intensive or non-intensive are not clear-cut but,
(CR) is consolidation therapy, where short intensive cyclic
as a guideline, an intensive course should produce, in a CR
therapy is given for 3-6 months and may be followed or not by patient, heavy cytopenia, i.e white blood cell (WBC) count of
maintenance [l]. For consolidation, options can be made for less than 1.0 x lo911and a platelet count of less than 50 x lo911
both the choice of drugs administered (only those employed for
about 2 weeks following its completion [2].
�M. Giordano zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDC
et al.
In this paper we report data on a treatment program for
ANLL which was started in 1983 [3]. Induction treatment was
the same for all patients. In the first group of CR patients,
consolidation was non-intensive and employed the same drugs
used for induction. In patients treated subsequently, consolidation was intensive and employed cytostatics that were not
used for induction. Intensive consolidation apparently resulted
in increased CR and responder survival duration.
as in the induction course, and followed by etoposide (100
mg/mzlday by 2 h intravenous infusion) plus thioguanine (100
mglm?day orally) for 5 days (1st and 3rd course) or by amsacrine
(60 mg/m’ by 2 h intravenous infusion) on day 5 (2nd and 4th
course).
Post-consolidation
treatment
After consolidation, patients of protocol ANLL83 were given
a 1.5-year maintenance regimen in which different cytostatics
MATERIALS AND METHODS
were given every 4-6 weeks in order of circumventing drug
Patients zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
resistance in residual leukaemia [6, 71. The following drugs and
84 consecutive untreated ANLL patients entered this prospecdrug combinations were used: TRAP (courses 1,6 and 11) [6],
tive, non-randomised
study between October 1983 and
VP 16 213 (150 mg/m2/day intravenously, days 1 to 5, courses
December 1988 (Table 1). No patient with a diagnosis of AL
2,7 and 12), POMP (course 3) [6], cytarabine plus thioguanine
was excluded due to advanced age or history of preleukaemia (8 (cytarabine 100 mg/m2/12 h intravenous plus 6-TG, 100
patients). Median age was 51 (range 16-78) and the male:female
mg/m2/day orally, days l-5, courses 4,9 and 14), COAP (courses
ratio was 45:39. Distribution of FAB subtypes was as follows:
5, 10 and 15) [6], Iomustine (80 mg/m* orally, day 1, course 8)
Ml: 12 patients; M2: 14; M3: 14; M4: 30; M5: 10; M6:2; and
and cyclophosphamide (1 g/m2/day by 2 h intravenous infusions,
M7:2. Chromosomal abnormalities were found in 10 patients
days 1 and 2, course 13).
[translocation 8/21,2 cases; trisomy 8, 3 cases; monosomy 7, 2
The CR patients of protocol ANLL86 were randomised to
cases; trisomy 11, 1 case; inv 16 (~13 q22), 1 case; and lq+, 1 receive or not receive the above maintenance program.
case].
Supportive measures
Cytostatic treatment
For all patients, two courses of induction
treatment were planned at a 14-21 day interval. The induction
course was derived from previous in vivo data, indicating that the
intravenous push administration of vincristine and of moderate
dose cytarabine increased the tritiated thymidine labelling index
in most patients with AL, i.e. synchronised blasts in S phase [4,
51, and this, in turn, increased the effectiveness of a sequentially
administered anthracycline in reducing the peripheral blood
blasts [4].
In each course, patients initially received vincristine (2 mg
intravenously on day 1) and cytarabine (75 mg/m*/l2 h directly
intravenously from day 1 to 4). Daunomycin (80 mg/m2
intravenously) was then given on days 5 and 7, and cytarabine
(200 mg/m2/day by continous infusion) on days 6 and 7. A bone
marrow (BM) aspirate and/or biopsy was performed 10-14
days after each course. Complete remission was defined as
disappearance of BM blasts with normal haematological values
(granulocytes > 1.5 x 109/1,platelets > 100 X 109/1and haemoglobin > llgldl) maintained for at least 1 month without
transfusions. Partial remission was not used as a criterion for
defining response.
Induction therapy.
These measures did not change throughout the whole study
period and have been reported in a previous paper [3].
Result analysis
Remission duration is calculated from the data of CR to the
data of relapse. Survival is calculated from the start of therapy.
Survival and remission curves were constructed according to
the method of Berkson and Gage [8] and analysed with the
Lee-Desu procedure [9].
RESULTS
No patient in our series had bone marrow transplantation.
The results obtained are summarised in Tables 1 and 2 and Figs
1 and 2.
CR rate
Table 2 furnishes the CR rates according to the categories of
patients included in the evaluation. Excluding patients who died
(due to consequences of cytopenia, i.e haemorrhage and/or
infection) before starting chemotherapy or before completing
induction, 48/67 (71.6%) patients achieved CR. Of 19 patients
Consolidation therapy
The CR patients recruited between November 1983 and
December 1985 (protocol ANLL83) received non-intensive
consolidation with 2 courses of the same drugs and with the
same drug sequencing used for induction (but with only one
dose of both daunomycin and infusion cytarabine, on day 5).
The CR patients recruited between January 1986 and
December 1988 (protocol ANLL86) received intensive consolidation using 4 courses, including cytostatics not used for induction. In each consolidation course, these new drugs were given
sequentially to vincristine and cytarabine, as in the induction
course. In practice, vincristine and cytarabine were scheduled
Correspondence to A. Riccardi.
The authors are at the Clinica Medica II, Dipartimento di Medicina
Interna e Teraoia Medica. Universiti di Pavia and Istituto di Ricovero e
Cura a Caratteie Scientifico Policlinico S. Matteo, 27100 Pavia, Italy.
Revised 11 Sep. 1990; accepted 13 Sep. 1990.
Table
1. M ain clinical characteristics of the studied population
Protocol
No. of patients
M/F
ANLL83 + ANLL86
ANLL83
ANLL86
I’
84
27
57
45139
15112
30127
NS
NS
Median age, yr
(range)
51
(16-78)
(lfz7!
57
(20-78)
FAB subtypes
M,IM,IM,
M,IM,IM,IM,
12114114
30/10/2/2
41416
814/O/l
8/10/8
NS
2216/211
All patients were treated to induce remission (CR) with sequential
vincristine, arabinosylcytosine and daunomycin. Patients on Protocol
ANLL83 and ANLL86 received non-intensive and intensive consolidation therapy, respectively.
�Consolidation Therapy in Adult Acute Non-lymphoblastic
439 zyxwvutsrqpon
Leukaemia
Table 2. Remission rates according with exclusion criteria
ANLL83
+ ANLL86
No.
Protocol
CR
%
-
ANLL83
ANLL86
No.
No.
CR
%
CR
All entered patients
48184 57.1
15127 55.5
33157 57.8
48178 61.5
48/67 71.6
48159 81.3
15124 62.5
15120 75.0
15116 93.7
33154 61.1
33147 70.2
33143 76.7
CR following 1st course
36148 74.6
llil5
25133 76.0
A = not treated (6 patients = 7.1%); B = early deaths (11 patients =
13.0%); C = previous myelodysplasia and/or treatment (8 patients =
9.5%).
who failed to achieve CR, 2 died from haemorrhage and/or
infection during BM aplasia and 17 had resistant disease. There
were no differences in CR rate between protocols ANLL83 and
ANLL86 and the 75% of responsive patients achieved CR
following the first course.
Among patients who completed induction, patients aged less
than the median age (43 and 54 yr for protocols ANLL83 and
ANLL86, respectively) had CR rates greater than older patients
(for protocol ANLL83, 60 and 90%, respectively, and for
protocol ANLL86 58.3 and 82.6%). No difference in CR
duration was seen depending on responsive patient age.
CR duration
Median CR was 11.1 months for all patients. It was 8.7
months for the 15 CR patients of protocol ANLL83 (who
received non-intensive consolidation with the same drugs used
for induction) and 13.2 for the 33 patients of protocol ANLL86
(who received intensive consolidation with cytostatics other than
those used for induction) (P < 0.05) (Fig. 1). 7115 CR patients
on protocol ANLL83 and 18133 CR patients on protocol
ANLL86 relapsed before completing consolidation. No difference in CR duration has been seen so far for the remaining 15
protocol ANLL86 patients depending whether they received (7
patients) or did not receive (8 patients) maintenance.
-
Protocol
ANLL83,
Protocol
ANLL86,33
15
ANLL83,
15 ptients
Protocol
ANLL86,
33patients
P-CO.05
%
With exclusion
A
A+B
A+B+C
73.0
Protocol
potlents
0
-I
.
I
IO
Respnsw
I
20
.
patients
1
30
surwval
I
1
40
50
(mo)
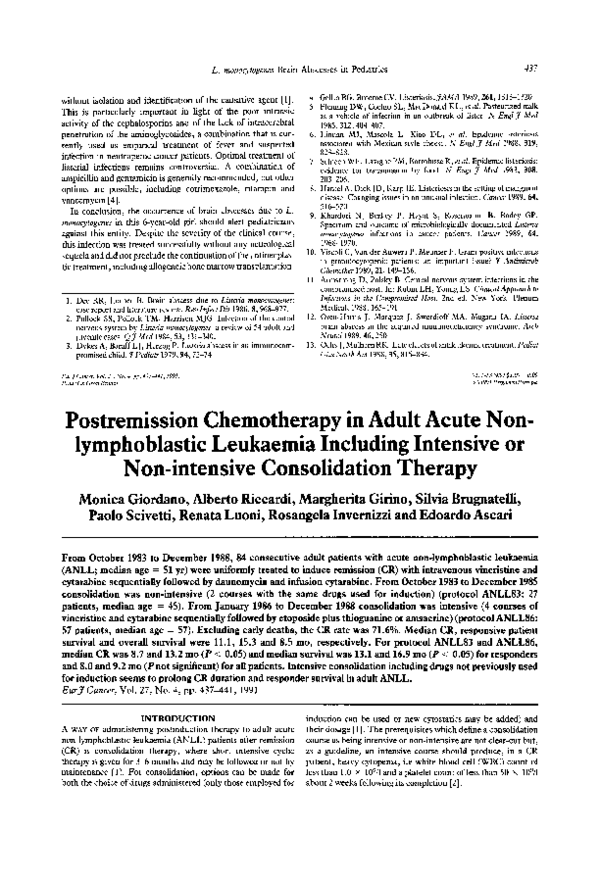
Fig. 2. Duration of responsive patient survival according with consolidation therapy (numbers indicate patients at risk).
Survival
56167 patients who completed induction (18120 of protocol
ANLL83 and 38147 of protocol ANLL86) have died. Median
survival was 8.5 months for all patients who had been treated
(including early deaths) and 15.3 months for those who had
responded to therapy. No difference in overall survival is seen
between protocol ANLL83 and ANLL86. Responsive patients
of protocol ANLL86 had a longer median survival (16.9 months)
than those of protocol ANLL83 (13.1 months) (P < 0.05) (Fig.
2).
Toxicity
Fever >38”C following the first course was present in 48/67
cases who completedinduction. The nadir of WBC (0.4 x 10’11)
was reached on day 10 following the end of treatment (WBC
were < 0.5 x 10’11for a median time of 13 days), and the nadir
of platelets (20 x 10’11)was reached on day 14 following the
end of treatment (platelets were < 50 x 10’11for a median time
of 16 days). Both fever and haematological toxicity were less
severe during the second course.
As expected, toxicity during consolidation was mild for protocol ANLL83 and quite severe for protocol ANLL86. In protocol
ANLL83, only an occasional consolidation course gave granulocyte counts CC1.0 x 10’11and/or platelet counts < 50 x 10v/l,
while in protocol ANLL86 (where 4 courses of more aggressive
therapy were administered) 68% of CR patients had these low
values at least one time during consolidation (the cytopenia
phase lasted a median time of 5 days); 48% had them twice and
the 21% for three or four times. Accordingly, both fever and
requirements for supportive therapy were much more frequent
in protocol ANLL86 than ANLL83. However, no patient died
due to complications related to consolidation-induced cytopenia.
patients
DISCUSSION
The presented data suggest that intensive consolidation following CR results in increased CR and responder survival
duration of ANLL adult patients.
Induction results indicate that the induction schedule we used
was well tolerated and effective in inducing CR. Excluding
patients who died before or while in induction due to cytopenia
(more probably related to leukaemia than to treatment-induced
aplasia) (Table 2) [lo], the 13.0% early deaths is acceptable
lb zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
0
2b
3b
4b
5b
Re m ~w o n
im o ) zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
during induction for adult AL. The 71.6% CR rate among
patients who completed induction compares well with the CR
Fig. 1. Remission duration according with consolidation therapy,
rates obtained in recent investigations [ 11. This is especially true
that was non-intensive in protocol ANLL83 and intensive in protocol
ANLL86 (numbers indicate patients at risk).
if we consider that the median age is higher in our study (5 1 yr)
PC005
�440
M. Giordano zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGF
et al.
than in most reported series, and that median age is a parameter
with a strong influence on the CR rate [ 11.
Sequencing vincristine, cytarabine and daunomycin for induction was based on previous in vivo cytokinetic data, indicating
that cytostatics have increased effectiveness when administered
at the time of S-phase synchronisation induced by vincristine
and medium dose cytarabine [4], an effect similar to that
reported in in vitro experiments using colony stimulating factors
(CSFs) before chemotherapy [ 1 I]. The good effectiveness of this
drug schedule in this quite large series supports that cytokinetic
based protocols are useful for inducing CR in AL, although this
issue is still unresolved. In fact, some investigations have
reported CR advantages in administering cytostatics at time of
S-phase blast synchronisation or recruitment [12-171 but this is
not confirmed in other studies [18-191 and a definite confirmation through randomised studies is lacking.
For the first 15 responsive patients consolidation was nonintensive and used only the same drugs (vincristine, cytarabine
and daunomycin) already employed for induction. In the 33
patients who responded subsequently, consolidation was intensive and contained also cytostatics (etoposide; thioguanine and
amsacrine) that were not previously employed. Although this
was not a randomised study, intensive consolidation resulted in
increased CR and responder survival duration (both induction
treatment and supportive measures were the same throughout
the whole study).
There is no consensus in the literature on the best postremission policy [l, 201. Our data are in keeping with those
from two large randomised studies, in which increasing the
amount of therapy given for both induction and consolidation
[21] or using for consolidation cytostatics other (high dose
cytarabine and/or amsacrine and/or 5-azacytidine) than those
(cytarabine and daunomycin) employed for induction [22] have
prolonged CR and survival duration. However, there are reports
contrasting these data, that were reviewed in detail elsewhere
[l]. As an example, the advantages of using new drugs for
consolidation (including high-dose cytarabine) [23, 241 has been
questioned and those of greatly increasing the drug dosage (with
BM transplantation rescue) are still not demonstrated [25].
Another example is that administering consolidation before
maintenance with the same drugs (cytarabine plus daunomycin
plus thioguanine) used for induction is not superior to maintenance alone [26].
These widely contrasting personal and literature data hamper
the belief that an empirically devised postinduction chemotherapy in ANLL is crucial in improving the final prognosis of
this disease, i.e. patient survival. Obtaining a better quality CR
is probably more advantageous. Since no other conventional
cytostatic regimen is more effective than cytarabine and anthracyclines in inducing CR, there are two possible ways for lowering
residual disease at CR. First, using granulocyte (and/or
granulocyte-macrophage)
CSFs as normal haemopoietic cell
rescue can allow to increase the doses of cytarabine and anthracyclines given for induction [27, 281. A prerequisite for this
approach is that it must be definitely proved that culture studies
on individual patient cells [ 11, 29, 301 can definitely exclude
that these stimulating factors also increase blast regeneration.
Second, the best way of administering
cell cycle-specific or
aspecific drugs to lower residual leukaemia could be based on
knowing the relative aliquots of in- and out-of-cycle blasts.
Exploiting pretreatment
kinetic differences in the individual
ANLL patient can now be done using the in viva bromodeoxyuri-
dine [31] and flow cytometry and the Ki-67 monoclonal antibody
[32, 331 techniques.
1. Riccardi A, Giordano M, Girino M. Treatment of adult acute non
lymphoblastic leukemia: a computer aided analysis. Haemacologica
1987,72,71-78.
2. Zittoun A (for the EORTC Leukemia-Lymphoma group). High
dose cytosine arabinoside plus AMSA for reinduction or consolidation maintenance in acute myelogenous leukemia. In: Hagenbeek
A, Lowenberg B. eds. Minimal Residual Disease in Leukemia.
Dordrecht, Martinus Niihoff. 1986.159-166.
3. Riccardi A, Invernizzi R, Girino fi, et al. Sequential vincristine,
arabinosylcytosine and daunomycin induction therapy in adult acute
leukemia. Haematologica 1986,71,129-133.
4. Riccardi A, Mazzini G, Montecucco CM, et al. Sequential vincristine, arabinosylcitosine and adriamycin in acute leukemia: cytologic
and cytokinetic studies. Cytometry 1982,3,104-109.
5. Montecucco CM, Riccardi A, Cresci R, Mazzini G, Ascari E.
Cytokinetic changes in the peripheral blood of leukemic patients
during cytostatic therapy. Effect of arabinosylcytosine. Bus Appl
Histochem 1980,24,423-434.
6. Spiers ASD. Chemotherapy of acute leukemia. Clin HematoZ1972,
1,144-155.
7. Buchner T, Urbanitz D, Hiddemann W, et al. Intensified induction
and consolidation with or without chemotherapy for acute myeloid
leukemia (AML): two multicenter studies of the German AML
Cooperative Group.J Clin Oncoll985,2,1583-1589.
8. Berkson J, Gage RI’. Calculation of survival rates for cancer. Proc
StaffMeetingMayo
Clin 1950,25,270-280.
9. Lee TE, Desu MM. A computer program for comparing K samples
with right-censored data. Comput Programs Biomed 1972, 2,
315-322.
10. The Toronto Leukemia Study Group. Results of chemotherapy for
unselected patients with acute myeloblastic leukemia: effect of
exclusion on interpretation of results. Lancet 1986,786-788.
11. Giordano M, Pedrazzoli P, Danova M, et al. Modulation of leukemic
cell proliferation by haemopoietic growth factors and cytosine
arabinoside (Ara-c) (abstr.). XIV International Conference on Analytical Cytology 1990,108.’
12. Vaughan WP, Karp JE, Burke PJ. Long chemotherapy free
remission after single cycle timed sequential chemotherapy for acute
myelocytic leukemia. Cancer 1980,45,85%865.
13. Dahl GV, Kalwinsky DK, Murphy S, et al. Cytokinetically based
induction chemotherapy and splenectomy for childhood acute non
lymphocytic leukemia. Blood 1982,60,856863.
14. Saponara BS, Rothemberg SP, Villamena D. Cytarabine and thioguanine for acute non lymphocytic leukemia. A new look. Arch Intern
Med 1984,139,1277-1290.
Biichner T, Kamanbroo D, Urbaniz D, Hiddenman W, van de
Loo J. Induktionsbehandlung der akuten myeloischen leukamie
mit cytosin arabinosid daunorubicin, zusazlicher effekt von ifosfamid und vincristin. Blut 1978,36,371-376.
16. Kremer WB, Vogler WR, Chang YK. An attempt at synchronization of marrow cells in acute leukemia. Cancer 1976,37,390-403.
17. Lampkin BC, McWilliams NB, Mauer AM, Flessa HC, Hake DA,
Fish& V. Manipulation of the mitotic cycle in the treatment of
acute mveloeenous leukemia. Br 7 HaematoZ1976,32.29-40.
18. MacKiiney-AA, Flynn B. Cytoine arabinoside modulation of the
mitotic cycle in the treatment of adult acute leukemia. Am J
15.
Haematol1979,5,93-99.
19.
Sutow VW, Thomas D, Stauber CP, et al. Study of cytosine
arabinoside (NSC-63878) plus vincristine (NSC-67574) prednisone
(NSC-1023) and L-asparaginase (NSC-109229) for remission induction in advanced acute leukemia in children. Cancer Treat Rep 1976,
60,591-594.
Lichman MA, Henderson ES. Acute mylogenous leukemia. In:
Williams WT. Bentler E. Ersler Al, Lichman MA eds. HematoloayNew York, &Craw-Hill, 1990,2ji-272.
21. Bell R, Rohatiner AZS, Slevin ML, et al. Short-term treatment for
acute myelogenous leukemia. Br Med 3 (Clin Res) 1982, 284,
1221-1224.
22. Winton EF, Vogler WR, Raney M. A randomized trial of postinduction theraov for acute mveloblastic leukemia (AML) (abstr.). Blood
1985,66, &ppl. l), 2lia.
23. Weiner RS, Raney M, Elfenbein GJ, et al. Treatment of residual
20.
�Consolidation
24.
25.
26.
27.
28.
29.
Therapy
in Adult Acute Non-lymphoblastic
441
Leukaemia
I. Growth regulation of acute myeloid leukemia (AML) (abstr.)
disease in AML: interim of analysis of a Southeastern Cancer Study
Haemarologica 1988,?3 (Suppl), 17.
Group prospective randomized clinical trial. In: Hagenbeek A,
30. Clutterbuck R, Newman AA, Powles R, er al. Failure to immortalize
M inimal Residual Disease in Leukemia. DordLowe&erg B. eds. zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
human AML cells using human recombinant GM-CSF in vitro and
recht, Martinus Nijhoff, 1986,167-179.
in vivo. Bone Marrow Transpll989,4,
(Suppl.), 40.
Zittoun R (for the EORTC Leukemia-Lymphoma Group). High
31. Riccardi A, Danova M, Wilson G, et al. Cell kinetics in human
dose cytosine arabinoside plus Amsa for reinduction or consolidation
malignancies studied with in vivo administration of bromodeoxyurimaintenance in acute myelogenous leukemia. In: Hagenbeek A,
dine and flow cytometry. Cancer Res 1988,48,6238-6245.
Lowe&erg B, eds. M inimal Residual Disease in Leukemia. Dord31. Riccardi A, Danova M, Wilson G, et al. Cell kinetics in human
recht, Martinus Nijhoff, 1986,159-166.
malignancies studied with in vivo administration of bromodeoxyuriMayer RJ. Chemotherapy versus allogenic bone marrow transplandine and flow cytometry. Cancer Res 1988,48,6238- 6245.
tation (ABMT) in first remission acute myeloblastic leukemia
32. Girino M, Riccardi A, Danova M, et al. Immunocytochemical
(abstr.). Third International symposium on minimal residual disease
evaluation of proliferative activity in human brain tumours. Anal
in acute leukemia, Rotterdam, 1990,28.
Cell Path01 (in press).
Cassileth PA, Begg CB, Bennet JM, et al. A randomized study of
33. Girino M, Cuomo A, Danova M, Buttini R, Giordano M, Riccardi
the efficacy of consolidation therapy in adult acute non lymphocytic
A. Ki 67 expression and BUDR-labeling index in acute non
leukemia. Blood 1984,63,843- 847.
lymphoid leukemias (abstr.). Cell Tissue Kinet 1989, 22 (Suppl. 2),
Biichner W, Hiddemann M, Koeningsmann M, et al. Human
133.
recombinant granulocyte macrophage colony stimulating factor
(GM-CSF) for acute leukemias in aplasia and at high risk of early
death (abstr.). Haematologica 1988,73 (Suppl.), 41.
Acknowledgements-This
research was supported by C.N.R.
Muhn M, Andreeef M, Geissler K, et al. Rh GM-CSF in combi(Consiglio Nazionale delle Ricerche, Roma, Progetto Finalizzato Oncolnation with chemotherapy-a
new strategy in therapy of acute
ogia, grant no. 88.0084144); by A.I.R.C. (Associazione Italiana per la
myeloid leukemia (abstr.). Third International symposium on miniRicerca sul Cancro, Milano); by I.R.C.C.S. (Istituto di Ricoverco e
Cura a Carattere Scientitico Policlinico San Matteo, Pavia) and by
ma1 residual disease in acute leukemia, Rotterdam, 1990,103.
Fondazione Ferrata-Storti, Pavia.
Lowenberg B, Delwel R, Bot F, Budel L, Salem M, Touw
Eur3 Cancer, Vol. 27, No. 4, pp. 441-147,1991.
Printed in Great Britan
0277-5379/91$3.00
0 1991
+ 0.00
Pergamon
Press plc zyxwvutsrqponm
Long-term Results of the HEAVD Protocol for
Adult Acute Lymphoblastic Leukaemia
Renato Bassan, Raffaele Battista, Anna D’Emilio, Piera Viero,
Patrizia Dragone, Enrico Dini and Tiziano Barbui zyxwvutsrqponmlkjihgfedcbaZYXWV
Between 1979 and 1987,82 adults (age 14-71 years) with acute lymphoblastic leukaemia (ALL) were treated with
a i-course protocol called HEAVD, the main feature of which was the early postremission administration of
escalating doses of doxorubicin (total 405 mg/m*) and cyclophosphamide (total 2.5 g/m*). A complete remission
(CR) was attained in 66 patients (80%, 95% confidence intervals, [CI] 71%-89%). Factors affecting favourable
CR achievement were age < 60 years and absence of lymphadenopathy-hepatosplenomegaly
at presentation
(P < 0.05). Median duration of CR was 27 months. 26 patients remain in first continuous and unmaintained CR,
18 of whom between 5.9 and 11.1 years, for an estimated 39% prolonged disease-free survival (95% CI 27%-Q%).
CR duration correlated significantly with absolute blast cell count (15 x lo911or less compared to more) and age
(30 years or under compared to over). Overall, 29 patients are alive with a median follow-up of 6.7 years, the
projected long term survival being 35% at 11 years (95% CI 24%46%). Treatment-related toxicity included 1
lethal case of L-asparaginase-related thromboembolism and 3 toxic deaths among 66 CR patients. Late-onset
toxicity was not observed in long-term survivors. The relatively late occurrence of endpoint events (relapse and
death) in adult ALL confirms that long-term updating is necessary to determine the curative potential of modern
chemotherapy programs for the disease.
EurJ Cancer, Vol.
zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
27, No. 4, pp. 441-447,1991
INTRODUCTION zyxwvutsrqponmlkjihgfedcbaZYXWVUTSRQPONMLKJIHGFEDCBA
subsequently relapse and eventually die [ 11. Since with modern
in adults is a rare and
treatment strategies a CR duration of 18-24 months is not
most often fatal neoplastic disease. Although as many as 80% of
unusual and systemic relapses occur as late as the fourth or fifth
patients may initially achieve a complete remission (CR), most
year of observation [l], clinical studies with a median follow-up
period extended beyond 5 years are needed if the impact of a
potentially curative therapeutic
approach is to be properly
Correspondence to T. Barbui.
R. Bassan, P. Viero and T. Barbui are at the Divisione di Ematologia,
assessed.
Ospedali Riuniti, Largo Barozzi 1, 24100 Bergamo; and R. Battista, A.
Starting in 1979, we have conducted an open uncontrolled
D’Emilio, P. Dragone and E. Dini are at the Divisione di Ematologia,
study
in adult ALL employing a regimen akin to HEAVD
Ospedale Civile, Vicenza, Italy.
from St Bartholomew’s
Hospital (SBH, London,
UK) [2],
Revised 5 Dec. 1990; accepted 17 Dec. 1990.
ACUTE LYMPHOBLASTICLEUKAEMIA(ALL)
�
 monica giordano
monica giordano